

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Minimally invasive surgery, especially laparoscopy, has a significant place in gynecological oncologic surgery. Laparoscopic surgery creates a more tolerable postoperative period, decreases the analgesic requirement, shortens hospitalization time, and results in earlier recovery to normal activity compared with laparotomy [12]. Although laparoscopy is associated with less postoperative pain, this pain may continue for several days in the abdominal and shoulder areas. Many previous studies have shown that the incidence of shoulder or abdominal pain ranges from 35% to 80% [34]. Furthermore, nausea and vomiting commonly affect patients after laparoscopic surgery [5].
The mechanism of shoulder pain after laparoscopy remains unclear. Various mechanisms have been suggested, but the leading hypothesis is that carbon dioxide (CO2)-induced irritation of the phrenic nerve causes referred pain in the fourth cervical dermatome [67]. Other possible mechanisms include residual CO2 between the liver and right diaphragm, which irritates the diaphragm and strains the peritoneum [8910]. The most accepted method that seems to reduce shoulder pain after laparoscopic surgery is to discharge residual CO2 by performing the pulmonary recruitment maneuver (PRM) at the end of the surgical procedure [111213]. However, this maneuver should not be used in patients with hemodynamic instability, high intracranial pressure, and right heart failure [456789101112].
Several studies have suggested that the PRM improves postoperative pain scores and reduces the rate of postoperative nausea and vomiting among patients who have undergone gynecological surgery [5141516]. No study has examined the effect of the PRM on postoperative pain and nausea in patients undergoing gynecological oncologic surgery; the authors of the most recent meta-analysis concluded that an adequately powered randomized trial is mandated to address this issue [13]. Therefore, we designed this study to investigate the hypothesis that the PRM reduces the postoperative pain score and to evaluate any effect on postoperative nausea and vomiting in patients who have undergone laparoscopic gynecological oncologic surgery.
MATERIALS AND METHODS
This prospective, randomized study was performed at the Department of Gynecologic Oncology of the Muğla Sıtkı Koçman Üniversity, Istanbul Bakirkoy Sadi Konuk Education and Research Hospital and Izmır Tepecik Education and Research Hospital, Turkey, from October 2013 to December 2017. These tertiary teaching hospitals perform nearly 500 gynecological oncologic operations annually. Ethical oversight was provided by the local ethics committee. This trial was performed in compliance with the Declaration of Helsinki and was registered at clinicaltrials.gov (NCT01940042).
Inclusion criteria were female sex; age of 15–65 years; American Society of Anesthesiologists (ASA) physical status classification of I–III; lack of previous major abdominal surgery, such as bowel resection; and the need for laparoscopic surgery. Patients were excluded from the analysis when the procedure required conversion to laparotomy or when 48-hour follow-up was not feasible.
The women were randomized to groups A (PRM group) and B (control group) using a random number tables. The assigned treatments were written on cards and sealed in secure opaque envelopes numbered in sequence. The anesthesiologist opened each envelope just before surgery, and the allocation was recorded on each woman's chart. Only the anesthesiologist for the specific case was aware of the treatment allocation until the end of the surgical procedure, when the control treatment or the PRM was performed. The patient and the investigator who determined the postoperative score were blinded to the patient's group allocation.
All subjects received 0.2 mg glycopyrrolate intramuscularly as a premedication. General endotracheal anesthesia was induced with an intravenous injection of 2 mg/kg propofol, 1 mg/kg fentanyl, and 0.8 mg/kg rocuronium. The lungs were ventilated in a volume-controlled mode at a tidal volume of 8–9 mL/kg. Ventilation frequency was regulated to maintain an end-tidal CO2 partial pressure of 30–37 mmHg, and no positive end-expiratory pressure (PEEP) was used. Specialists in gynecological oncology (G.K. and Ö.İ.A.) performed all laparoscopic procedures using 4 ports. One 10- or 12-mm port was inserted through the umbilicus, and the other 5-mm ports were inserted through the lateral lower abdominal wall and suprapubic areas. Laparoscopy was performed using CO2 gas as the distention medium. CO2 was insufflated through a Veress needle at 20 mmHg pressure until all 4 ports were placed. Thereafter, the procedure was continued under 14 mmHg pressure with a CO2 flow rate <3 L/min. The patients were randomized upon completion of the procedure and divided into the standard care (control) and maneuver groups. In the control group, the residual gas pneumoperitoneum was evacuated passively at the end of the procedure by opening the operative ports to allow the abdomen to discharge. In the maneuver group, the patient was placed in the Trendelenburg position (30°) and the PRM, consisting of two manual inflations to a maximum pressure of 40 cmH2O, was applied in addition to standard care. The anesthetist performed the PRM, holding each positive pressure inflation for 5 seconds with the valves on the operative ports opened fully [14].
