

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The pace of globalization has rapidly increased with the progress in information and communication technologies.1 With globalization, people from different countries have become multilingual and multicultural,2 resulting in the increased movement of populations internationally.3 According to the United Nations Population Division statistics, the number of immigrants in Korea has grown rapidly from 43,107 in 1990 to 1,327,324 in 2015.4 Considering that the current population of Korea is about 51 million, migrants account for a large proportion.5 Studies claim that globalization may have also led to an increase in the number of international marriages.6 The rate of marriage between Koreans and foreigners has nearly doubled, from 3.5% in 2000 to 7.3% in 2016.7
In 2015, the birth rate of multicultural families accounted for 4.5% of all births in Korea.8 As such, adolescents in multicultural families are likely to be at greater risk for social dysfunction than adolescents in monocultural families.9 For instance, peer relationships could be a particularly common problem for multicultural adolescents because of the uncertainty surrounding racial status, which may lead to behavioral and psychosocial problems such as social isolation and delinquent behavior.91011 Recent studies have consistently reported that multicultural adolescents tend to have more psychological problems than monoracial adolescents.1213 Because adolescence is the period of ego development and self-esteem formation, these psychological issues warrant more attention.14
While industrialization and economic development have brought about significant advances in convenience, deteriorating mental health is becoming an increasingly relevant issue in our competitive modern society.15 The World Health Organization defines health as a state of complete physical, mental, and social well-being and not merely the absence of disease or infirmity.16 Thus, mental health is considered a notable health issue; depression is a particularly important mental health condition.16 In fact, depression is a disease of great burden. A study showed that depression is likely to have the highest disease burden worldwide by 2030.17 In addition, more than 60% of suicides can be attributed to mental health status including depressive disorder and other mood disorders.18 In particular, Korea has the highest suicide rate among Organisation for Economic Co-operation and Development (OECD) countries (29 suicides per 100,000 persons, in 2014).19 Thus, depression and its treatment requires attention.20
Although several studies have investigated depression in adolescents from multicultural families, most of them involved Caucasians, and rarely Asians.21 Thus, the purpose of this study was to investigate whether a significant association exists between the parents' country of birth and adolescent depressive symptoms in a nationally representative sample of South Korean adolescents.
METHODS
Study population
Data from the Korea Youth Risk Behavior Web-based Survey (KYRBWS) 2012, 2013, 2014, 2015, and 2016 were used for this study. The KYRBWS used a cross-sectional study design and comprised a nationwide web-based survey of Korean adolescent health behaviors. The KYRBWS was the result of collaboration between the Korea Centers for Disease Control and Prevention, Ministry of Health and Welfare, and Ministry of Education. The study design included multistage sampling, stratification, and clustering. The samples were stratified by 44 regional and school type variables and the participants were selected from two sources: school (first sampling unit) and class (second sampling unit). The validity and reliability of the data collected using the questionnaire survey analysis has been approved by several studies.2223 The study population consisted of 74,186 students in 2012, 72,435 students in 2013, 72,060 students in 2014, 68,043 students in 2015 and 65,528 students in 2016 from 400 middle schools and 400 high schools in Korea. Students who did not have a mother or father or both mother and father (n = 24,894) were excluded from our study population. After excluding missing data (n = 1), our total sample size comprised 327,357 individuals.
Variables
The dependent variable was adolescent depressive symptoms. All participants were asked the question, “Within the last year, did you experience any emotions such as sadness or despair continuously for 2 whole weeks, which was enough to hinder your daily life?” Respondents who answered “Yes” were classified as having depressive symptoms, and those who answered “No” were classified as having no depressive symptoms.
The main independent variable of interest in this study was the parents' country of birth. We examined the parents' country of birth using a questionnaire; the data were subjected to two stages of analyses. At the first stage, the students were asked to state whether the father and/or mother was born in Korea or abroad using a “Yes” or “No” response. Subsequently, the participants were divided into three groups: i.e., both parents were native Korean, only one parent was born abroad, both parents were born abroad. In the second stage of the analysis, the participants were asked, “In which country was your father/mother born?” Accordingly, the participants were classified into six groups on the basis of their fathers' or mothers' country of birth and considering the possibility that both parents were native Korean: Korea, China, North Korea, developing countries, Japan, Taiwan, and Others. Developing countries included Vietnam, Philippines, Mongolia, Thailand, Cambodia, and Malaysia, which ranked below 25 in GDP globally after excluding other country groups.
We controlled for sociodemographic, socioeconomic, health-behavior, and health-condition covariates in the analysis. The sociodemographic factors were grade (middle school student, high school) and gender (male, female). The socioeconomic factors were school achievement (low, middle, high), region (metropolitan, urban, rural area), father's/mother's educational level (high school or less, college or over, unknown), household income level (low, middle, high). Metropolitan areas included capital and metropolitan cities, urban areas included cities except metropolitan areas, and rural areas included the remaining geographic area, except for the metropolitan and urban regions. Health-behavior factors included physical activity (inactive, low, middle, high), smoking status (ever or never), and alcohol consumption (ever or no), Health-condition factors included suicidal thoughts (yes or no), sleep duration for overcoming fatigue (enough, normal, not enough), perceived health status (good, normal, bad), perceived happiness status (good, normal, bad), stress level (high or low) and year (2012, 2013, 2014, 2015, and 2016).
