

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Hashimoto thyroiditis (HT), also known as chronic lymphocytic thyroiditis, is the most common human autoimmune disease, with an incidence estimated to range from 0.3 to 1.5 cases per 1,000 people [12]. HT is characterized by a cellular immune response involving T and B lymphocytic infiltration of the thyroid gland, as well as by a humoral immune response leading to the production of thyroid-specific antibodies [3].
Papillary thyroid cancer (PTC) is the most common histologic type of thyroid cancer, and its incidence is increasing rapidly worldwide [4]. Notably, epidemiological studies have reported an average coexistence rate between HT and PTC of approximately 23% (range, 5% to 85%) [5]. Although the mechanism underlying this association is not fully understood, several experimental studies have suggested that the synchronous appearance of HT and PTC reflects an immunological link. Consistent with these findings, a recent meta-analysis of 76,281 patients in 27 studies observed HT in patients with PTC more frequently than in those with benign thyroid diseases [6]. Apart from its positive association with the development of PTC, interestingly, HT has also been suggested to play a protective role against the progression of PTC [5789]. A meta-analysis [5] revealed that PTC patients with coexisting HT exhibited less aggressive clinicopathologic characteristics, as manifested by lower rates of extrathyroidal extension (ETE) and lymph node metastasis, and showed a longer recurrence-free survival duration. However, that meta-analysis only included four studies and did not present a subgroup analysis according to potential confounding factors, such as tumor size.
Given the limitations of previous work and the subsequent publications in this field, an updated review and meta-analysis of recent data is warranted to better understand and clarify the effects of HT on the progression of PTC. Therefore, we performed an updated meta-analysis via a comprehensive investigation of the literature and a predefined subgroup analysis.
METHODS
Search strategy
The literature search was performed in accordance with the general principles recommended in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (Supplemental Table S1). Two independent investigators (S.M. and H.S.C.) searched the PubMed and Embase databases and selected articles using combinations of the following terms: “Hashimoto's thyroiditis” or “chronic lymphocytic thyroiditis” and “thyroid cancer.” Only articles published in English prior to September 2017 were included.
Study selection
The literature search yielded 1,132 potentially relevant articles, of which 982 were screened for further review after excluding duplicate studies. If a single study was described in multiple reports, the latest or most complete publication was included. All articles were downloaded and screened for inclusion using a 2-step method. After an evaluation of the titles and abstracts according to predefined criteria, 898 articles were excluded because they met one or more of the following criteria: (1) a different topic of interest; (2) an animal or in vitro study; (3) no information about HT or thyroid cancer; or (4) publication as an abstract, expert opinion, conference article, or review. Subsequently, the full texts of the 85 remaining articles were reviewed by two independent investigators (S.M. and H.S.C.), and any disagreement was resolved by a third investigator (Y.J.P.). Seventy-two articles were finally selected for the meta-analysis (Fig. 1).
Assessment of bias risk
Three researchers independently assessed the methodological quality of the included articles using the Newcastle-Ottawa Scale for case-control studies [10]. Eight items were included in the quality assessment, and all articles received scores above 5 of 9. We concluded that the quality of these cross-sectional studies would not affect the quality of our meta-analysis.
Data extraction
The following variables were independently extracted by the two investigators using the same criteria: first author, publication year, country, number of study participants, number of cases of coexistence of HT, sex ratio, and the clinicopathologic features and recurrence of PTC.
Data analyses and statistical methods
We used the Mantel-Haenszel method to calculate the pooled odds ratios (ORs) or relative risks (RRs) with 95% confidence intervals (CIs). The Higgins I2 statistic was used to test for heterogeneity. Here, an I2 ≤50% indicated that the included studies had little heterogeneity, and a fixed-effects model was used; by contrast, an I2 >50% indicated heterogeneity, and a random-effects model was used. Subgroup and sensitivity analyses were used to determine the cause of heterogeneity. The Egger test and a funnel plot analysis were used to determine the likelihood of publication bias. All statistical analyses were performed using the statistical program R (R version 3.1.0, 2014, R Project for Statistical Computing, Vienna, Austria; www.r-project.org).
