

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Clinical benefits of lipid-lowering with statins are well established. Randomized clinical trials have shown that intensive lipid-lowering results in the reduction of cardiovascular (CV) events in patients with stable coronary artery disease (CAD).1)2) Despite this high-quality evidence of superior effectiveness, high-dose statin therapy is reluctantly prescribed,3) which may be explained by concern about high-dose statins causing higher rates of side-effects, such as myalgia, transaminitis, and developing diabetes mellitus.1)2)4) Non-statin treatments in addition to a moderate dose of statin can be another option in such patients.5)
However, all non-statin treatments are focused on additional lipid-lowering effects beyond statin. Interestingly, a recent data suggested that anti-inflammatory treatment can also reduce the recurrent CV events on top of statin treatment.6) Although it is used as an anti-diabetic agent, pioglitazone, a peroxisome proliferator-activated receptor (PPAR)-γ agonist, is also a promising inflammation modulator, which may reduce the rate of CV death, myocardial infarctions, and strokes among patients with diabetes7)8) and with insulin resistance.9) Pioglitazone successfully retards an increase in the carotid intima-media thickness in patients with diabetes10)11) and attenuates plaque inflammation in insulin-resistant patients.12) Even in non-diabetic patients, pioglitazone shows an additive anti-inflammatory effect to statins.13)14) However, data are limited regarding whether pioglitazone further reduces plaque inflammation when combined with moderate dose statins in stable CAD patients with or without diabetes.
18F-fluorodeoxyglucose positron emission tomography/computed tomography (18F-FDG-PET/CT) imaging permits the noninvasive measurement of arterial plaque inflammation and successfully monitors alterations following therapy.15)16) Accordingly, we employed serial fluorodeoxyglucose positron emission tomography/computed tomography (FDG-PET/CT) imaging to address whether pioglitazone further reduced plaque inflammation in patients with stable CAD taking moderate dose statin.
METHODS
Design and subjects
This study was a prospective, open-labeled, randomized controlled single-center trial that evaluated the anti-inflammatory effects of atorvastatin treatment on an arterial plaque in the presence or absence of pioglitazone. Statin-naïve patients with angiographically significant stable CAD were imaged with serial FDG-PET/CT to assess the plaque inflammation in the carotid arteries and thoracic aorta. The study protocol was approved by the Institutional Review Board of Seoul St. Mary's Hospital (approval number: KC09MISV0195). This trial is registered with ClinicalTrials.gov, number NCT01341730. All subjects provided written informed consent.
Patients who underwent percutaneous coronary intervention due to stable CAD and had non-calcified atherosclerotic plaques of ≥3 mm in their carotid arteries identified via ultrasound examinations were eligible for this study. We excluded patients with any one of the following conditions: patients with acute coronary syndrome, statin or thiazolidinedione therapy within 4 weeks prior to the study, elevated liver function enzyme levels, significant renal dysfunction, congestive heart failure, less than 18 years of age, or pregnancy. After enrollment, all patients immediately underwent a baseline FDG-PET/CT, were randomized to treatment groups and underwent a second FDG-PET/CT after 3 months.
Study treatment
Eligible patients were randomized 1:1 to the atorvastatin (20 mg/day), or atorvastatin (20 mg/day) plus pioglitazone (30 mg/day) groups for 3 months using a computer-generated code after the baseline FDG-PET/CT scanning. Because atorvastatin and pioglitazone exert their greatest effects after 1 month,17)18) we administered atorvastatin and pioglitazone for 3 months. All medications, including anti-diabetic medications, anti-platelet agents, and anti-hypertensive medications, which were taken by the patients prior to the baseline FDG-PET/CT scanning, were continued.
18F-FDG-PET/CT analyses
FDG-PET/CT images were visually evaluated for the presence of an abnormal fluorodeoxyglucose (FDG) uptake in the bilateral carotid arteries and ascending aorta. Next, the FDG uptake in the arterial plaques was quantified by measuring the maximum standardized uptake values (SUVs) corrected for the body weight. The SUV was calculated using the pixel activity value within the region of interest (ROI) placed on the entire vasculature obtained from consecutive co-registered transaxial FDG-PET and contrast-enhanced computed tomography (CT) images. The SUV was the highest value of the pixel activity within the ROI of every vessel. The SUVs were measured along the carotid arteries and ascending aorta at 5 mm intervals in an axial orientation. The arterial SUV scores were derived by averaging the SUVs for all slices within the arterial territories. The arterial target-to-background ratio (TBR) was then calculated by dividing the arterial SUV score by the blood SUV (background) to produce a blood-corrected artery SUV. Two nuclear medicine physicians blinded to the treatment groups made the FDG uptake measurements, and the 2 measurements were averaged.
