

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Total hip arthroplasty (THA) was first introduced by Sir John Charnley in the 1960s, and has been accepted as the most common surgical procedure used worldwide for the management of hip-joint diseases1). A cemented femoral stem used for THA in the early period achieved firm fixation; however, this approach was associated with high rates of revision surgery due to complications at long-term follow-up (e.g., aseptic loosening and severe osteolysis around cemented components) and was also associated with fatal complications caused by fat embolisms and bone cement embolisms23). For these reasons, beginning in the early 1980s, cementless femoral stems were developed with the goal of improving biomechanical fixation; since their development, these stems have been widely used4). Many attempts have been made to develop and manufacture femoral stems in Korea and in 2006, the Bencox® hip stem (Corentec, Seoul, Korea) became the first total hip prosthesis domestically commercialized. The authors of this study aimed to verify the stability and efficacy of the Bencox® hip system by reviewing a consecutive series of 1,000 cementless hip arthroplasties using the Bencox® hip stem5).
Go to : 
MATERIALS AND METHODS
1. Materials
A consecutive series of 1,000 THA performed using the Bencox® hip stem by a single surgeon between September 2006 (following its approval) and July 2014 were included in this study. Since a wide range of patients of different ages, bone qualities and muscle strengths were included in the study; an analysis of those patients at the same time may not obtain meaningful results. Patients were classified into groups based on reason for surgery (i.e., fracture, osteoarthritis [OA], avascular necrosis [AVN] and re-operation). This study reviewed medical and test records for a retrospective analysis of patients and was approved by the institutional review board of our institution (IRB No. CHAMC 2017-11-017).
Breakdown of patient groups is as follows: OA (n=155), AVN (n=209), and fracture including femoral neck, intertrochanteric femur and other fractures (n=552). Bipolar hemiarthroplasty was performed in most cases and THA was done in some patients. Revision surgery was carried out in 84 cases. The re-operation group included patients who underwent surgery for aseptic loosening, periprosthetic fracture and conversion THA after THA infection. As shown in Table 1, of the patients included in this study, 616 were followed up for a minimum of one year (mean, 54.8 months; range, 12–309 months).
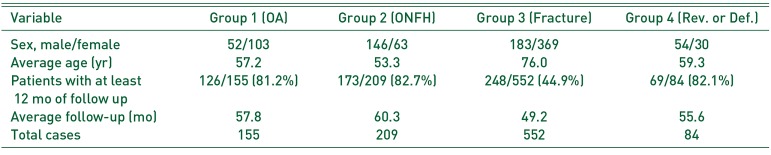
Table 1
Material (Patient) information & follow up period of group
![]()
The Bencox® hip stem used in this study is the first artificial hip arthroplasty implant developed in Korea. The Bencox® hip stem design has a straight, double-tapered, wedge shape figure with a rectangular-shaped cross-section and no collars, and three vertical ribs in the lateral aspect of the proximal body of the stem. This stem has adopted a trapezoidal neck design patented in the United States. to offer increased range of motion (ROM) of the femoral neck, and is made of titanium alloy (Ti6Al4V) and treated with micro arc oxidation (MAO)-blasted surface coating to maximize bone ongrowth6) (Fig. 1). In THA, the Bencox® cup is coated with titanium plasma spray on the surface and hemisphere-shaped, and three screw holes are anatomically designed for more effective fixation. Since the Bencox® hip system was first manufactured in September 2006, the offset was increased in 2009 and the stem shoulder edge was chamfered for easy insertion. In the current study, arthroplasties were performed using the initial design (n=296) and the modified design (n=704). However, since these two stem systems were fundamentally the same, we did not analyze them independently.
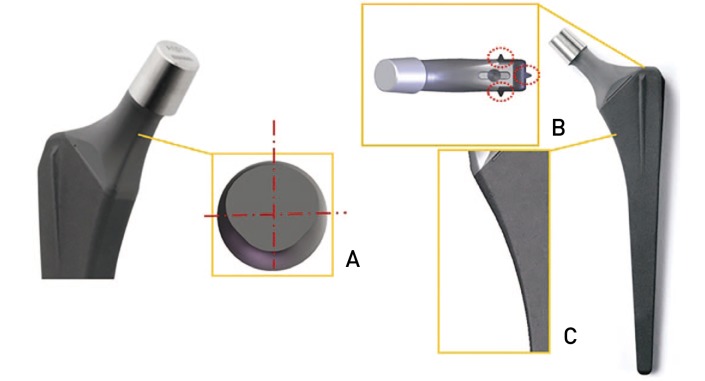 | Fig. 1Bencox® (Corentec, Seoul, Korea) cementless femoral stem design, straight, rectangular, double wedged, tapered, titanium-alloy stem with a rough, grit-blasted surface. Note the smaller neck diameter (A), three vertical ribs in the stem shoulder area (B) and anatomical contour medial-proximal portion (C).
