

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Chest CT has become a common imaging modality for various clinical conditions of the lung, chest wall, mediastinum, pleura, and diaphragm (1). Although not routinely used to assess breast lesions, the entirety of the breast usually appears on chest CT. With the increasing use of chest CT, incidental breast lesions are being frequently encountered (2345). Thus, it is important for clinicians to be familiar with the CT characteristics of breast lesions, which can be referred to mammography or breast ultrasonography (US) for further evaluation if necessary (6).
Several previous studies have reported that the detection rate of incidental breast lesions on chest CT ranges from 0.06% to 7.63% (789). The referral rates of incidental breast lesions on chest CT are uncertain and malignancy rates of the referred cases vary with a wide range (9.2% to 70%) (9101112). This suggests that effective criteria for referral to diagnostic breast evaluation are needed for incidental breast lesions found on chest CT, which may provide further characterization of the incidental breast lesions due to its high resolution, large field of view (FOV), and cross-sectional capabilities (13).
There are a few reports that have investigated suspicious CT characteristics of incidental breast malignancy (3121415). Reliable features for breast malignancy on CT include spiculation, irregular shape, and rim enhancement (16). However, these CT features are not robust and some remain controversial (101117). The aims of this study were to evaluate the CT features of incidentally found breast lesions on chest CT, and to suggest useful criteria for referral to a specialized breast unit for assessment.
MATERIALS AND METHODS
Patients
This retrospective study was performed with approval of the Institutional Review Board (3-2017-0114). Given the retrospective nature of the study and the use of anonymized data, requirements for informed consent were waived. All reports of chest CT examinations from May 2009 to April 2014 containing the key word ‘breast’ were reviewed. Patients with known breast disease, previous history of breast cancer or breast surgery, or who had undergone only non-enhanced CT examination were excluded from the study. Inclusion criteria were patients who exhibited incidental breast lesion(s) on enhanced chest CT and were referred to a specialist breast unit for assessment and then underwent pathological confirmation or follow-up over a 1-year period. A total of 55001 chest CT examinations were performed during the study period, and 1729 radiological reports containing the key word ‘breast’ were found. A total of 488 patients with no history of breast disease or breast operation were reported to have an incidental breast lesion on chest CT. Of these 488 patients, 224 (45.9%) were referred to a specialized breast unit; of these 224, 86 underwent pathological confirmation or follow-up for at least 1 year (Fig. 1).
Chest CT Scan Protocol
CT scans were obtained using one of three multi-detector CT scanners: a 16-slice (Somatom Sensation 16; Siemens Medical Solutions, Erlangen, Germany); a 64-slice (Somatom Sensation 64; Siemens Medical Solutions), or a 128-slice (Somatom Definition AS+; Siemens Medical Solutions) device. The chest CT scans were obtained from the lung apices to the level of the adrenal glands, during a breath hold at the end of inspiration, in the supine position. After acquiring a scout image to determine the FOV, CT scans were obtained after contrast material injection. Scanning was done by using a helical technique, with a 3 mm or 5 mm reconstruction interval. The exposure parameters for the CT scans were 120 kVp and 50–130 mA. Image reconstruction for conventional CT scans was obtained by using the scanner's workstation. All CT scans were transferred to a picture archiving and communication system (Centricity 2.0; GE Medical Systems, Mount Prospect, IL, USA).
CT Image Analysis
Two radiologists (C.H.P and T.H.K), each with > 10 years of experience with chest CT interpretation, reviewed the chest CT scans and were blinded to the final results of the breast assessment. Decisions regarding CT features were determined by consensus. The radiologists evaluated lesion morphology and contrast-enhancement patterns. In the absence of a formal CT lexicon for breast lesions, the modified Breast Imaging and Reporting Data System (Bi-RADS) terminology for MRI lexicon 2013 was used for the analysis of morphology (18).
The following CT findings were recorded for each lesion: size, location; shape (round or oval, irregular), margin (well-circumscribed, non-circumscribed), and enhancement ratio (poor enhancement, high contrast enhancement).
To overcome the various contrast media injection protocols, the attenuation ratio between breast masses and the ipsilateral trapezius muscles were calculated and used as the indicator of enhancement strength. Regions of interest were drawn in the breast lesion (as large as possible) and the ipsilateral trapezius muscle (larger than 1.5 cm2) and the attenuation (Hounsfield units) was measured. The enhancement ratio of the breast mass was calculated as (attenuation of breast lesion)/(attenuation of trapezius muscle). All lesions were categorized into 1 of 2 groups according to the attenuation ratio as follows: poor enhancement (attenuation ratio ≤ 1), or high contrast enhancement (attenuation ratio > 1).