Statistical analysis
First of all, χ2 tests were used to confirm significant differences in the presence of adolescents' depressive symptoms according to the parents' migration background. We also conducted logistic regression analysis to determine adjusted odds ratios (ORs) and 95% confidence intervals (CIs). Subgroup analysis was performed according to grade, gender, region, household income level, father's educational level, and mother's educational level. Model fitting was conducted using the PROC SURVEYLOGISTIC procedure using SAS software, version 9.4 (SAS Institute, Cary, NC, USA). All analyses were performed by applying strata, cluster, and weight procedures. A P value < 0.05 was considered to indicate a statistically significant result.
RESULTS
Table 1 demonstrates the general characteristics of the study population. Of the 327,357 participants, 88,341 (27.0%) have depressive symptoms and 239,016 (73.0%) do not. The rate of depressive symptoms is higher among adolescents born in families wherein only one was born abroad (27.4%) than among adolescents with native Korean parents (27.0%). Furthermore, the rate of depressive symptoms is the highest among adolescents from families wherein both patents were born abroad (43.8%).
Table 1
General characteristics of the study population

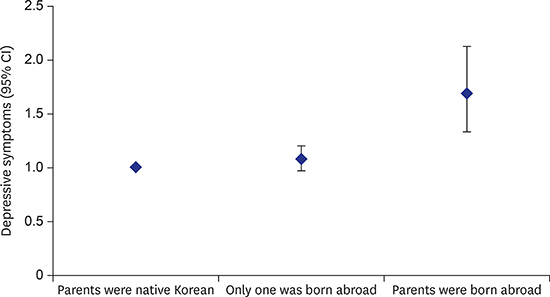
Table 2 shows the results for the factors associated with adolescent depressive symptoms. After controlling for covariates, the parents' country of birth is significantly associated with adolescent depressive symptoms. Respondents whose parents were born abroad are more likely to have depressive symptoms than respondents whose parents were native Korean and respondents with only one was born abroad (only one was born abroad: OR = 1.08; 95% CI, 0.97–1.20; parents were born abroad: OR = 1.68; 95% CI, 1.33–2.12).
Table 2
Factors associated with adolescents' depressive symptoms

Table 3 demonstrates the results of the subgroup analysis of the effect of parents' country of birth on the incidence of adolescent depressive symptoms, stratified by grade, gender, region, household income level, father's educational level and mother's educational level. The analysis stratified by grade revealed that, compared with middle school students, high school students with one or both non-native Korean parents have a greater magnitude of depressive symptoms (only one was born abroad: OR = 1.15; 95% CI, 0.97–1.36; parents were born abroad: OR = 2.04; 95% CI, 1.45–2.87). Overall, the multiculturism of the family is found to be directly proportional to the magnitude of depressive symptoms in the adolescents.
Table 3
Subgroup analysis of depressive symptoms with parents' country of birth by demographic factors
Table 4 shows a more detailed analysis of the correlation between the parents' country of birth and the adolescents' depressive symptoms. Respondents whose father was North Korean are more likely to have depressive symptoms (father born in North Korea and mother was native Korean: OR = 4.70; 95% CI, 1.27–17.44) compared to respondents from other groups. Also, adolescents whose father was from Japan or Taiwan are more likely to be have depressive symptoms than other groups (OR = 1.49; 95% CI, 1.15–2.77). Additionally, depressive symptoms are observed more frequently in adolescents with mother was from a developing country and father was native Korean (OR = 1.31; 95% CI, 1.02–1.70) than other adolescents.
Table 4
Adolescents' depressive symptoms associated with parents' country of birtha

OR = odds ratio, CI = confidence interval.
aAdjusted by grade, gender, region, household income level, school achievement, father's educational level, mother's educational level, physical activity, smoking status, alcohol consumption, suicidal thoughts, sleeping duration for overcoming fatigue, perceived health status, perceived happiness status, stress level, year.
Finally, in Supplementary Table 1, the general characteristics of the study population are demonstrated according to parental country of birth. We found that father's educational level and mother's educational level are higher among native Korean parents than among parents born abroad. Furthermore, the frequency of low household income level is 17.2% in the families with native Korean parents and 34.6% in families wherein the parents were born abroad group.
DISCUSSION
The aim of this study was to identify significant correlations between the parents' country of birth and adolescent depressive symptoms in Korea. The findings revealed that, compared with adolescents whose parents are both native Korean, adolescents whose parents were born abroad are more likely to have depressive symptoms. In high school students, the parents' country of birth has a greater influence on the existence of depressive symptoms than that in middle school students. By subdividing the parents' country of birth, we found that if father was born in North Korea or Japan or Taiwan and mother was native Korean, the adolescents are more likely to have depressive symptoms. When the mother's country of birth was developing countries, adolescents are more likely to have depressive symptoms.