Study outcomes
The primary endpoints were comparing the absolute changes in the TBR within an index vessel between atorvastatin and atorvastatin plus pioglitazone during the 3 months of treatment. An index vessel was defined as a carotid artery with plaque buildup detected before the treatment using carotid ultrasound. In cases where both carotid arteries had detectable plaque buildup, we chose the artery with the higher TBR as the index vessel. The secondary endpoint was the change in the TBR within each carotid artery and the ascending aorta.
Statistical analyses
Based on a previous study, we assumed that 20% of the patients would not be able to be evaluated for the primary outcome, and estimated that 20 patients in each treatment group would provide an 80% power to detect an absolute decrease of 0.1 or greater in the TBR within the index vessel upon the addition of pioglitazone (30 mg), with a standard deviation (SD) of 0.1 and α=0.05 on the basis of a previous study.12)
Continuous variables are expressed as the mean±SD or medians (interquartile range), whereas categorical variables were expressed as frequencies. Continuous variables were compared using the paired t-test or Wilcoxon rank-sum test for changes in each group, and an unpaired t-test or the Mann-Whitney U test for differences between groups. Statistical significance was defined as a 2-sided p value <0.05.
RESULTS
Characteristics of the study population
Baseline and follow-up FDG-PET/CT images were available in 33 patients. Sixteen patients received atorvastatin, and 17 received atorvastatin plus pioglitazone. The patient population details are described in Figure 1. The demographic characteristics at baseline are shown in Table 1. There were no significant differences in the baseline data between the 2 groups.
 | Figure 1Study flow chart of the patient enrollment.
CAD = coronary artery disease; 18F-FDG-PET/CT = 18F-fluorodeoxyglucose positron emission tomography/computed tomography.
|
Table 1
Baseline characteristics of the patients
Values are the mean±standard deviation or number (%).
BMI = body mass index; CAD = coronary artery disease; NS = not significant.
![]()
Treatment effects on the metabolic, lipid, and inflammatory parameters
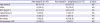
Both treatments were well tolerated, and there were no adverse events. After the 3 months of treatment, the atorvastatin plus pioglitazone group showed lower fasting serum insulin levels and homeostatic model assessment insulin resistance (HOMA-IR) indices compared with the atorvastatin group (Table 2). Although both groups showed similar and significant reductions in the serum total cholesterol, triglyceride, and low-density lipoprotein (LDL) cholesterol levels, only the atorvastatin plus pioglitazone group revealed a significant increase in the serum high-density lipoprotein (HDL) cholesterol. The serum LDL cholesterol levels dropped below 70 mg/dL in two-thirds of the patients (12 of 16 patients in the atorvastatin group, and 13 of 17 patients in the atorvastatin plus pioglitazone group). The high-sensitivity C-reactive protein (hsCRP) serum levels were significantly reduced in both groups. However, the changes did not significantly differ between the groups (p=0.83). Both groups also showed similar reductions in the serum matrix metalloproteinase-9 (MMP-9) levels.
Table 2
Laboratory findings during a 3-month treatment

Values are the mean±standard deviation or median (interquartile range).
HDL = high-density lipoprotein; HOMA = homeostatic model assessment; hsCRP = high-sensitivity C-reactive protein; LDL = low-density lipoprotein; MCP-1 = monocyte chemoattractant protein-1; MMP-9 = matrix metalloproteinase-9; NS= not significant; PAI-1= plasminogen activator inhibitor-1.