RESULTS
Characteristics of selected studies
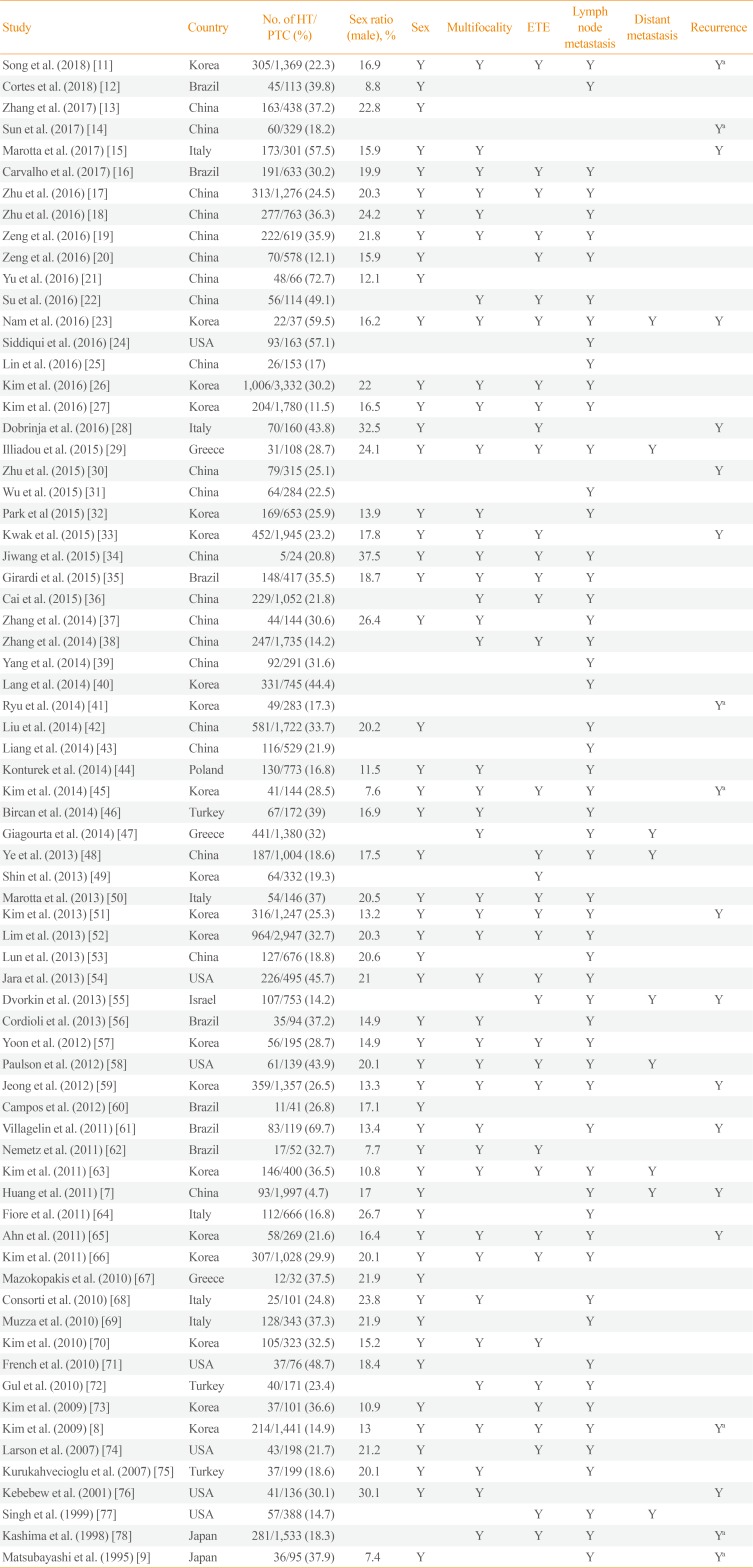
The main characteristics of the 71 articles included in this meta-analysis are summarized in Table 1 [7891112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960616263646566676869707172737475767778]. A total of 44,034 participants with PTC were enrolled, of whom 11,132 (25.3%) had HT. The sample sizes of these studies ranged from 24 to 3,332 participants. Among them, 53 studies reported the mean tumor size of PTC and eight studies provided longitudinal data for recurrence-free survival. Forty-three studies were conducted in Asia, 14 studies in America, and 14 studies in Europe.
Effect of HT on the clinicopathologic characteristics of PTC
To investigate the association between HT and sex, 55 studies were analyzed. HT was detected in 802 of 6,489 male (12.4%) and 8,438 of 28,717 female (29.4%) with PTC, and a significant association was identified between female sex and HT (OR, 3.13; 95% CI, 2.67 to 3.68). However, as significant heterogeneity was observed among the studies (I2=65.1%), we conducted analyses of sensitivity and publication bias. The sensitivity analysis identified two outlier studies [1844]. After omitting these studies, the estimated pooled OR was 3.49 (95% CI, 3.21 to 3.79) without significant heterogeneity (I2=49.8%) (Table 2). The funnel plot analysis and the Egger test revealed no significant publication bias (P=0.366).
Thirty-eight studies provided data suitable for a meta-analysis of the association between HT and ETE in patients with PTC. In this population, ETE was reported in 2,856 of 7,311 patients (39.1%) with HT and in 9,796 of 22,527 patients (43.5%) without HT. Accordingly, the coexistence of HT was found to show a negative association with the presence of ETE (OR, 0.75; 95% CI, 0.70 to 0.79) (Table 2). No significant heterogeneity was observed among these studies (I2=30.8%).