Our postoperative care protocol featured administration of the prokinetic agent metoclopramide 0.2 mg/kg intravenously (IV) as an antiemetic if required for, and prophylaxis for stress-induced gastritis in the form of histamine H2 blockers for 48 hours after surgery. Postoperative pain control was provided with 50 mg meperidine hydrochloride IV as needed within 12 hours after operation. Antiemetic agents were prescribed for nausea if required. Early ambulation was encouraged, and all patients were mobilized after assuming a sitting position for 10 minutes in bed to prevent hypotension, starting from 24 hours after surgery; patients walked approximately 5–10 m.
Postoperative blood pressure, heart rate, and respiratory rate were recorded at 4-hour intervals. Postoperative hospital stay (in days), meperidine use duration of postoperative hospital stay period, and were recorded. Flatulence relief time, which indicates the resumption of normal bowel function as expressed by the presence of bowel sounds and the passage of flatus, was also recorded. All data were recorded and analyzed by a researcher blinded to group assignment.
The primary outcome was the frequency and intensity of postoperative shoulder pain, and the secondary outcome was the rate of nausea and vomiting. Pain scores were determined at 12, 24, and 48 hours using a validated visual analog scale (0, no pain; 10, worst conceivable pain), rounded to the nearest whole number. Pain scores were determined verbally when the patient was illiterate. Pain in the shoulder, upper abdomen, and lower abdomen was assessed at rest. Lower abdominal pain was defined as a trocar wound or intra-abdominal pain. The investigator asked about the occurrence of nausea and vomiting. We estimated that the incidence of shoulder pain would be reduced from 80% to 50% by use of the PRM and determined that the required sample size was 45 patients per group for a 2-tailed χ2 test with 80% power and p=0.05, based on Phelps et al. [14]. An additional 10 subjects were recruited to account for possible drop-outs, so the recruitment target was 55 per group.
All statistical analyses were performed using MedCalc software (ver. 16.0 for Windows; MedCalc Software, Mariakerke, Belgium). The normality of the distribution of continuous variables was assessed using the Kolmogorov-Smirnov test, and the chi-squared test was used for categorical variables. Student's t-test was used to detect differences in normally distributed continuous variables, and the Mann-Whitney U test was used for abnormally distributed variables. Relative risk with the 95% confidence interval was calculated. p-values <0.05 were considered to indicate statistical significance.
RESULTS
In total, 113 women were randomly assigned to the PRM (n=57) and control (n=56) groups. Data from 54 women in the PRM group and 52 women in the control group were analyzed. The reasons for pre-randomization and post-randomization exclusion are shown in Fig. 1. Demographic and clinical characteristics, including maternal age, parity, operative time, surgery indication, type of surgery, postoperative hospital stay and flatulence relief time, were similar in the 2 groups (Table 1). The analgesic requirement and the incidence of postoperative nausea and vomiting did not differ (Table 1).

Table 1
Clinical characteristics of the study subjects
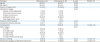
Data are shown as mean ± standard deviation or number (%).
CI, confidence interval; BMI, body mass index; BSO, bilateral salpingoophorectomy; PLN, pelvic lymphadenectomy; PPLND, pelvic and para-aortic lymphadenectomy; PRM, pulmonary recruitment maneuver; OR, odds ratio; TLH, total laparoscopic hysterectomy; TLRH, total laparoscopic radical hysterectomy.