|
All operations were performed by a single surgeon via a transgluteal approach with patients in the supine position. For anatomical reconstruction, the height of the greater trochanter was determined based on the distance from the center of femoral head and the lesser trochanter (head-lesser trochanter distance)7). Given the possibility of lesser trochanter fracture in fracture patients, insertion of the femoral component was carried out by measuring the distance from the tip of the fracture to the center of the femoral head by adding fragment size and head-lesser trochanter distance measured preoperatively. The size of the rasp was gradually increased according to the measured values before surgery to expand the canal, and the stem size was determined for firm fixation. After insertion of the femoral stem, a trail head was placed. After temporary reduction, adequate leg tension was determined by measuring leg length discrepancy.
Since the lesser and greater trochanters are important muscle insertion points within the hip, anatomical reconstruction and firm fixation of the trochanters are crucial for postoperative function. For this reason, fixation was additionally carried out with a candy-package wiring technique originally designed by the authors in cases with lesser trochanter fractures89). Since the fracture line of the greater trochanter runs more in the coronal plane, reduction of bone fragments were performed after insertion of the femoral stem. Fragments were then fixed firmly using cables and wires to help achieve stability10).
Prophylactic antibiotics were administered immediately and for 3 to 5 days after surgery. On the second or third postoperative day, the Hemovac drain was removed and partial weight bearing ambulation using crutches was allowed. Total weight bearing ambulation was allowed from the fourth or sixth postoperative week.
2. Methods
Radiographic examinations were performed during the patient's hospital stay, 6 weeks, 3, 6 and 12 months after surgery and annually. Evaluations were conducted based on clinical outcome indicators including Harris hip scores (HHS), postoperative thigh pain, and complications (e.g., infection and dislocation). Radiographic assessment was carried out based on anteroposterior (AP) and lateral X-rays of the hip and radiographic appearance of endosteal bone ongrowth on both AP and lateral views, osteolysis and subsidence. Bone ongrowth was determined by gross observation of bone-bridge formation that indicates bone growth at the border between the femur and an implant and on the stem surface. The presence of osteolysis was confirmed with cortical reaction to the femoral stem. The stability of the femoral stem was determined with subsidence. Subsidence of the stem was determined by measuring the distance from the tip of the greater trochanter to the shoulder of the femoral prosthesis (superior lateral aspect of the proximal body of the stem). If the distance increased by more than 5 mm in sequential radiographs taken immediately after surgery and at the final follow-up, it was considered as a significant subsidence. The severity of heterotopic ossification was evaluated according to the Brooker classification11). Radiographic evaluations were independently conducted by three orthopedic surgeons who had not participated in any surgery.
HHS were measured to evaluate clinical outcomes. HHS was calculated in 175 cases, and hips with a score of >90 points were considered an excellent result, 80 to 90 points defined as a good result, 70 to 80 points as fair, and <70 points as poor.
Go to :
RESULTS
1. Clinical Results
Postoperative laboratory exam, blood chemistry, and infection and medical findings in immunologic tests revealed no abnormal findings. The results of the HHS measurements are as follows, excellent (n=126), good (n=32), fair (n=14) and poor (n=3); the average HHS at the final follow-up was 95.5–a score in the excellent range (Table 2). No complications were observed (e.g., stem breakage, ceramic breakage, dislocation).