In this study, adolescents whose parents were born abroad are more likely to have depressive symptoms than adolescents whose parents were both native Korean. This could be explained by several reasons. Adolescents of immigrants experience many conflicts and unfamiliar situations as they grow in a dual culture where the values and attitudes of their fathers and mothers are different.24252627 Moreover, because the adolescents experience different lifestyles at home and in society, they often experience identity crises and value conflicts. Bilingual usage within the family could lead to difficulty with language competence. Additionally, adolescents of immigrants were more likely to experience poor parenting and family functioning and discrimination such as school violence. These factors can affect the mental health of multicultural adolescents.24252627 In addition, we found that low parental education levels and low household income were more commonly observed among multicultural families. Several previous studies have reported that lower parental education levels are associated with a higher probability of impaired mental health in the child. Moreover, children belonging to families with low household income levels are more likely to be depressed.2829
The present study shows that high school students demonstrated a greater magnitude of depressive symptoms than did middle school students, when analyzed according to the parents' birth country. In Korea, where educational success is very important, in order to go to university, high school students have to take an entrance examination.30 High school students therefore experience enormous amounts of educational success; several reports of high school students committing suicide owing to poor entrance examination performance have been reported.30 Because high school students have vulnerable mental health owing to this educational success, they may be more influenced by their parents' birth of country.
In multicultural families, adolescents with father was from North Korea are more likely to have depressive symptoms. This may be associated with the traumatic events experienced while escaping from North Korea to South Korea. People who escaped from North Korea to South Korea were often crossing through China or other Asian countries.31 If arrested during this process, the people were deported to North Korea again and would face severe punishment or a death penalty. These traumatic events may cause serious mental health problems for North Korean defectors. Moreover, North Korean defectors commonly experience discrimination and political problems in South Korea.3132 Therefore, adolescents with one North Korean father may experience mental health problems owing to the unstable parenting and home environment.
Adolescents with their mother from a developing country tend to have depressive symptoms more frequently than other adolescents. It is necessary to consider that many immigrants from developing countries are migration workers.3233 Most migration workers are given dirty, dangerous, difficult, and low-paying jobs that South Koreans refuse. Therefore, migration workers are likely to maintain a low economic level. In addition, there were many international marriages between women from developing countries and men who were not married to native Korean women. These families tended to maintain a low economic level; in particular, the women who migrated had several difficulties adapting to the South Korean culture.3233 Furthermore, people from low-income countries experienced more severe discriminations than people from high-income countries.34 Thus, adolescents with their mother from developing countries were more likely to experience lower incomes and several discriminations. These factors may have contributed to the adolescents' depressive symptoms.
This study had some limitations. First, the data were self-reported by the participants. It is possible that the responses did not match the actual depressive symptoms rate. Second, we could not examine several parental factors such as their characters and domestic violence exposure. Parental characteristics are known as important factors that determine the adolescent's mental health.3536 Third, the study was based on a cross-sectional survey. Causality could not be confirmed clearly and the association could be confirmed. These limitations will be considered in a future study. Despite the above limitations, this study also had strengths. First, this study used the most recent nationally, multistage, stratified collected data. Therefore, the results obtained are representative of Korean adolescents. Second, although most previous studies were conducted in Caucasians who already have formed a multicultural society, we conducted research in Asian society, which is experiencing the early stages of a multicultural society. Third, to the best of our knowledge, this study offers new insights into the association between the parents' country of birth and adolescent depressive symptoms rates.
In conclusion, in our investigation of the correlation between the parents' country of birth and adolescent depressive symptoms, we found that, compared with adolescents whose parents were both native Korean, adolescents whose parents were born abroad are more likely to have depressive symptoms. Korea is in the early stages of forming a multicultural society; therefore, the number of studies on multicultural adolescents and mental health in Korea is limited. From a long-term point of view, mental health examinations for adolescents from multicultural families should be conducted, and adolescent mental health should be given attention. In addition, the existing multicultural policy does not include a classification according to the parent's country of origin; the immigrant populations with various nationalities are included in a single policy. The findings of our study confirm that the rates of depressive symptoms differ according to the parent's country of birth. Further studies should investigate the relationship between detailed characteristics of the parent's country of birth and their offspring's mental health. In addition, multicultural family support policies should be implemented, considering the characteristics of the parent's country of birth. Also, schools, government, and communities should propose and implement the multicultural education policies so that the growing youth could understand and accept the multicultural society. Overall, the findings also demonstrate what could happen in an early multicultural era. The results could be regarded as a prequel to the current situation in advanced multicultural societies such as the United States and Canada,373839 and could have implications in many countries experiencing the early stages of a multicultural society.40
 XML Download
XML Download