

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
While early detection and advances in cancer treatment have facilitated steady increases in the survival of gastric cancer patients, improvement in the quality of life (QOL) after surgery continues to be pursued, even in the early postoperative period. Accordingly, minimally invasive surgery (MIS) to treat gastric cancer has garnered increasing popularity owing to more rapid recovery and shorter hospital stays after surgery than those after open surgery [12]. Apart from advances in surgical techniques, dedicated management tools such as exercise and dietary programs during the postoperative recovery can also be helpful in improving the QOL after surgery.
Exercise intervention after surgery has been found to improve physical fitness and QOL and to reduce treatment-related side effects in several organ cancers, such as breast, colorectal, prostate, and hematological malignancies [345678]. However, most studies have only assessed exercise intervention that is conducted after full recovery from surgery or on completion of treatment. No exercise program has been devised for use during the postoperative recovery, especially after MIS for gastric cancer. Thus, evidence is still lacking regarding the feasibility of applying exercise intervention to patients undergoing MIS for gastric cancer during the early postoperative period.
Accordingly, we developed a postoperative recovery exercise program developed specifically for gastric cancer patients (PREP-GC) after minimally invasive gastrectomy. This study investigated the safety and feasibility of the PREP-GC in gastric cancer patients who underwent MIS. Moreover, we evaluated and compared body composition, physical status, and QOL before surgery and after completing the PREP-GC.
MATERIALS AND METHODS
Study design
This study was designed as a prospective, single-arm, interventional study to assess the feasibility and effects of PREP-GC in gastric cancer patients after minimally invasive gastrectomy. PREP-GC consisted of sessions of In-hospital Exercise (1 week), Home Exercise (1 week), and Fitness Improvement Exercise (8 weeks). All patients were assessed preoperatively, after postoperative recovery (2 weeks after surgery), and upon completion of the PREP-GC (10 weeks after surgery). This study was reviewed and approved by the Institutional Review Board of Severance Hospital, Yonsei University College of Medicine (4-2012-0221) and registered with ClinicalTrials.gov (NCT01751880).
Patients
Patients were recruited between August 2012 and August 2013. Fig. 1 shows the flow of patient enrollment. The following criteria for patient inclusion were applied: 1) pathologically proven gastric adenocarcinoma, 2) age between 20–70 years, 3) preoperative diagnosis of early gastric cancer, 4) consent to undergo MIS (laparoscopic or robotic), 5) Eastern Cooperative Oncology Group score of 0 to 1, 6) no regular exercise during the previous 6 months, and 7) submission of signed informed consent to participate in the study. The following criteria were used for patient exclusion: 1) pregnancy or plans to become pregnant, 2) cognitive disabilities, 3) history of other primary cancer, 4) history of major abdominal surgery, or 5) presence of cardiopulmonary medical comorbidities. All patients were freely permitted to withdraw from the study at any time.