Table 2
Summary of Clinical Outcome (i.e., Harris hip score)
![]()
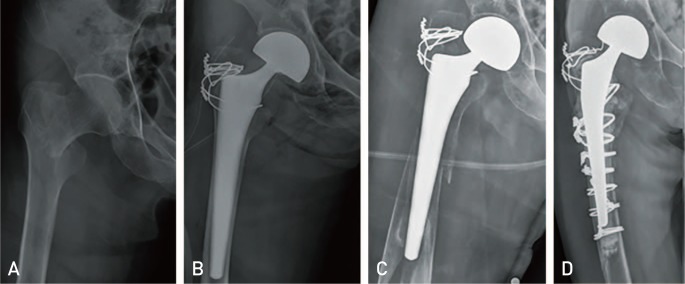
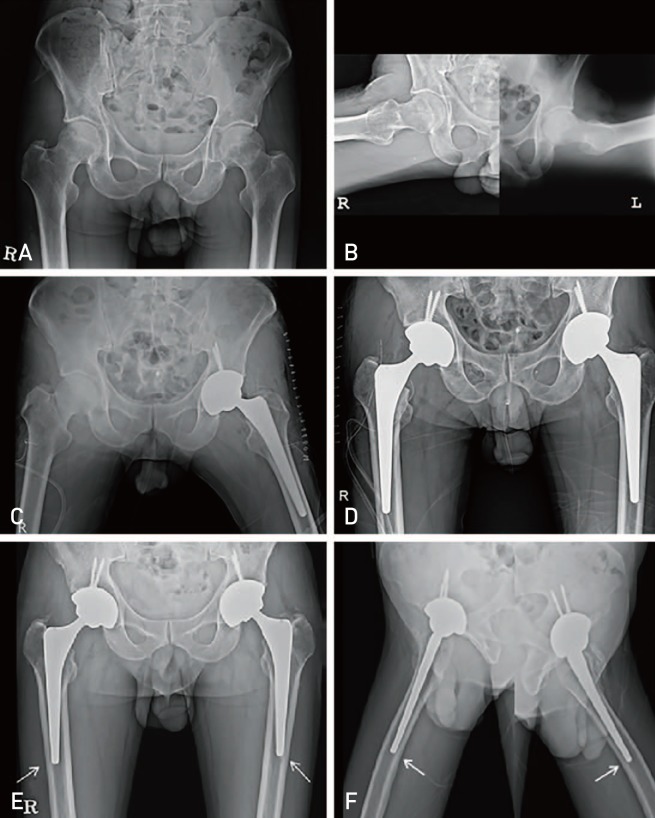
Stem subsidence or aseptic loosening was not seen postoperatively. Periprosthetic fractures were determined by using the Vancouver classification. A total of 19 patients had a periprosthetic fracture. A hip classified as Vancouver type A was managed with cable fixation. The 9 hips classified as Vancouver type B1 were managed as follows: cable fixation (n=5), open reduction and internal fixation with plate (n=3), and conservative treatment due to old age and poor systemic condition (n=1). Of 2 cases classified as Vancouver type B2, 1 had a stem change with a longer stem and the other case received a cemented stem change due to poor bone quality around the prosthesis (Fig. 2). Seven hips were classified as Vancouver type C, and bone union was achieved with open reduction and internal fixation with plate. No patients experienced complications (e.g., postoperative dislocation, infection, complaints of persistent hip pain).
2. Radiological results
Bony ongrowth around the femoral component was observed in 235 (94.8%) of 248 patients in the fracture group, 120 (95.2%) of 126 in the OA group, 166 (96.0%) of 173 in the AVN group, and 64 (92.8%) of 69 in the reoperation group. Of the 616 patients who were followed up for a minimum of 1 year, 585 (95.0%) experienced bony ongrowth. Although there was variation in the healing time of fractures, bone ongrowth occurred between 6 months and 1 year postoperatively and observed mainly in the intermediate and distal regions of the femoral component. Bony ongrowth is easily visible in the radiographs where the femoral stem and femoral bone are in contact with each other.
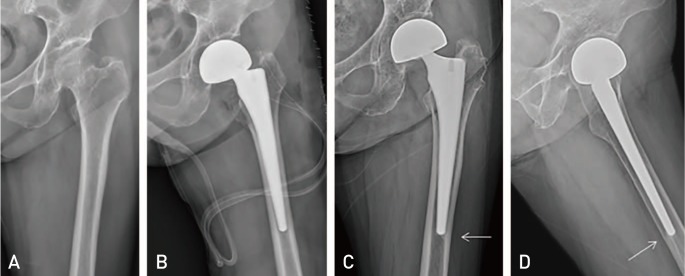
On hip AP X-ray, bony ongrowth was easily visible within the mediolateral region, and Hip lateral X-ray bony ongrowth was well founded in the posterior aspect of the distal region (Fig. 3). No patients experienced osteolysis affecting stem stability and vertical subsidence of the femoral stem. Some cases had varus insertion less than 5°; however, in all cases, these patients achieved stable bony fixation with no specific findings (Fig. 4). There were 2 cases of heterotopic ossification. The first was Brooker class II heterotopic ossification that occurred after surgery; however, no reduction in ROM was observed. The other patients experiencing heterotopic ossification were classified as Brooker class IV; ROM returned following ossification excision surgery.
