

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The increasing prevalence of allergic rhinitis (AR) and its management are major challenges for both otolaryngologists and patients around the globe. According to the latest Allergic Rhinitis and its Impact on Asthma (ARIA) guideline 2016 revision,1 AR is characterized by 2 or more nasal symptoms of itching, sneezing, rhinorrhea and obstruction, and affects 10% to 40% of the population. The prevalence of AR has been shown to vary up to 40% in adults2 and 25% in children.3 Although AR is not a life-threatening disease, it reduces patients' quality of life (QoL) in many aspects such as work and school performance, depression, anxiety and sleeping disturbance and imposes a considerable socio-economic burden due to medical costs and lost productivity.14
The management of AR includes avoidance of environmental allergens, pharmacotherapy, and allergen specific immunotherapy (AIT) using modified or unmodified allergen extracts.5 Although the symptoms can be significantly alleviated by pharmacotherapy, the efficacy of treatment is hard to maintain over a long-term without repeated medication. In this regard, AIT including subcutaneous immunotherapy (SCIT) and sublingual immunotherapy (SLIT) is currently the only etiology-oriented treatment available for AR with the potential to alter disease progression,6 which was introduced more than 100 years ago.7
Traditionally, SCIT has been viewed as the golden standard for AIT, although SLIT has emerged as an effective and safe alternative.6 In recent years, there has been accumulating evidence for the efficacy and safety of AIT for AR, with several studies demonstrating both short-term efficacy8910 and long-term efficacy, using mainly SLIT.11121314 However, comparatively few studies have reported on the efficacy of AIT in Chinese AR patients, with the available data documenting the efficacy of SLIT in pediatric and adult AR patients.151617 Thus, this study aimed to compare the long-term efficacy and safety of SCIT in children and adults with AR. As house dust mite (HDM) has been reported to be the most common sensitizing allergen in China,18 the current study investigated primarily the effect of HDM-SCIT.
MATERIALS AND METHODS
Patients
A total of 124 outpatients aged 5 to 51 years with a confirmed diagnosis of AR in accordance with the ARIA criteria19 were enrolled in the study at the Department of Otolaryngology Head and Neck Surgery, Beijing TongRen Hospital. All subjects were recruited over a 2-year run-in period between November 2010 and December 2012, who showed significant nasal symptoms (rhinorrhea, congestion, itching and sneezing), and demonstrated sensitization to HDM according to skin prick test (SPT) ≥ 2+ or specific immunoglobulin (Ig) E ≥ 2+ as measured using the Pharmacia UniCAP system (Thermo Fisher Scientific China Co., Ltd., Shanghai, China).
Patients with severe unstable disease including asthma, active systemic/immunologic disease were excluded as were pregnant women.
Study design
The study was approved by the Ethics Review Board of the Beijing Tongren Hospital and Beijing Institute of Otolaryngology, P.R. China (No. 2010023), and written informed consent was obtained from all participants or guardians of minors before enrolment in the study. Following primary examination, all eligible patients were evaluated on enrolment for baseline total nasal symptom score (TNSS), allergic rhinoconjunctivitis (ARC) daily symptom scores (DSS), daily medication score (DMS), total combined score (TCS)20 and rhinoconjunctivitis quality of life questionnaire (RQLQ) score21 using the different efficacy instruments as described below. All patients then received SCIT for 3 years with standardized extracts of Dermatophagoides pteronyssinus (Der p) (Alutard SQ, ALK company, hørsholm, Denmark). The protocol involved an ‘8-week’ up-dosing (up to 100,000 SQ-U) and a ‘3-year’ maintenance period with injection of allergen at intervals of 6 ± 2 weeks. In total, there were 4 vials of standardized HDM extracts with concentrations ranging from 100 to 100,000 SQ-U/mL, with 1 mL of 100,000 SQ-U containing 9.8 μg Der p1. At the end of SCIT, the patients were evaluated at baseline and then followed up for a period of 2 years, at the end of which the patients again underwent a final evaluation. After 3-years' treatment, patients used only usual medication (antihistamines, topical corticosteroids or oral corticosteroids) if necessary. All data were compared between pediatric subjects (< 14 years old) and adults (≥ 18 years old) based on enrolment date.