Final Diagnosis
Eighty-six patients subsequently underwent breast US or mammography for the incidental breast lesion(s). Findings were reported according to the Bi-RADS US or mammography lexicon (1920). All mammography and breast US were analyzed by two experienced radiologists (H.M.G and E.J.S). Sonographically guided core-needle biopsy or surgery was done for definite diagnosis in 38 (44.2%) patients. The diagnoses in the remaining 48 (55.8%) patients were determined on the basis of follow-up chest CT or breast US for a period of at least 12 months.
Statistical Analysis
Continuous variables were stated as mean ± standard deviation, and categorical variables were expressed as frequencies and/or percentages. The Shapiro-Wilk test was performed to evaluate the distribution of continuous data. The independent t-test was used to compare the age and size of benign and malignant lesions. The Fisher's exact test was used to assess potential correlations of various CT features with breast lesion malignancy. The sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and overall diagnostic accuracy were calculated for the various criteria using significant CT characteristics to diagnose breast lesions on chest CT scans. A p value of < 0.05 was considered to be statistically significant. All statistical analyses were done using commercially available software (SPSS version 20, IBM Corp., Armonk, NY, USA).
RESULTS
Assessment Findings
Of a total of 86 breast lesions found on chest CT, the final assessment categories from mammography and breast US were distributed according to BI-RADS as follows: category 1 in 4 lesions (4.6%), category 2 in 12 lesions (14.0%), category 3 in 42 lesions (48.8%), category 4 in 23 lesions (26.7%), and category 5 in 5 lesions (5.8%). All 28 lesions that were BI-RADS category 4 and 5 underwent sonographically guided biopsy, which revealed 13 cancers and 15 benign lesions. One category 0 lesion was designated a category 3 lesion on follow-up breast US. Of the 4 breast lesions detected on chest CT that were BI-RADS category 1, breast mammography and US, one cancer was diagnosed. This lesion appeared as an 0.8 cm enhancing lesion in chest CT, and was not detected at mammography or US. Two-year follow-up breast US revealed a 1.0 cm irregular hypoechoic lesion in the right breast, and the final assessment was BI-RADS category 4. Subsequent tissue sampling and surgery were performed, and diagnosis of a 0.9 cm infiltrative ductal carcinoma was made (Fig. 2). The other three lesions were not detected on follow-up mammography or breast US, which suggested false-positive lesions on chest CT.
Overall, the malignancy rate of the incidental breast mass at chest CT was 16.3% (14 of 86), 78.6% (11 of 14) was invasive carcinoma [median tumor size, 1.5 cm (range, 0.5–1.9 cm)] and 21.4% (3 of 14) were ductal carcinoma in situ (Table 1).
There were 24 biopsy-proven benign lesions among the 86 patients. These included six fibrocystic diseases, 11 fibroadenomas, two atypical lobular hyperplasia, two sclerosing adenosis, one intraductal papilloma, one fibrosis and one abscess. The other 48 lesions were followed-up with CT or US and confirmed to be benign.
Clinical and CT Features of Breast Masses
The clinical and CT features were compared between malignant and benign lesions (Table 2). The mean age of patients with malignant breast tumors (56.7 ± 14.6 years) was higher than that of patients with benign breast lesions (47.4 ± 11.7 years) (p = 0.011). The mean size of the incidental malignant breast tumor was 1.2 ± 4.6 cm (range, 0.7–2.2 cm), whereas the mean size of incidental benign breast lesions was 1.1 ± 6.8 cm (range, 0.4–4.5 cm). There was no difference between the mean size of malignant and benign lesions (p = 0.793).
Among CT features, the shape, margin, and attenuation ratio were significantly different between malignant and benign lesions. Of the 14 patients with malignant breast masses, irregular shape was defined in 9 (64.3%) patients, and the other 5 (35.7%) patients exhibited oval or round masses. Of 72 patients with benign breast tumors, 5 (6.9%) exhibited an irregular shape and 67 (93.1%) exhibited oval or round masses. Incidental malignant breast masses exhibited a higher rate of irregular shape (p < 0.001).