For the association between HT and tumor multifocality, 42 studies were included. Among the PTC patients, 2,536 of 8,129 (31.2%) with HT had multifocal disease, as did 6,345 of 22,970 (27.6%) without HT. Coexistent HT and PTC was thus found to be associated with tumor multifocality (OR, 1.17; 95% CI, 1.05 to 1.31) (Table 2). However, as significant heterogeneity was detected among the studies (I2=65%), we conducted analyses of sensitivity and publication bias. After omitting the single outlier study identified in the sensitivity analysis [18], the estimated pooled OR was 1.13 (95% CI, 1.03 to 1.24) without significant heterogeneity (I2=48.6%). The funnel plot analysis and the Egger test revealed no significant publication bias (P=0.741).
To determine the effects on lymph node metastasis, 57 studies were included. Among patients with PTC, 3,829 of 9,767 (39.2%) with HT had lymph node metastasis, as did 12,542 of 29,378 patients (42.7%) without HT. Accordingly, coexistent HT and PTC was found to be negatively associated with lymph node metastasis (OR, 0.82; 95% CI, 0.72 to 0.94) (Table 2). However, as significant heterogeneity was identified among the studies (I2=81%), we analyzed sensitivity and publication bias. In the sensitivity analysis, the pooled ORs ranged from 0.79 to 0.85 after omitting each study individually, and remained statistically significant. The funnel plot analysis and the Egger test revealed no significant publication bias (P=0.647).
Eight studies that included 957 patients with HT and 4,221 patients without HT were analyzed with regard to distant metastasis. Distant metastasis was reported in 25 patients (2.6%) with HT and 185 patients (4.4%) without HT. Accordingly, the coexistence of HT with PTC was found to be negatively correlated with distant metastasis (OR, 0.49; 95% CI, 0.32 to 0.76) (Table 2). No significant heterogeneity was found among these studies (I2=0%).
Effect of HT on recurrence of PTCs
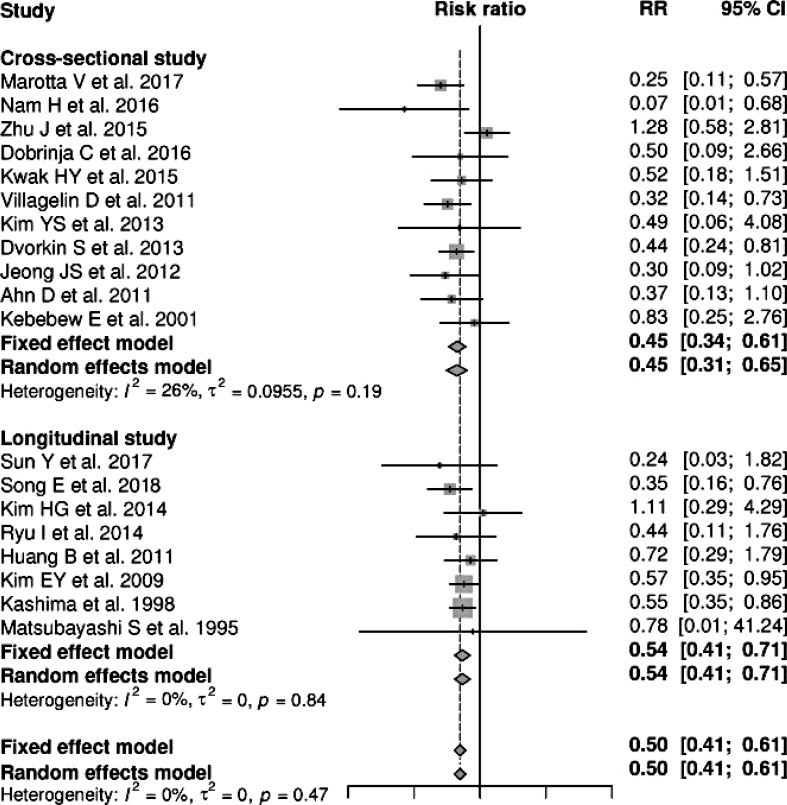
Nineteen studies, including 11 cross-sectional studies and eight longitudinal studies, provided data suitable for a meta-analysis of the association between HT and PTC recurrence. Here, coexistent HT and PTC were found to be negatively associated with the recurrence of PTC (RR, 0.50; 95% CI, 0.41 to 0.61) (Fig. 2). No significant heterogeneity was found among these studies (I2=0%), and a subgroup analysis by study design yielded similar results (Fig. 2).
