

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Lung cancer is the leading cause of cancer-related death in the United States and Korea.12 Among lung cancer cases, adenocarcinoma is the most common histologic type, and many molecular adenocarcinoma subsets have been discovered.3 Certain genetic alterations, such as epidermal growth factor receptor (EGFR) or anaplastic lymphoma kinase (ALK) rearrangement, have distinct histological features and are highly correlated with target therapy response rate.34 For example, ALK-rearranged adenocarcinoma displays a solid-predominant pattern and has mucin-containing cells, while KRAS-mutated adenocarcinoma reveals invasive mucinous adenocarcinoma, that typically shows goblet or columnar cell morphology and abundant intracytoplasmic mucin.4
ALK tyrosine kinase inhibitors (TKIs) are highly effective in patients with ALK-rearranged adenocarcinoma. However, despite the good response to ALK-TKIs, most patients eventually become resistant to the agents. Possible mechanisms of acquired resistance to ALK-TKIs include ALK secondary mutation, ALK amplification, loss of ALK, EGFR activation, c-KIT amplification, KRAS mutation, and insulin like growth factor 1 receptor (IGF-1R) activation.5 Similarly, in EGFR-mutated adenocarcinoma cases, the possible underlying mechanisms include a secondary mutation in EGFR (T790M), human epidermal growth factor receptor 2 (HER2) amplification, MET amplification, overexpression of hepatocyte growth factor, and loss of phosphatase and tensin homolog (PTEN) expression.678 Additionally, histologic transformations, including small cell lung cancer (SCLC) transformations, are suggested as possible mechanisms of ALK- or EGFR-TKI resistance.91011121314
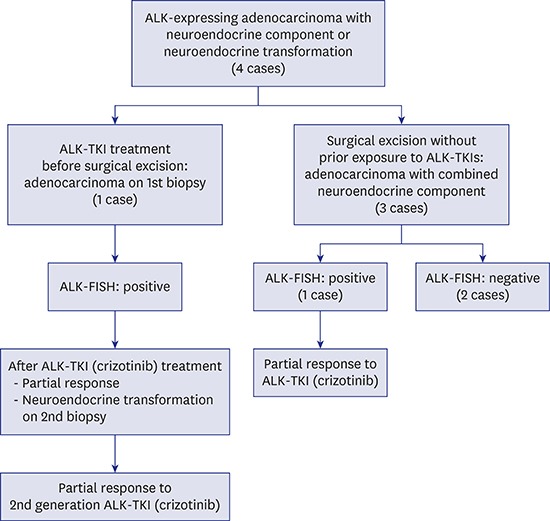
ALK-expressing adenocarcinoma with neuroendocrine differentiation in patients with no TKI therapy has not been reported in the literature. In this study, we describe the clinicopathological features of four ALK-expressing adenocarcinoma cases with combined neuroendocrine component or transformation.
Go to : 
METHODS
Patients and tissue samples
Archived cases from the Department of Pathology, Samsung Medical Center, Seoul, Korea were evaluated. All cases were diagnosed by one experienced pulmonary pathologist. The tumor sections were evaluated after being stained with hematoxylin and eosin. Histologic type, subtype, size, pleural invasion, lymphovascular invasion, perineural invasion, and lymph node metastasis were assessed according to the international tumour, node, and metastasis (TNM) classification system. Clinical data, including age, sex, smoking history, treatment, and clinical course were retrieved from the patients' electronic medical records retrospectively. Patient clinicopathologic parameters are summarized in Table 1.
Table 1
Clinicopathologic characteristics of ALK-rearranged adenocarcinoma with combined neuroendocrine component tumor in this study
ALK = anaplastic lymphoma kinase, ADC = adenocarcinoma, NET = neuroendocrine tumor, IHC = immunohistochemistry, FISH = fluorescence in site hybridization, Recur = recurrence, DFS = disease-free survival, OS = overall survival, LCNEC = large cell neuroendocrine carcinoma, Pos = positive, Ex- = ex-smoker, Neg = negative, ILD = interstitial lung disease, SCLC = small cell lung cancer, FNAC = fine needle aspiration cytology, NSCLC = non-small cell lung cancer, FNAB = fine needle aspiration biopsy, LN = lymph node.