![]()
The postoperative shoulder pain scores were significantly lower in the maneuver group than in the control group at 12 hours (2.2±0.5 vs. 4.0±0.5; p<0.001) and 24 hours (2.0±0.4 vs. 3.9±0.4; p<0.001) after the operation. No significant difference was observed between the groups at 48 hours (1.7±0.5 and 1.9±0.4; p=0.115). Similarly, shoulder pain and postoperative laparoscopy-induced upper abdominal pain scores were significantly lower in the maneuver group than in the control group at 12 hours (3.1±0.4 vs. 5.9±0.5; p<0.001) and 24 hours (2.9±0.4 vs. 4.9±0.5; p<0.001) after the operation, but did not differ at 48 hours (2.7±0.5 and 2.9±0.4; p=0.120). Lower abdominal (wound) pain scores did not differ between the 2 groups at 12, 24, or 48 hours (Table 2). No case was complicated by cardiovascular, pulmonary, or respiratory problems. The results of a literature review are shown in Table 3.
Table 2
Mean postoperative pain scores (visual analog scale score)

Data are shown as mean ± standard deviation.
PRM, pulmonary recruitment maneuver.
*Statistically significant.
![]()
Table 3
Review of the literature

| Outcome | Phelps et al. [14] | Sharami et al. [21] | Tsai et al. [15] | Tsai et al. [5] | Present study | |
|---|---|---|---|---|---|---|
| Type of study | RCT | RCT | RCT | RCT | RCT | |
| Patient number | 54 vs. 46 | 67 vs. 64 | 53 vs. 51 | 50 vs. 50 | 54 vs. 52 | |
| Type of operation | Minor laparoscopic procedures | Laparoscopic procedures for benign gynecological lesions | Laparoscopic procedures for benign gynecological lesions | Elective laparoscopic procedures for benign lesions | Elective laparoscopic procedures for premalignant or malign lesions | |
| PRM | ||||||
| No. of manual inflations | 5 | 5 | 5 | 5 | 5 | |
| Maximum inspiratory pressure (cmH2O) | 60 | 40 | 60 | 60 | 40 | |
| Pain scores 24 hr after the operation | ||||||
| Shoulder | 1.08±2.4 vs. 2.57±0.47 | 0.89±1.3 vs. 2.6±2.4 | 2.87±3 vs. 4.22±3.332 | 2.76±2.93 vs. 4.52±2.99 | 2.0±0.4 vs. 3.9±0.4 | |
| Upper abdomen | Not assessed | Not assessed | 3.85±3.15 vs. 5.61±2.82 | 4.64±2.95 vs. 5.90±1.95 | 2.9±0.4 vs. 4.9±0.5 | |
| Lower abdomen | Not assessed | Not assessed | 4.65±2.54 vs. 5.30±2.89 | Not assessed | 4.7±0.5 vs. 4.8±0.3 | |
| Nausea or vomiting (%) | 20.4 vs. 56.5 | Not assessed | 50.9 vs. 56.9 | 46.0 vs. 40.0 | 22.2 vs. 28.8 | |
| p-value of postoperative analgesic requirement (rate or amount) | Amount | Amount | Rate | Amount | Rate | |
| p=0.44 | p=0.01 | p=0.62 | p=0.209 | p=0.719 | ||
All comparisons are maneuver group/control group.
RCT, randomized controlled trial; PRM, pulmonary recruitment maneuver.
![]()
DISCUSSION
This randomized trial showed that laparoscopy-induced shoulder and upper abdominal pain occurred in the majority of patients after a minimally invasive procedure and that the PRM, with positive pressure of 40 cmH2O at the end of surgery, was associated with a significant reduction in the incidence of shoulder and upper abdominal pain, as well as pain scores at 12 and 24 hours (p<0.001). However, this intervention did not change the rate of analgesic use in relation to the control group after laparoscopic gynecological oncologic surgery. This study is the first to examine the use of the PRM in gynecological oncology.
Postoperative shoulder and upper abdominal pain can persist for several days and may disturb these patients more than pain in the lower abdomen. The most widely accepted hypothesis is that residual CO2 is the major contributor to shoulder pain. Kafali et al. [17] reported that pain was the most common cause of delayed discharge after day-case laparoscopy. Jackson et al. [18] first reported a correlation between the remaining volume of gas and pain severity. Fredman et al. [19] investigated removal of residual CO2 by active aspiration and manual compression of the abdominal wall to decrease postoperative pain. Tsimoyiannis et al. [20] reported that the removal of CO2 from the right subdiaphragmatic region by saline irrigation reduced shoulder pain after laparoscopic surgery. Finally we believe that the most important technique to reduce shoulder pain is to allow escape of the CO2 gas from the abdominal cavity at the end of surgery by performing forced maneuver.