Go to :
DISCUSSION
In THA, the femoral stem should be selected according to patient's diagnosis, BMD and shape of the femur. The use of a cemented stem allows early ambulation by obtaining initial firm fixation121314). However, cardiovascular complications have been associated with this approach (e.g., intraoperative fat embolism, bone cement embolism, vasodilation due to autonomic reflex); additionally, failure of biologic fixation, thigh pain, stress-shielding, bone resorption and loosening, and difficulty of stem extraction in revision surgery have been reported at both mid- and long-term follow-up1516). Cortical atrophy, proximal stress-shielding, bone loss and other problems produced in early-designed cemented femoral stems have been reported to be significantly associated with cylindrical shape and extensive porous coating of a stem1718). To help overcome these potential complications, many studies have been performed using cementless femoral stems, and tapered cementless femoral stems are now widely used in THA.
The Bencox® hip system used in this study is the first cementless femoral stem developed and manufactured in Korea. We reviewed the results of a consecutive series of 1,000 cementless hip arthroplasties utilizing the Bencox® hip stem and report favorable clinical and radiological outcomes in all patient groups encountered. In particular, no stem failure caused by subsidence or aseptic loosening occurred–a satisfactory result. Moreover, bony ongrowth was shown in 95.0% of patients (585 of 616 cases) with follow up for at least one year. Our previous 5-year follow-up study revealed good results of the Bencox® stem (e.g., excellent bone ongrowth rates [86.6% in the fracture group, 99.6% in the OA group without subsidence or complications requiring revision operation])19). In another study, 78% of patients with an unstable intertrochanteric fracture experienced restoration of their ambulation ability to a pre-injury state, and the combined use of wiring fixation has been described to help obtain support in the posterolateral aspect including the lesser trochanter510). These results compare favorably to the long-term follow-up results of a study involving the Cementless Spotorno (CLS; Protek AG, Berne, Switzerland) stem and Zweymüller stem (Alloclassic; Sulzer Orthopedics, Basel, Switzerland) that resemble the tapered wedge design and blasted surface coating of the Bencox® hip stem. Cruz-Pardos et al.20) reported that the survival rate of Zweymüller stems was 95.9% at a minimum follow-up of 25 years. Furthermore, CLS stem had a survival rate of 98.5% at an average follow-up of 17 years in a study of Müller et al.21) and bone ongrowth at 93.6% and a survival rate of 100% at an average follow-up of 17 years and 3 months in a previous study by this group22). The results achieved seem to be attributed to the unique design and features of the Bencox® hip stem. A Bencox® hip stem is straight, double wedged and tapered with a rectangular cross-section and designed to achieve press-fit at the metaphysis and initial rigid compression reduction in the femoral intramedullary canal by increasing axial and rotational stability within the cylindrical shape of the medullary cavity. Solid fixation can be obtained in patients with arthritis and in elderly patients with hip fractures8). The stem with three vertical ribs on its proximal end improves early rotational stability, and this design can prevent stress shielding with no contact to the distal cortex by increasing proximal stability and surface contact rate and help preserve the femur bone stock. In addition, the slim diaphyseal part– designed to not fill the distal medullary cavity–reduces stress shielding and induces bone ongrowth on all surfaces. In this study, we report a high bone ongrowth rate of 94%.
Haentjens et al.23) suggested that bipolar hemiarthroplasty in the elderly with intertrochanter femur fracture significantly reduced the occurrence of cardiovascular complications by allowing early ambulation compared to open reduction internal fixation (ORIF). In the current study, the high bone ongrowth rate in the fracture group implies that the femoral stem is maintaining good fixation in the hip. Although surgeons may hold different opinions about what type of surgery to perform, we think that cementless THA could be an appropriate surgical option (along with ORIF) for the management of osteoporotic fractures occurring in elderly patients.