![]()
Immunohistochemistry (IHC)
Representative formalin-fixed, paraffin-embedded (FFPE) tissue sections were used for IHC. These sections were incubated with primary antibodies against CD56 (1:200; Novocastra, Newcastle-upon-Tyne, UK) and ALK (Clone 5A4; Leica, Wetzlar, Germany). Immunohistochemical staining using a biotin-avidin-peroxidase method with BOND-MAX autostainer (Leica) was performed on 3-µm-thick sections from each patient after retrieval with T/E buffer. Nuclei were counterstained with hematoxylin.
EGFR mutation and ALK gene status
Tumor tissues were microscopically dissected from FFPE tissue sections for EGFR mutation detection. Using a DNeasy tissue kit (Qiagen, Helden, Germany), DNA was extracted from the tissue sections according to the manufacturer's instructions. The EGFR mutation status of tumor samples was assessed with the PNA Clamp EGFR Mutation Detection Kit (Panagene, Inc., Daejeon, Korea). For determining ALK gene rearrangement, ALK fluorescence in situ hybridization (FISH) testing was performed using the Vysis ALK Break-Apart Probe kit (Abbott Molecular, Des Plaines, IL, USA).
Ethics statement
The present study protocol was reviewed and approved by the Institutional Review Board of Samsung Medical Center (IRB File No. 2017-08-110). Informed consent was waived for individual participants included in the study given the retrospective nature of this work.
Go to :
RESULTS
Histologic features, ALK and EGFR status of each cases
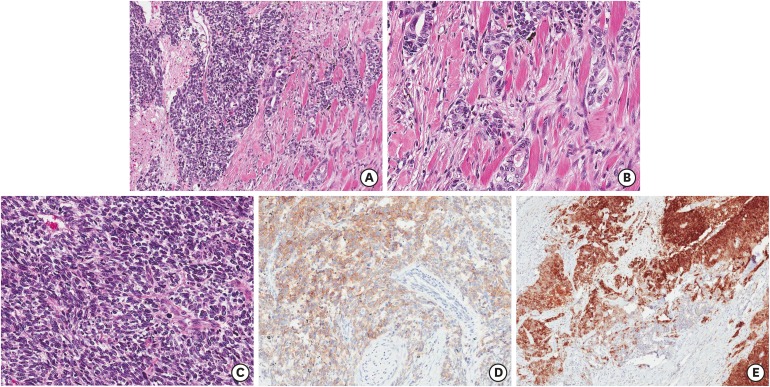
Case 1 was a 73-year-old female never-smoker who presented with an incidentally found lung mass. She underwent a lobectomy of the right upper lobe without neoadjuvant treatment. The lung mass was 2.8 cm and appeared to be comprised of acinar-pattern adenocarcinoma (30%) and large cell neuroendocrine carcinoma (70%) (Fig. 1A and B). The perihilar lymph node was involved in the tumor (pT1bN1 by 7th edition American Joint Committee on Cancer/International Union Against Cancer (AJCC/UICC) cancer staging system). Clinically distant metastasis was not present. On immunohistochemical evaluation, the adenocarcinoma component of the tumor was positive for thyroid transcription factor-1 (TTF-1) (image not included) and ALK (Fig. 1C), but negative for CD56 (Fig. 1D). The large cell neuroendocrine component of the tumor was positive for TTF-1 (image not included), ALK (Fig. 1C), and CD56 (Fig. 1D). Break-apart signals were detected on an ALK FISH test (Fig. 1E). An EGFR mutation was not detected. After 157 days without adjuvant therapy, the patient had multiple lymph node metastases, peritoneal seeding, adrenal metastasis, and bone metastasis in the right humerus, as shown on positron emission tomography-computed tomography (PET-CT). Endobronchial ultrasound-guided transbronchial needle aspiration biopsy (EBUS-guided TBNA) was performed and metastatic carcinoma, mainly consisting of large cell neuroendocrine carcinoma, was present. After diagnosis, the patient received chemoradiation therapy and crizotinib administration and a partial response was noted after two months. She was then lost to follow-up due to personal reasons.