Phelps et al. [14] demonstrated that the PRM effectively removes residual CO2 gas from the abdominal peritoneal cavity, eventually leading to low intra-abdominal acidosis as well as phrenic nerve and peritoneal irritation. They concluded that this maneuver effectively reduced shoulder pain severity from 61% to 31%. Sharami et al. [21] reported that the PRM reduced shoulder pain 4, 12, 24, and 48 hours after the operation. The main durations of surgery were 40 and 27 minutes. Tsai et al. [5] evaluated shoulder, upper abdominal, and lower abdominal pain, and obtained results similar to ours. Furthermore the use of a PRM in combination with low tidal volumes (6–8 mL/kg) and PEEP, is referred to as lung-protective ventilation, and is associated with improved clinical outcomes, such as a reduction of mortality after abdominal surgery [22]. However, our study has only focused on PRM, therefore tidal volumes of 7–9 mL/kg without PEEP were applied.
To perform the PRM in the present study, the patient was placed in the Trendelenburg position (30°) and 2 manual inflations were performed to a maximum pressure of 40 cmH2O. Our results were similar to those of Phelps et al. [14] and Sharami et al. [21], indicating that this maneuver significantly reduced shoulder and upper abdominal pain after 12 and 24 hours. Tsai et al. [5] reported that only upper abdominal pain was significantly reduced after the PRM; shoulder pain did not differ between the 2 groups. This difference from our results can be attributed to the different surgical type and duration in our study.
The most recent meta-analysis suggested that future studies should test the effect of the PRM on overall pain scores as well as the need for additional analgesia during the postoperative period [13]. We found that the analgesic requirement and the incidence of postoperative nausea and vomiting did not differ between groups. These results are similar to those reported by Tsai et al. [5]. Sharami et al. [21] reported that control patients required additional analgesic doses compared with an interventional group. They determined that the amount of analgesic agent required differed between the treatment and control groups.
All previous studies have involved minor or benign gynecological surgery. Kojima et al. [23] reported that injury to some tissues and bleeding during the procedure increased the risk of postoperative pain. Furthermore, Magnusson et al. [24] discovered that a longer duration of pneumoperitoneum was associated with more shoulder pain after surgery. The duration of surgery in our study was much longer than in all previous studies.
Many previous studies (e.g., Tsai et al. [5] and Phelps et al. [14]) involved the application of the maximum pressure of 60 cmH2O, which theoretically can cause pneumothorax [51415]. Ricard [25] reported that an alveolar recruitment maneuver of 40 cmH2O safely and effectively improved arterial oxygenation during anesthesia. Similarly, in a prospective study, Ryu et al. [26] demonstrated that the PRM using a maximal inspiratory pressure of 40 cmH2O is as effective as a 60 mmH2O for removing CO2 from the peritoneal cavity. Furthermore, Phelps et al. [14] and Sharami et al. [21] evaluated only shoulder pain. Finally, Radosa et al. [16], Phelps et al. [14], and Sharami et al. [21] performed minor or benign gynecological surgery, so the operation durations were very short. We inflated the lungs to 40 cmH2O in the present study. Additionally, we evaluated both shoulder and abdominal pain.
The strength of this investigation is that it was a prospective, randomized, multicenter clinical trial involving patients with similar demographic characteristics. In addition, this investigation was conducted at 3 tertiary referral centers specializing in gynecological oncology. Furthermore, experienced surgeons carried out all operations. The coauthor, who collected and analyzed the data, was blinded to the group assignments. These factors increase the validity of our results. However, the present study had several limitations. First, this is the relatively small sample size for looking at parameters such as the number of postoperative analgesic and antiemetic reguirements. Second, we excluded high-risk patients, such as those with ASA IV status and patients who had undergone surgery previously, because the risk of conversion to laparotomy would have been high and would have negatively affected the analysis. Third, different surgical types and durations could interfere with the pain evaluation, although there was no difference in the surgical type between the groups.
In conclusion, the present study demonstrated that a simple clinical maneuver significantly reduced shoulder and upper abdominal pain without increasing postoperative nausea and vomiting after laparoscopic gynecological oncologic surgery. The PRM can be implemented easily in daily clinical practice.
 XML Download
XML Download