SPT
All the participants were instructed not to take any antihistamines or topical steroids for at least 72 hours before the test. Standardized inhalant allergen extracts (Allergopharma GmbH & Co. KG, Reinbek, Germany) were used for SPTs, including 20 allergens, animal dander, trees, grass, cereals, mugwort, dandelion, giant ragweed, Chenopodium album, humulus, locus, Blattella germanica, pine, plantain, Candida albicans, Penicillium notatum, Alternaria tenuis, Aspergillus fumigatus, Dermatophagoides farina (Der f) and Der p. Histamine and saline were used as positive and negative controls, respectively. The diameter of the wheal produced in response to a specific allergen was measured 15 minutes later, and results were expressed as a skin index (SI = mean size of allergen weal/size of histamine wheal).22 The SI was used to further determine the grade of reaction as follows: 0.5 ≤ SI < 1 = grade 2+, 1 ≤ SI < 2 = grade 3+ and SI ≥ 2 = grade 4+. In the present study, grade ≥ 2+ was considered positive.
Efficacy assessment
The efficacy of SCIT was evaluated by assessing symptoms and medication use as below. Nasal symptoms of congestion, discharge, itching and sneezing, as well as eye discomfort were assessed on a 4-point visual analogue scale (VAS) ranging from 0 (asymptomatic) to 3 (very severe).811 TNSS was calculated as the total score of the four nasal symptoms and ranged from 0 to 12 points. ARC DSS was calculated as the sum of TNSS and conjunctivitis scores, with a maximum total score of 15. DMS, ranging from 0 to 6 points, was assessed according to the total daily medicine intake on a 4-point scale, with 0 = “without taking medication”, 1 = “taking antihistamines”, 2 = “taking topical corticosteroids” and 3 = “taking oral corticosteroids”.20 TCS was calculated as the combination of the average score of 6 nasal/conjunctivitis symptoms (rhinorrhea, nasal congestion, itching, sneezing, gritty eyes and watery eyes) and DMS.1020 RQLQ21 was used to evaluate QoL influenced by AR.
Patients were divided into responders and non-responders based on TCS improvement after 3-year treatment of SCIT. In this regard, a 43.9% decrease in TCS was considered the threshold to identify responders as suggested by Zimmer and colleagues.23
Safety assessment
The safety profile was assessed at the time of each injection by documenting adverse events, including local wheals, redness, pruritus and any others. Systemic reactions were classified into 5 grades, ranging from grade 1 (symptoms of 1 organ system present) to grade 5 (death) according to the World Allergy Organization (WAO) criteria.24
Statistical analysis
SPSS statistical software, version 19.0 (IBM Corp., Armonk, NY, USA) was used for data analysis. Descriptive statistics were used for demographic data. The paired t-test was used to evaluate the treatment efficacy and χ2 analysis to evaluate associated factors for efficacy. A P value of < 0.05 was considered statistically significant.
RESULTS
Population characteristics
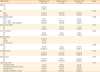
A total of 124 participants eventually completed the 3-year SCIT treatment; of these, 118 (95.2%) completed the follow-up evaluation 2 years after discontinuation of SCIT. The basic demographic characteristics of 118 patients completing the follow-up evaluation are illustrated in Table. These included 44 children (37.3%) and 74 adults (62.7%). The mean age was 9.66 ± 2.60 years in the pediatric group and 33.01 ± 8.62 years in the adult group. The major sensitization patterns were “Der p + Der f” (48, 40.7%) and “Der p + Der f + other allergens” (68, 57.6%). Additionally, 110 patients (93.2%) had no history of smoking, 4 (3.4%) were smokers, and 4 (3.4%) were former smokers. The history of AR before SCIT ranged from 0 to 20 years (3.85 ± 4.23 years). A significantly higher percentage of adults (n = 54; 73%) showed persistent symptoms compared to children (n = 22; 50%). Of the 118 patients, 21 (17.8%) suffered from mild AR and the remaining 97 (82.2%) from moderate-severe AR. Assessment of duration (persistent/intermittent) and severity (mild/moderate-severe) of the disease between adults and children showed that the percentage of adults with persistent symptoms was significantly higher than that of children with persistent symptoms (P = 0.012), while the severity of disease was comparable between adults and children (P = 0.159).
Efficacy assessment
The symptoms and QoL were significantly improved (P < 0.001) in the third year and fifth years compared to the baseline in both groups (Fig. 1). Similarly, DMS was significantly reduced (P < 0.001) by the end of SCIT compared to initiation of immunotherapy. Reduction in DMS was maintained for 2 years after discontinuation of SCIT; however, it tended to be different between the efficacy by the end of the third and fifth years (Fig. 1A and B), especially in nasal congestion and discharge (P = 0.003 and P = 0.001, respectively).
 | Fig. 1Comparison of nasal symptoms (A), TNSS, AR/C DSS, DMS, TCS (B), and RQLQ scores (C) at baseline, and in the third and fifth years (2 years after the discontinuation of treatment). All scores were significantly decreased after the 3-year SCIT (P < 0.001). Statistically significant difference could be observed between the 3-year and 5-year SCIT in nasal congestion, discharge, TNSS, AR/C, DSS, DMS and TCS.SCIT, subcutaneous immunotherapy; TNSS, total nasal symptoms scores; AR/C DSS, allergic rhinoconjunctivitis daily symptom scores; DMS, daily medication score; TCS, total combined score; RQLQ, rhinoconjunctivitis quality of life questionnaire.