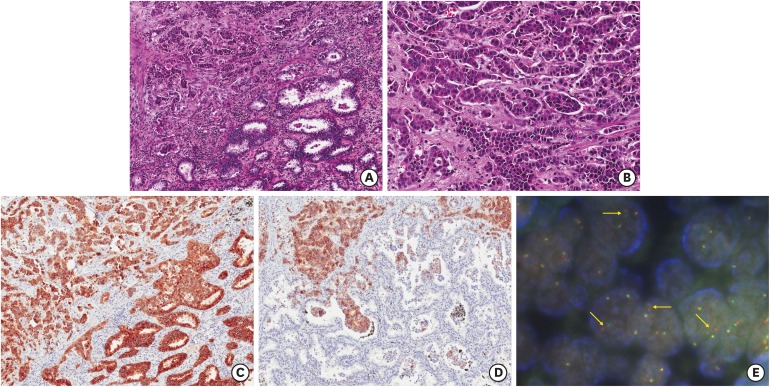 | Fig. 1Histologic finding, immunohistochemical results and ALK FISH study of case 1. The tumor shows acinar-pattern adenocarcinoma (A, ×100, right lower) with combined large cell neuroendocrine component (A, left upper; B, ×200). Both components are positive for ALK immunohistochemically (C, ×100). However, only large cell neuroendocrine component reveals CD56-positivity (D, ×100). The tumor shows break-apart signal pattern on ALK FISH study (E).
ALK = anaplastic lymphoma kinase, FISH = fluorescence in situ hybridization.
|
Case 2 was a 73-year-old male patient who was diagnosed with idiopathic pulmonary fibrosis (IPF). He was an ex-smoker with a 40-pack-year history and was diagnosed with interstitial lung disease on low-dose chest computed tomography (CT) during a health examination. During follow-up, a 2.5-cm mass and a nodular lesion were found in the right middle and lower lobes, respectively. He underwent bilobectomy of the right middle and lower lobes. Two masses were noted and the larger one measured 3.5 cm at its greatest diameter. Hilar, interlobar, and lobar lymph nodes were involved in the tumor (pT3N1 by 7th edition AJCC/UICC cancer staging system). Clinically distant metastasis was not observed. On microscopic examination, the tumor was poorly differentiated, solid-pattern adenocarcinoma, which displayed diffusely large cell neuroendocrine differentiation (Fig. 2A and B). The poorly differentiated adenocarcinoma components of the tumor were positive for ALK and focally positive for CD56 (Fig. 2C and D). The neuroendocrine differentiated component showed ALK- and CD56-positivity (Fig. 2C and D). Break-apart signal was not detected on an ALK FISH test (Fig. 2E). No EGFR mutation was detected. While there was no evidence of disease recurrence noted on follow-up, the patient died three months later due to IPF progression.
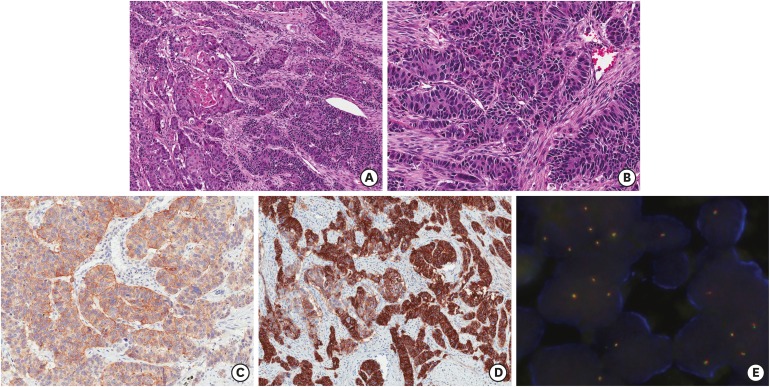 | Fig. 2Microscopic finding, immunohistochemical results, and ALK FISH study of case 2. The tumor displays poorly differentiated solid-pattern adenocarcinoma (A, ×100, left; B, ×200) with combined large cell neuroendocrine component (A, right; B, ×200). Both components have ALK immunoreactivity (C, ×100). Only large cell neuroendocrine component reveals strong CD56-positivity (D, ×100). However, both components examined with ALK break-apart FISH rearrangement probe kit are negative (E).