![]()
Treatment effect on the arterial FDG uptake
Representative images of improved FDG uptake in the carotid plaque after combination treatment (atorvastatin plus pioglitazone are shown in Figure 2 and the FDG-PET/CT data are presented in Table 3. The baseline TBRs of both carotids and the ascending aorta were similar between the 2 treatment groups (right carotid artery; p=0.98, left carotid artery; p=0.60, and ascending aorta; p=0.06). After the 3 months of treatment, the TBR values in the bilateral carotid arteries and ascending aorta were significantly reduced in both groups.
 | Figure 2Representative images of carotid plaque of a patient treated with atorvastatin and pioglitazone. Representative FDG-PET (top), CT (second from top), FDG-PET/CT (third from top) images at baseline (left) and at 3-month follow-up (right) are shown. Average of cross-sectional analysis (bottom) of FDG uptakes of the index vessel (arrow) was the primary endpoint.
CT = computed tomography; FDG = fluorodeoxyglucose; FDG-PET = fluorodeoxyglucose positron emission tomography.
|
Table 3
FDG-PET/CT findings during a 3-month treatment

Values are the mean±standard deviation.
FDG-PET/CT = fluorodeoxyglucose positron emission tomography/computed tomography; Lt. = left; Rt. = right; TBR = target-to-background ratio.
![]()
Regarding the primary endpoint of the TBR within the index vessel, the baseline TBR values were similar between the groups (p=0.78). The reduction in the TBR within the index vessel was greater in the patients with atorvastatin plus pioglitazone than in those with atorvastatin and the difference between the 2 groups exhibited a marginal difference (atorvastatin plus pioglitazone; −0.10±0.07 and atorvastatin −0.06±0.04, p=0.058, Figure 3A).
 | Figure 3Absolute change in the FDG uptake in the index vessel during a 3-month treatment. (A) The TBR was evaluated in individual patients at baseline and after 3-month treatment with atorvastatin 20 mg (left) and atorvastatin 20 mg plus pioglitazone 30 mg (mid). The absolute change in TBR from baseline (right). (B) Individual changes and the absolute change of the TBR in patients with baseline TBR above the median.
FDG = fluorodeoxyglucose; TBR = target-to-background ratio.
|
We underwent an exploratory analysis dividing the patients according to the baseline TBR of the index vessel. The difference between the 2 groups was more evident in patients with a baseline TBR above the median (n=8, each in both groups). The patients with a baseline TBR above the median (median TBR=1.65) were likely to be more male and hypertensive and did not differ in the frequency of diabetes and HOMA-IR compared to those with a baseline TBR below the median (Supplementary Table 1). The addition of pioglitazone to atorvastatin showed a greater reduction in the TBR from baseline than atorvastatin only in patients with a baseline TBR above the median (atorvastatin plus pioglitazone; −0.14±0.04 and atorvastatin −0.03±0.03, p<0.001, Figure 3B), though the baseline TBRs were similar (atorvastatin plus pioglitazone; 1.83±0.13, atorvastatin; 1.75±0.07, p=0.18). In contrast, the difference in the reduction of the TBR was insignificant in the patients with a baseline TBR below the median (atorvastatin plus pioglitazone; −0.06±0.05 and atorvastatin −0.08±0.04, p=0.29). For the secondary endpoints, the change in the arterial TBR values in the bilateral carotid arteries and ascending aorta were numerically greater in the atorvastatin plus pioglitazone group than atorvastatin group but did not significantly differ between the groups (p=0.53, 0.14, and 0.47, respectively).
Patients with diabetes and an impaired fasting glucose
In our study, 22 patients (10 patients in the atorvastatin group and 12 patients in the pioglitazone plus atorvastatin group) had diabetes or an impaired fasting glucose level (fasting glucose ≥100 mg/dL). In those patients, the differences in the changes in the hsCRP and TBR within the index vessel between the 2 groups were also insignificant (Supplementary Table 2).
DISCUSSION
We assessed the effect of pioglitazone (30 mg/day) on the vascular inflammation of carotid arteries using serial FDG-PET/CT in stable CAD patients receiving atorvastatin (20 mg/day) with or without diabetes. Although a reduction in the FDG uptake by pioglitazone on top of atorvastatin in carotid arteries with a plaque was nearly statistically significant in the entire patients, pioglitazone showed a marked reduction of the FDG uptake of the vessels in the patients who had a baseline FDG uptake above the median.