*P < 0.001; †P < 0.01.
|
The improvements of TNSS and TCS between baseline and time points at the end of the third year or the end of the fifth year were calculated and defined as TNSSΔ3 and TCSΔ3 and TNSSΔ5 and TCSΔ5, respectively. HDM-SCIT led to significantly greater improvement in TNSS and TCS from baseline to third and fifth year in children compared to adults (TNSSΔ3: 6.66 vs. 5.41, P = 0.011; TCSΔ3: 4.30 vs. 3.83, P = 0.027; TNSSΔ5: 6.16 vs. 4.86, P = 0.037; TCSΔ5: 4.11 vs. 3.62, P = 0.044) (Fig. 2). Comparison of the improvement in TNSS and TCS from the third to fifth years showed that although this was slightly greater in children, this was not significantly different from changes in adults (P = 0.905 and P = 0.849 for changes in TNSS and TCS, respectively).
 | Fig. 2Comparison of improvements in long-term (3-year and 5-year) efficacy of SCIT in children and adults with AR, assessed as a change in TNSS and TCS from baseline to the third and fifth years. Better improvements in both TNSS and TCS were observed from baseline to the end of the third and fifth years in children compared to adults.SCIT, subcutaneous immunotherapy; AR, allergic rhinitis; TNSS, total nasal symptoms scores; TCS, total combined score.
*P < 0.05.
|
Assessment of the factors that might be associated with the maintenance of long-term efficacy of HDM-SCIT showed that duration of AR before SCIT (<10 vs. ≥10 years) was significantly associated with TCSΔ3 (4.12 vs. 3.13, P = 0.036) and TCSΔ5 (3.90 vs. 3.09, P = 0.033), respectively, indicating that a shorter history of AR predisposed an individual to maintain better HDM-SCIT efficacy 2 years after discontinuation of treatment (Fig. 3). In contrast, sex, sensitization pattern and family history were not significantly associated with long-term efficacy.
 | Fig. 3Comparison of improvements in TCS from baseline to the end of the third and fifth years in patients with < 10 years history of AR before SCIT and patients with ≥10 years history of AR.TCS, total combined score; AR, allergic rhinitis; SCIT, subcutaneous immunotherapy.
*P < 0.05.
|
Based on a cutoff value of 43.9% decrease in TNSS after the 3-year SCIT, 98/118 (85.4%) participants were found to be responders to SCIT therapy, achieving efficacy with symptom improvements over the pre-determined threshold value. Among the 20 non-responders, only 3 were children and the remaining 17 were adults. Children were more likely to be responders (P = 0.025). Furthermore, a significant difference was found in the age between responders and non-responders (22.48 vs. 33.25, P = 0.001). However, no significant difference was found in duration (persistent/intermittent) of AR between the responders and non-responders (P = 0.566).
Adverse reactions
Among all the 124 patients who completed SCIT, 10 (8.1%; 7 children and 3 adults) reported local adverse reactions. Similarly, 5 (4.2%; 2 was child and 3 were adults) experienced systemic adverse reactions, with 1 patient experiencing grade 1 reactions and 4 patients experiencing grade 2 reactions. Symptoms in these patients were relieved after taking antihistamines, without requiring epinephrine.
In the final 118 subjects who finished 2-year follow-up, 3 events of systemic side effects were reported. Local adverse effects (pruritus and wheals) were observed in 1 child (2.3%) and 3 adults (4.1%), at least once during the treatment (Table). There was no significant difference between the pediatric and adult groups in adverse reaction rates.