ALK = anaplastic lymphoma kinase, FISH = fluorescence in situ hybridization.
|
Case 3 was a 64-year-old male who was a current-smoker with a 60-pack-year smoking history. A mass in the left upper lobe was identified during a low-dose chest CT. He underwent a lobectomy of the left lower lobe. The resected specimen was a 2.2-cm mass with multiple satellite small nodules that were comprised of combined adenocarcinoma (10%) and SCLC (90%) components. The left lower paratracheal and subaortic lymph nodes were involved in the tumor (pT3N2 by 7th edition AJCC/UICC cancer staging system). Clinically distant metastasis was not observed. On microscopic examination, the tumor appeared to be composed mostly of SCLC (90%) with focal acinar- and solid-pattern adenocarcinomas (Fig. 3A-C). Tumor cells were positive for ALK (Fig. 3D) and CD56 (Fig. 3E). Break-apart signal was not shown on an ALK FISH test (image not included). No EGFR mutation was shown. After surgery, the patient was given a standard SCLC chemotherapy regimen. The tumor metastasized in multiple T- and L-spine bones after 243 days, and to the brain thereafter. He was eventually lost to follow-up.
 | Fig. 3Histologic finding and immunohistochemical results of case 3. The tumor reveals acinar-pattern adenocarcinoma (A, ×100, right; B, ×200) with combined small cell neuroendocrine component (A, left; C, ×200). These both components are positive for ALK immunohistochemically (D, ×100). However, only large cell neuroendocrine component shows CD56-positivity (E, ×100). Break-apart signal was not shown on an ALK FISH test (image not included).
ALK = anaplastic lymphoma kinase, FISH = fluorescence in situ hybridization.
|
Case 4 was a 35-year-old female, a never-smoker who presented with left chest pain and dyspnea. A left pleural effusion and pleural multifocal nodularity were discovered with no definite lung parenchymal lesions on a chest CT taken during her initial work-up. Metastatic non-SCLC (NSCLC) was present on pleural fluid aspiration cytology. Palliative chemotherapy with pemetrexed and cisplatin was initiated. After showing a partial response and subsequent progression, palliative target therapy with gefitinib was administered, but the same combined response, partial response and subsequent progression was observed. Re-biopsy of the left axillary lymph node was done, and the lymph node revealed metastatic adenocarcinoma (Fig. 4A). The tumor cells were positive for ALK immunohistochemically (Fig. 4B), and an ALK FISH test was performed. The FISH test revealed break-apart signals (Image not shown). An EGFR mutation was not detected. Thereafter, target therapy using ALK-TKI with crizotinib was administrated. After partial response and progression, palliative radiotherapy was begun. Re-biopsy of the right supraclavicular lymph node was done, and the tumor cells displayed neuroendocrine morphology without typical adenocarcinoma (Fig. 4C). This tumor cells were positive for CD56 (Fig. 4D). The possibility of transformation to neuroendocrine carcinoma as a resistance mechanism to ALK-TKI was suspected. She underwent radiation therapy and was administrated another ALK-TKI-ceritinib regimen. She displayed a partial response to the ceritinib treatment, and was still alive six years later.
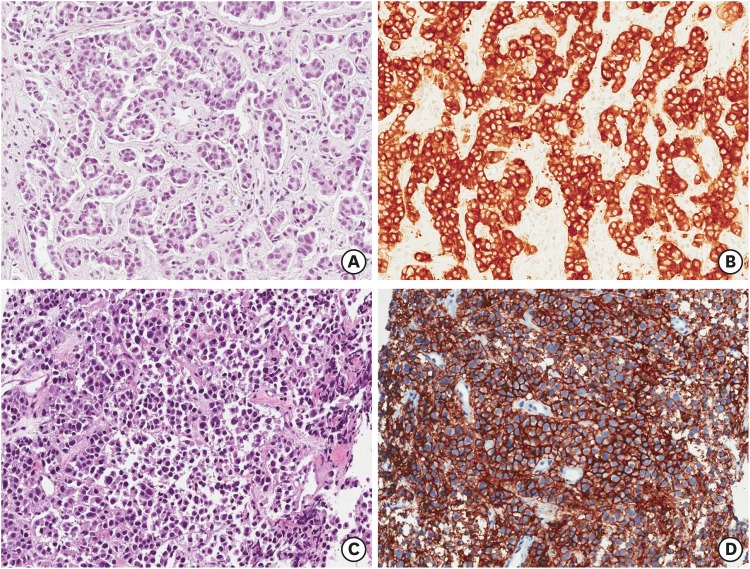 | Fig. 4Microscopic finding and immunohistochemical results of case 4. Second biopsied specimen consists of poorly differentiated solid and acinar-pattern adenocarcinoma (A, ×200) and displays ALK-positivity (B, ×200). The tumor showed break-apart signal pattern on ALK FISH study (image not included). After ALK-TKI (crizotinib) administration, third biopsied tumor reveals solid and sheet pattern tumor with neuroendocrine differentiation (C, ×200). And it reveals also ALK-positivity and CD56-positivity (D, ×200).
