

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Youn Shin Kim1 , Ji Hye Park2
, Ji Hye Park2
, Ji Hye Park2
Abstract
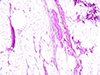
Progressive muscular dystrophy (PMD) is a primary muscle disease characterized by progressive muscle weakness and wasting, which is inherited by an X-linked recessive pattern and occurs mainly in males. There are several types of muscular dystrophies classified according to the distribution of predominant muscle weakness including Duchenne and Becker, Emery-Dreifuss, facioscapulohumeral, oculopharyngeal, and limb-girdle type. Clinical manifestations of PMD are clumsy, unsteady gait, pneumonia, heart failure, pulmonary edema, hydropericardium, hydrothorax, aspiration, syncopal attacks, and sudden cardiac death. The deceased was a 34-year-old man, and the onset of the first clinical symptom, gait disturbance, was in his late teens. His elder brother had the same disease and experienced brain death after a head trauma and died after mechanical ventilation was discontinued. After an autopsy, we found contracture of the joints, pseudohypertrophy of the calf, wasting and fat replacement of the thigh muscle, pericardial effusion (80 mL), fibrosis and fat replacement of the cardiac ventricular wall, pulmonary edema, and froth in the bronchus. The cause of death was heart failure and dyspnea due to muscular dystrophy. There was no sign or suspicion of foul play in his death.
Figures and Tables




References
1. Emery AE. The muscular dystrophies. BMJ. 1998; 317:991–995.
2. Kim KI, Oh BH, Rhee MY, et al. Deletion of exon in the dystrophin gene in a case of Becker muscular dystrophy with cardiac involvement. Korean Circ J. 1998; 28:805–811.

3. Globus JH. The pathologic findings in the heart muscle in progressive muscular dystrophy. Arch Neurol Psychiatr. 1923; 9:59–72.
4. Darras BT. Molecular genetics of Duchenne and Becker muscular dystrophy. J Pediatr. 1990; 117:1–15.
5. Emery AE. The muscular dystrophies. Lancet. 2002; 359:687–695.
6. Lee JH, Chae JH, Kim KJ, et al. Diagnosis of Duchenne/Becker muscular dystrophy: clinical and moleculargenetic characteristics. J Korean Child Neurol Soc. 2000; 8:211–220.
7. van Ommen GJ, Scheuerbrandt G. Neonatal screening for muscular dystrophy. Consensus recommendation of the 14th workshop sponsored by the European Neuromuscular Center (ENMC). Neuromuscul Disord. 1993; 3:231–239.
8. Steare SE, Dubowitz V, Benatar A. Subclinical cardiomyopathy in Becker muscular dystrophy. Br Heart J. 1992; 68:304–308.
9. Hapke EJ, Meek JC, Jacobs J. Pulmonary function in progressive muscular dystrophy. Chest. 1972; 61:41–47.
10. Eckardt L, Harzer W. Facial structure and functional findings in patients with progressive muscular dystrophy (Duchenne). Am J Orthod Dentofacial Orthop. 1996; 110:185–190.
 XML Download
XML Download