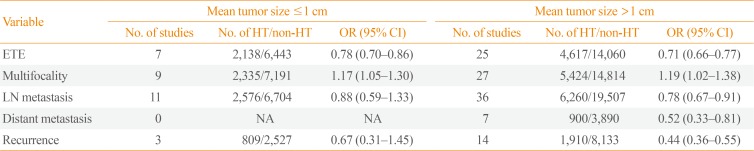
Subgroup analysis by tumor size and study location
We next performed a subgroup analysis according to the mean tumor size (Table 3). Here, the significant negative associations of HT with ETE were independent of the mean tumor size. Among cases with a mean tumor size >1.0 cm, coexistent HT was negatively associated with lymph node and distant metastases and recurrence of PTC.
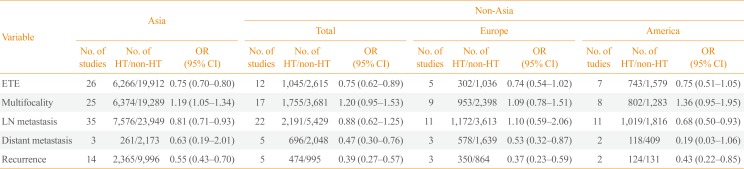
A subgroup analysis based on the study location revealed that the significant associations of HT with absence of ETE and recurrence were location-independent. Among Asian patients, coexistent HT was negatively correlated with lymph node metastasis of PTC, whereas in studies conducted elsewhere, coexistent HT was negatively correlated with distant metastasis (Table 4).
DISCUSSION
An association between HT and PTC was initially proposed in 1955 by Dailey et al. [79], who linked chronic inflammation to neoplastic changes. Since then, many studies have aimed to evaluate the association between these two prevalent diseases [380]. In this updated meta-analysis of 71 observational studies, we demonstrated that coexistent HT was significantly associated with better clinicopathologic characteristics and an improved prognosis among patients with PTC, as demonstrated by reduced incidence of ETE, lymph node metastasis, and distant metastasis and an increased recurrence-free survival duration relative to those in patients without HT. In contrast to clinicopathologic characteristics, multifocality was positively correlated with HT. Because multifocality has been considered to be a feature associated with the development of PTC, rather than with its aggravation, these findings are consistent with previous studies that reported a positive association of HT with PTC development, along with a protective role of HT against the progression of PTC [356]. Although significant heterogeneity was detected, the results did not change after adjustments via subgroup, sensitivity, and publication bias analyses.
Although the mechanism by which HT affects PTC remains unclear, several hypotheses have been suggested. Among them, inflammation-induced carcinoma has been proposed as one of possible mechanism [81]. The activated inflammatory response in HT, which involves the production of mediators by immune cells in a state of chronic inflammation, might create a favorable setting for malignant transformation in the thyroid gland [381]. However, this hypothesis has difficulties explaining the protective role of HT against the progression of PTC. In this context, tumor defense-induced autoimmunity, such as thyroid-specific cytotoxic T-cells, might play a role [3]. Thyroglobulin (Tg) and thyroid peroxidase (TPO), which are presented on antigen-presenting cells and thyrocytes, are the main target antigens of cellular immune reactions in HT, and these immune reactions may result in target-specific destruction of the thyroid gland [3]. Since TPO and Tg also seem to be specific target antigens in PTC, anti-thyroid antibodies may destroy PTC in the same way as they destroy normal thyroid follicular cells [382]. Several studies have reported increases in antitumor T-cell-mediated immune reactions [798384], while others have suggested the involvement of apoptotic pathway activation [85]. However, whether thyroid-specific cytotoxic T-cells also recognize TPO and Tg in PTC needs investigation.
A genetic predisposition was proposed as another possible mechanism of the protective properties of HT against the progression of PTC, because the BRAF V600E mutation, a marker of more aggressive behavior in PTC, was less frequently detected in patients with coexistent HT than in those without HT [86].
This study had considerable strengths, such as the inclusion of many observational studies with large populations and the performance of predefined subgroup analyses. Our study is therefore the first to demonstrate an association of HT with better outcomes of PTC, regardless of tumor size. Furthermore, we conducted a subgroup analysis according to the region where each study was performed to account for differences in iodine status, and observed that although most studies were performed in Asia and indicated better outcomes of PTC among patients with coexistent HT, studies from non-Asian countries yielded similar results.
Despite the above strengths, however, the present study also had some potential limitations. First, the included studies mainly featured retrospective designs. Further prospective studies are needed to clarify the potential causal relationship between HT and PTC. Second, inter-study differences in age, sex ratio, and iodine status might have led to bias. Third, the included studies predominantly involved Asian populations. Although we performed a subgroup analysis based on study location, further large cohort studies involving multiple races are needed.
In conclusion, this meta-analysis clearly demonstrated that among patients with PTC, coexistent HT is associated with better clinicopathologic features and clinical outcomes. Although the underlying mechanism remains unclear, our findings suggest that this association could be used to predict the prognosis of PTC in clinical settings. Further prospective and large cohort studies are warranted to elucidate the link between HT and PTC.


 XML Download
XML Download