ALK = anaplastic lymphoma kinase, FISH = fluorescence in situ hybridization, ALK-TKI = anaplastic lymphoma kinase tyrosine kinase inhibitor.
|
Go to :
DISCUSSION
Histologic transformations, such as small cell transformations and large cell neuroendocrine transformations, lead to resistance to EGFR- or ALK-TKIs.91011121314 Herein, we reviewed four cases of ALK expressing adenocarcinoma with combined neuroendocrine component or neuroendocrine transformation. Three cases of them underwent lobectomy without administration of ALK-TKI, and one received ALK-TKI (crizotinib) after diagnosis with biopsied sample. These tumors were positive for ALK immunohistochemically. However, two of four cases were identified break-apart signals on ALK FISH study. These two patients displayed a partial response to the ALK-TKI treatment.
The standard test for ALK rearrangement in NSCLC is break-apart FISH study. Recently, several study using ALK 5A4 and D5F3 (Cell Signaling; Ventana, Tucson, AZ, USA) clones has already demonstrated to correlate between IHC and FISH.15161718 As a result, the sensitivity of IHC with two antibodies was more than 90%, the specificity was more than 97%.151617 Moreover, ALK IHC method using Ventana ALK IHC (D5F3 clone) is also Food and Drug Administration approved companion diagnostics.17 Among the 4 cases we reported, two cases showed discrepancy. Interestingly, these tumors were not entirely adenocarcinoma, but were accompanied by a neuroendocrine component and CD56 immunoreactivity was expressed in the neuroendocrine component. Further studies are needed to determine whether the combined neuroendocrine component is caused by ALK immunoreactivity.
To date, histologic transformations, such as neuroendocrine differentiation, small cell changes, or sarcomatoid changes in ALK-rearranged adenocarcinoma, have been reported in seven patients.10141920212223 The clinicopathologic parameters of these patients are summarized in Table 2. Only one patient (case 7) underwent an initial lobectomy, while the six other patients were biopsied. Histologically, all cases were diagnosed with adenocarcinoma. The result of ALK immunohistochemical staining for case 8 was not recorded. The tumors of the other patients were all positive for ALK immunohistochemically. The ALK FISH test results for all cases revealed break-apart signals. All patients had chemotherapy and underwent ALK-TKI administration. After treatment, one showed neuroendocrine differentiation (case 5) while another revealed a sarcomatoid change (case 11), and five others displayed small cell carcinoma or small cell carcinoma-like morphologies (case 6–10).