Table
Demographic and survey information on the study population
![]()
DISCUSSION
Since the introduction of AIT into clinical practice by Noon7 more than a century ago, it has now been recognized as the only treatment with considerable long-term efficacy for AR, targeting the aetiology of the disease.25 Although SCIT was considered the golden standard of AIT,6 most studies have employed SLIT rather than SCIT. Furthermore, there is insufficient evidence on the long-term efficacy of SCIT between pediatric subjects and adults. Indeed, comparison of the efficacy of 1-year SLIT using HDM in Korean children and adults demonstrated that although the change in medication scores was greater in children, this difference was not statistically significant.15 In the present study, our findings confirm the long-term efficacy of SCIT with HDM, which is in line with other carry-over findings.13262728 Importantly, for the first time, our study has demonstrated that children with AR tend to achieve better long-term efficacy of HDM-SCIT compared to adults as indicated by significant improvements from baseline values in TNSS and TCS. Although statistical differences could be observed between the efficacy (TNSS, ARC DSS, TCS) at the end of the third year and fifth years, the differences were so small (less than 0.5) that the clinical significance was limited. Assessment of QoL further indicated that all RQLQ domains were also improved from baseline in both children and adults in the third and fifth years.
Our findings of long-term efficacy of SCIT with HDM are in accordance with those of previous studies,111329 two of which assessed the 3-year follow-up efficacy of SCIT. While Tahamiler and colleagues29 suggested remarkable improvements in TNSS and TCS, while Karakoc-Aydiner and colleagues11 demonstrated significant efficacy with respect to TNSS TCS as well as DMS. Sahin and colleagues13 conducted a 10-year follow-up of AR patients after receiving HDM-SCIT and demonstrated that the positive effects of SCIT were maintained even after 10 years. Similarly, our findings for the effect of HDM-SCIT on improvement of QoL are also in accordance with those of previous studies employing SLIT.30
Studies comparing the efficacy of AIT between pediatric and adult patients are limited. A prospective observational study by Soh and colleagues17 indicated that although improvements in medical scores were greater in children than in adults after SLIT, the differences were not significant. In contrast, our study demonstrated that improvements in TNSS and TCS following HDM-SCIT were significantly greater in pediatric AR patients than in adult AR patients. Children with AR tended to have better improvements in the third and fifth years than adults. Comparison between the 3-year and 5-year SCIT to assess its sustained effect after discontinuation of treatments further showed no significant difference between the children and adults.
Adverse effects of AIT can be divided into local and systemic adverse effects. While local adverse effects have been shown to be common in SCIT with a prevalence of 26%-86%31 and often well tolerated,32 systemic adverse effects are less common and of low prevalence of around 3.4%.33 In this retrospective study, the prevalence of local and systemic adverse effects was 15.4% and 3.2%, respectively. All were well tolerated without severe clinical outcomes, thus emphasizing the safety of standard HDM-SCIT in children and adults with AR.
Although much effort has been made in recent years to identify specific biomarkers or clinical criteria to predict patient responsiveness to AIT and when to stop treatment for non-responders no universal standard is currently available for use in clinical practice.3435 Zimmer and colleagues23 have suggested that a 43.9% decrease in average rhinoconjunctivitis total symptom score following AIT may be a suitable threshold to identify clinical responders. Using this criterion, we found a high total response rate, with 85.4% (98/118) patients responding to HDM-SCIT. In our study, children were more likely to be responders (P = 0.025). What is more, we found that patients whose ages were older were more likely to be non-responders, which further strengthened our conclusion. Still, further studies involving a larger sample size are warranted to explore any potential associations between patient age and responsiveness to AIT. Indeed, our finding showed that patients with AR history of more than 10 years less benefit from HDM-SCIT compared to those with AR history shorter than 10 years, suggesting that a younger age and smaller duration of AR may be a good predictor of which patient is likely to respond well to AIT. Although there were more adult patients with persistent symptoms than children in this study, there was no significant difference in duration (persistent/intermittent) of AR between responders and non-responders, suggesting that the difference in the persistent symptoms was unlikely to be responsible for the difference in HDM-SCIT efficacy between children and adults.
Despite the encouraging findings, the present study has some limitations. First, as a retrospective study, SPT results were not available for all patients after discontinuation of SCIT, and thus new onset allergens after the treatment could not be evaluated. Secondly, only symptoms and medical scores were used to assess the efficacy of SCIT, and thus use of some additional objective measures such as IgE, IgG or other cellular biomarkers such as regulatory T cells may have provided additional useful data on the effects of SCIT on these indices.
In conclusion, a 3-year course of HDM-SCIT is a safe, effective, sustainable long-term treatment option in both pediatric and adult patients with AR, although children appear to achieve better long-term efficacy compared to adults. A short history of AR may be a good predictor of higher responsiveness to AIT, and therefore this therapy should be considered at the earliest opportunity in children and adults with AR in order that progression of the disease can be attenuated earlier.
 XML Download
XML Download