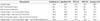
All malignant breast masses exhibited a non-circumscribed margin. Well-circumscribed margins were identified in 68 of 72 (94.4%) patients with benign breast masses and only 4 (6.9%) exhibited non-circumscribed margins. Notably, the incidence of non-circumscribed margin was higher in malignant masses than in benign masses (100% vs. 6.9%; p < 0.001). All malignant breast masses exhibited high contrast enhancement. Among benign breast masses, the incidence of high contrast enhancement was similar to that of poor enhancement (58.3% vs. 41.7%). Table 3 summarizes the sensitivity, specificity, PPV, NPV, and accuracy for malignancy in relation to the shape, margin, enhancement ratio, and combinations thereof. A feature of malignancy with high PPV was a non-circumscribed margin (94.4%). The combination of non-circumscribed margin and high contrast enhancement had the highest accuracy (97.7%), followed by non-circumscribed margin, with an accuracy of only 95.4% (Fig. 3).
DISCUSSION
In our study, we evaluated the CT features of incidental breast lesions on chest CT, and assessed useful CT features for referral to a specialized breast unit. Among the CT features, shape, margin, and attenuation ratio were significantly different between malignant and benign lesions. The combination of non-circumscribed margin and high contrast enhancement had the highest accuracy for malignancy.
In previous studies, most incidental breast lesions have been reported to be benign (221). Therefore, it is important for radiologists to be able to discern the differences in typical CT features of malignant and benign breast lesions to avoid unnecessary additional imaging workup. A few studies have evaluated the correlation between CT features and pathological outcomes of incidental breast lesions (910111217). The predictive CT features suggestive of malignant breast tumors on chest CT included larger size, irregular margins, spiculation, and rim enhancement (111216). In our study, malignant breast lesions exhibited significantly higher probabilities of irregular shape and non-circumscribed margins. Similarly, well-circumscribed lesions were suggestive of benignity. Careful assessment of the margins and shapes of incidental breast lesions may differentiate benign and malignant lesions.
Uematsu et al. (22) reported that attenuation of breast lesions is not useful in the differential diagnosis, and the presence of enhancement alone does not always suggest a malignant tumor. Another study reported that additional delayed enhancement on CT may be important to differentiate benign from malignant lesions (23). However, chest CT was usually obtained for indications other than breast pathologies, and protocols are not optimized for breast imaging; therefore, variation in contrast medium administration and scan time is expected. In this study, we used the attenuation ratio between the breast lesions and ipsilateral trapezius muscles to correct the diversity of enhancement protocols. High contrast-enhanced masses exhibited high sensitivity (100%), although a low PPV (25.0%) and accuracy (51.2%). Our findings suggest that enhancement ratio alone cannot be used as a reliable CT feature of malignancy or benignity. However, a combination of non-circumscribed margin and high contrast enhancement had high sensitivity, specificity, PPV, NPV and accuracy for incidental malignant breast masses (100%, 97.2%, 88.2%, 100%, and 97.7%, respectively).
In the present study, four incidental breast lesions were considered BI-RADS category 1 on initial mammography and breast US. One of these lesions increased in size on follow-up chest CT and was confirmed to be a malignant tumor; the other three lesions were not delineated on follow-up mammography and breast US. Mammography and breast US are currently preferred imaging modalities for breast abnormalities. Compared with mammography and US, CT has several advantages. A breast lesion may be better visualized using contrast-enhanced CT than mammography if the breast lesion is in a dense breast or if the lesion is located adjacent to the chest wall (24). However, normal breast glandular tissue could be appeared as a ‘pseudo-mass’ on CT, and this finding was more common in dense breasts (10). Therefore, chest CT cannot be a standard modality for breast evaluation, and it is important to refer to a specialized breast unit when incidental breast lesion(s) are detected.
There were a few limitations to this study, including its single-center, retrospective design. Second was the potential perception bias of missed or unreported breast lesions. Finally, despite a large number of chest CT examinations were carefully reviewed with strict inclusion/exclusion criteria, histological evaluation was absent in one-half of the incidental breast masses. Thus the malignancy rate of incidental breast lesions would have increased in this study.
In conclusion, the malignancy rate of incidentally found breast lesions on chest CT is not negligible. Reliable features for incidental malignant breast masses on chest CT were irregular shape, non-circumscribed margin, and high contrast enhancement. The combination of non-circumscribed margin and high contrast enhancement could help to distinguish incidental malignant breast lesions on routine chest CT and inform referral to a specialized breast unit.





 XML Download
XML Download