Considering the complexity of the atherosclerotic disease process, myriad of effects of atorvastatin and pioglitazone, and ambiguity of pioglitazone (which has both plaque stabilizing and destabilizing effects19)), we employed FDG-PET/CT imaging, which is a useful surrogate biomarker for the evaluation of anti-atherosclerotic drug effects, to monitor the alterations in the vessel wall inflammation over drug treatment.15)17) Since the FDG uptake of calcified or small plaques is low or undetectable,20)21) we selected patients with non-calcified plaques of ≥3 mm for enrollment in this study. In previous trials, hsCRP was used as a marker for atherosclerotic inflammation14) which do not correlate with plaque inflammation on FDG-PET/CT in previous studies,15)17) only half of the patients received statins, and the exact statins and doses used were not described.12) In contrast, the present study enrolled statin-naïve patients, and all the patients were given fixed doses of atorvastatin to minimize the confounding factors.
The difference of carotid TBR by the addition of pioglitazone was smaller (ΔTBR=0.04) than we expected from the previous FDG-PET/CT trial examined pioglitazone12) and showed marginal significance. Although we enrolled statin-naïve patients with the inflammation prone carotid artery, our patients had relatively low inflammation activity of carotid artery (mean TBR=1.64) compared to other previous studies (mean TBR >2.0).22) In an exploratory analysis, pioglitazone showed more prominent anti-inflammatory effect (ΔTBR=0.1) in carotid arteries with high plaque activity (baseline TBR ≥1.65). A study17) which compared the anti-inflammatory effect between atorvastatin 80 mg and atorvastatin 10 mg enrolled patients who had the baseline TBR ≥1.6 based on another previous trial.15) In this study, atorvastatin 80 mg resulted in significant additional reductions in TBR by 0.1 compared to atorvastatin 10 mg. Considering clinical benefit of atorvastatin 80 mg over atorvastatin 10 mg, our result suggests that pioglitazone may be another option in high risk patients with CV events even after treatment with statins.
Although, guidelines recommend high-intensity statins in patients with documented CAD,23) some individuals may experience unacceptable adverse effects when taking the recommended intensity of statin, the most commonly reported being muscle-related symptom which may lead to statin discontinuation.5) Patients who are statin intolerant may be down-titrated and or considered to take non-statin treatment. Recently, anti-inflammatory therapies have been proposed to be the next promising therapy to reduce residual CV risk after statin treatment.6)24) The PPAR-γ agonist pioglitazone may be another potential anti-inflammatory drug in addition to statins.25) Indeed, in vivo studies have demonstrated that pioglitazone successfully reduces atheroma inflammation in animal models.26)27) Furthermore, high-dose potent statins cause adverse metabolic effects including worse insulin sensitivity and glucose intolerance that contribute to increased risk of new-onset diabetes. To optimize simultaneous CV and metabolic benefits while minimizing adverse events, a moderate dose of statins combined with PPAR-γ agonist may be a good option in patients with stable CAD.28)
Our study had several limitations. First, our small sample size might have limited our data interpretation. It is possible that the study was underpowered for testing the significant differences. However, we attempted to determine the sample size based on the results from a previous study,12) which was the only study that showed the effect of pioglitazone on reducing the vascular FDG signals in humans. Second, higher doses of pioglitazone might have provided clearer information regarding its anti-inflammatory effects on atherosclerotic plaque. However, we chose 30 mg/day of pioglitazone because higher doses are accompanied by side-effects. Moreover, higher doses are not typically prescribed in the clinic. Third, atorvastatin 20 mg, which is a moderate dose statin, is not the standard of care for secondary prevention. Therefore, it is unknown whether pioglitazone on top of a high-dose atorvastatin 80mg therapy would demonstrate additional anti-inflammatory benefits. Fourth, a TBR above the median analysis was not pre-specified. However, the subgroup analysis of a TBR above the median is an exploratory endpoint that suggests that pioglitazone would have particular efficacy for plaques that are highly inflamed. Fifth, this study was a single-center study and was not a double-blinded study. Larger multicenter outcome studies may be indicated to test pioglitazone in patients with sustained plaque inflammation despite statin therapy.
In conclusion, pioglitazone showed a potential to reduce plaque inflammation beyond a concomitant moderate dose statin in a serial FDG-PET/CT study of the arteries in patients with stable CAD. Pioglitazone could be an option to reduce the vascular inflammation in patients with sustained inflammation after statin treatment.
 XML Download
XML Download