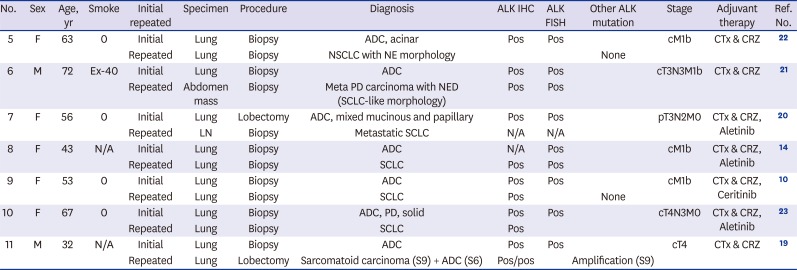
Table 2
Clinicopathologic features of histologic transformation of ALK-rearranged adenocarcinoma after ALK-TKI administration in the literature
| No. | Sex | Age, yr | Smoke | Initial repeated | Specimen | Procedure | Diagnosis | ALK IHC | ALK FISH | Other ALK mutation | Stage | Adjuvant therapy | Ref. No. |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 5 | F | 63 | 0 | Initial | Lung | Biopsy | ADC, acinar | Pos | Pos | cM1b | CTx & CRZ | 22 | |
| Repeated | Lung | Biopsy | NSCLC with NE morphology | None | |||||||||
| 6 | M | 72 | Ex-40 | Initial | Lung | Biopsy | ADC | Pos | Pos | cT3N3M1b | CTx & CRZ | 21 | |
| Repeated | Abdomen mass | Biopsy | Meta PD carcinoma with NED (SCLC-like morphology) | Pos | Pos | ||||||||
| 7 | F | 56 | 0 | Initial | Lung | Lobectomy | ADC, mixed mucinous and papillary | Pos | Pos | pT3N2M0 | CTx & CRZ, Aletinib | 20 | |
| Repeated | LN | Biopsy | Metastatic SCLC | N/A | N/A | ||||||||
| 8 | F | 43 | N/A | Initial | Lung | Biopsy | ADC | N/A | Pos | cM1b | CTx & CRZ, Aletinib | 14 | |
| Repeated | Lung | Biopsy | SCLC | Pos | Pos | ||||||||
| 9 | F | 53 | 0 | Initial | Lung | Biopsy | ADC | Pos | Pos | cM1b | CTx & CRZ, Ceritinib | 10 | |
| Repeated | Lung | Biopsy | SCLC | Pos | None | ||||||||
| 10 | F | 67 | 0 | Initial | Lung | Biopsy | ADC, PD, solid | Pos | Pos | cT4N3M0 | CTx & CRZ, Aletinib | 23 | |
| Repeated | Lung | Biopsy | SCLC | Pos | |||||||||
| 11 | M | 32 | N/A | Initial | Lung | Biopsy | ADC | Pos | Pos | cT4 | CTx & CRZ | 19 | |
| Repeated | Lung | Lobectomy | Sarcomatoid carcinoma (S9) + ADC (S6) | Pos/pos | Amplification (S9) |
ALK = anaplastic lymphoma kinase, TKI = tyrosine kinase inhibitor, IHC = immunohistochemistry, FISH = fluorescence in site hybridization, Ref. = Reference, ADC = adenocarcinoma, Pos = positive, CTx = chemotherpy, CRZ = crizotinib, NSCLC = non-small cell lung cancer, NE = neuroendocrine, Ex- = ex-smoker, Meta = metastatic, PD = poorly differentiated, NED = neuroendocrine differentiation, SCLC = small cell lung cancer, LN = lymph node, N/A = not available.
![]()
However, in this study, three cases had ALK-expressing adenocarcinoma with combined neuroendocrine component and no history of ALK-TKI administration. These findings suggest that ALK-expressing adenocarcinoma may involve combined neuroendocrine carcinoma or neuroendocrine differentiation. However, only one case of three revealed break-apart signal on ALK FISH study. No cases of ALK-rearranged adenocarcinoma with neuroendocrine carcinoma without ALK-TKI therapy were reported. Recently Le et al.24 reported that a patient without EGFR-TKI was diagnosed with EGFR-mutated adenocarcinoma and then later experienced transformation to squamous-cell carcinoma after chemotherapy. Herein, although the number of cases was too small to draw robust conclusions, a partial response to ALK-TKI was present in a combined ALK-rearranged adenocarcinoma and large cell neuroendocrine carcinoma. Moreover, after small cell transformation as a resistance mechanism for ALK-TKI-crizotinib, a partial response to ceritinib was observed. Further research is needed to identify the clinicopathologic features of these tumors.
In summary, the underlying mechanisms of histologic transformation leading to drug resistance are not well understood. We reported four cases that exhibited ALK-expressing adenocarcinoma with combined neuroendocrine component or neuroendocrine transformation. Three cases did not undergo neoadjuvant chemotherapy or ALK-TKI therapy. The clinical characteristics of these patients are not well understood; thus, further evaluation of more cases is recommended. Finally, sufficient tumor sampling and careful histologic examination is necessary to identify combined ALK-rearranged or EGFR-mutated adenocarcinoma and neuroendocrine carcinoma.
Go to :
 XML Download
XML Download