No patients in the current study complained of hip pain after surgery. This outcome, comparable to previous findings, is thought to be attributable to the fact that the stem with a tapered design serves a critical role in more evenly distributing weight load to the proximal and distal femur, thus providing a gradual decrease of stiffness from the proximal to the distal regions. Moreover, osseointegration, rigid fixation at the proximal portion, anatomical reduction of fracture fragments of the greater and lesser trochanters2425), and a surgical procedure of adjusting leg length discrepancy by checking adequate stress on the legs in a trial reduction after stem insertion seem to reduce pain and limping.
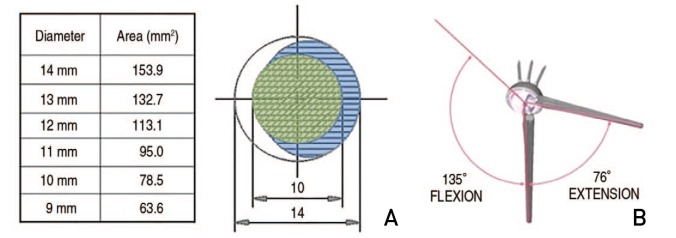
In addition, the surface treatment of the Bencox® hip stem and the unique neck design with an increased head-neck ratio seem to contribute to favorable outcomes. MAO used in surface coating results in numerous porosity structures (diameter of 15µm) that maximize the contacting area with the surrounding bone, assists in adhering the osteoblast and facilitates bone ongrowth. These design features that improve biocompatibility and fixing force provide an excellent environment for bone ongrowth. The Bencox® hip stem is designed with an increased head-neck ratio by reducing a femoral stem neck diameter in order to minimize prosthetic impingement during hip joint motion and a trapezoidal neck design to maintain an optimized neck diameter and minimize neck impingement. This specialized design is expected to be an appropriate hip prosthesis for both Asians with a sedentary lifestyle and Westerners with a standing lifestyle. Since indications for THA have broadened to include active young patients, the Bencox® hip system is expected to meet the worldwide trends of increasing long-term implant survival rates (Fig. 5).
Complications such as infection or dislocation did not occur, and no observed loosening caused by subsidence appears even more impressive. However, periprosthetic fractures occurred in 19 cases. In a comparative study on Vancouver B1 and B2 periprosthetic fractures occurring after well-fixed cementless grit-blasted tapered-wedge stems were used, there was a 4-fold increased rate of Vancouver type B2 fractures (80.4%) compared with Vancouver B1 fractures. In the present study, there were only 9 cases of Vancouver type B1, 2 cases of Vancouver type B2, and 7 cases with Vancouver type C; stem stability was maintained in the majority of patients26). Since fracture type is determined by complex factors including the degree of comminution, the level of bone ongrowth, the onset time of postoperative fracture, bone quality and others, the distribution of periprosthetic fractures may differ despite the use of the same stem. Of 19 patients experiencing periprosthetic fractures, 12 were from the fracture group, perhaps as a result of older age at the time of surgery and poorer bone quality in this group. Moreover, those patients experienced periprosthetic fractures resulting from a simple fall due to poor walking ability before surgery. The poor general health condition of the fracture group is thought to be another cause. Except for two cases that underwent revision of femoral stem change due to periprosthetic fracture, no cases of stem failure caused by subsidence or aseptic loosening was a satisfactory outcome of this study.
There are some notable limitations in this study. Statistical analyses were unable to be performed because it was difficult to establish a control group and select patient groups due to the nature of the study. The number of withdrawals from the study was high due to high mortality rates among older patients. In addition, it was difficult to compare pre- and post-operative conditions because the study involved a large number of fracture patients.
Go to :
CONCLUSION
The Bencox® hip stem is the first developed in Korea and designed as a double wedged, tapered stem which enables rigid fixation and rotational stability and evenly distributed stress as it has almost no stress shielding. Another advantage of the stem is the neck design made to optimize the ROM. Clinical and radiographic evaluations of hip arthroplasty using the Bencox® hip stem revealed excellent outcomes in a consecutive series of 1,000 cementless hip arthroplasties performed in patients requiring surgery for a number of different injuries.
Go to :
 XML Download
XML Download