Surgery
All patients underwent laparoscopic or robotic gastrectomy. Five trocars were utilized for surgery, with a 10-mm trocar placed just below the umbilicus for a camera port and an additional 4 trocars for working ports. Standard radical subtotal or total gastrectomy with partial omentectomy and D1+ or more extended lymphadenectomy was performed on the basis of Japanese gastric cancer treatment guidelines [9]. After gastric resection, gastroduodenostomy, loop gastrojejunostomy, or Roux-en-Y esophagojejunostomy was performed intracorporeally. Resected specimens were retrieved through extension of an umbilical incision up to 3 cm.
Postoperative management
Following the operation, all patients with no serious comorbidities were sent to the general ward. A Foley catheter was indwelled after general anesthesia in the operating room and was removed on postoperative day 1. No nasogastric tube was inserted in any patient and a drain was inserted for selected patients. Postoperative pain control was achieved with intravenous patient-controlled anesthesia over the first 2 postoperative days. After these 2 days, intravenous painkillers were administered when required. When tolerated, water was given from postoperative day 2, a liquid diet was started on postoperative day 3, and a soft diet was started on postoperative day 4. Patients were discharged after 1 day of soft diet with no complications.
PREP-GC after minimally invasive gastrectomy
The exercise program was divided into 3 phases: In-hospital Exercise, Home Exercise, and Fitness Improvement Exercise (Fig. 2). In-hospital Exercise was conducted during hospitalization for 5 to 7 days. The exercises were chosen to facilitate anatomical adaptation and to help increase range of motion after minimally invasive gastrectomy. Patients were asked to perform each exercise for 5–10 seconds and were encouraged to perform a minimum of 2 sets of all exercises under the supervision of exercise specialists (SY and SS). Walking without supervision was encouraged as much as possible. The 1-week Home Exercise was designed to improve the range of motion after discharge from the hospital, without supervision. Patients were provided a handout illustrating the Home Exercise regimen, which exercise specialists used to educate patients. The patients were encouraged to complete the Home Exercise regimen more than once per day and to report their daily activity using an exercise log. By mainly focusing on resistance exercises, the Fitness Improvement Exercise was designed to improve reduction in muscle volume and function resulting from surgery. Patients were instructed to exercise 3 times a week at an appointed place and time with a small group of 1 to 2 patients under the supervision of accredited exercise specialists. Each session comprised a warm-up, a resistance exercise, and a cool-down phase. Patients were instructed to warm-up and cool-down for 10 minutes via low-level aerobic exercise and stretching before and after performing the resistance exercises. The 8 weeks of resistance exercise were divided into four 2-week periods, during which patients were to complete 4 different regimens of increasing strenuousness on the abdominal area. The resistance exercises included weight-bearing exercises, along with some upper-body work with dumbbells or elastic bands. During the Fitness Improvement Exercise phase, exercise specialists led patients to exercise at a perceived exertion of 12 to 14 (somewhat hard) on the Borg Scale [10].

Primary outcome measures
The safety of PREP-GC was assessed as the incidence of adverse events (AEs, any clinical symptoms and signs) on exercise. The feasibility of In-hospital Exercise was evaluated according to adherence to and completion of the planned exercise regimen. The feasibility of Home Exercise was determined by reviewing the patients' self-reports listing their daily performance and adherence to the prescribed exercise program. The feasibility of the Fitness Improvement Exercise was evaluated in terms of adherence and compliance to the exercise regimen. Adherence was defined as the number of completed sessions relative to the number of scheduled sessions with the exercise specialist. Compliance to each component was defined as the completion of exercises for the prescribed duration, frequency, and intensity as assessed by the exercise specialists. Any modification to the duration, frequency, or intensity of any exercise was considered as non-compliance.
Secondary outcome measures
Anthropometric parameters
All anthropometric parameters were measured by the same individual. Height and weight were measured to the nearest one decimal point. Circumference was measured according to the procedures outlined by the American College of Sports Medicine (ACSM) at the following 7 sites: abdomen, waist, upper arm, lower arm, hips, thigh, and calf. Subcutaneous fat thickness was measured at the following 7 sites: chest/pectoral, midaxillary, abdominal, suprailiac, subscapular, triceps, and thigh muscles. The technical error of all measurements was less than 0.3 mm [11]. The percent body fat was calculated using the 7-site Jackson Pollock skinfold equation [12].
Fat and muscle volume measurement using computed tomography (CT)
To determine standard CT values for muscle and fat volume, muscle CT cross-sectional areas of whole muscular components at each section and fatty CT cross-sectional areas of visceral and subcutaneous fat were obtained (Fig. 3). Regions of interest were drawn at a pre-specified level, including the whole muscle, to generate region of interest values. Data were acquired with a Multi-Detector Row CT scanner (Somatom Sensation 64 and 128, Siemens Medical System, Erlangen, Germany; Light Speed VCT 64 or Discovery 750-HD 64, General Electric Medical Systems, Milwaukee, WI, USA). Cross-sectional areas were measured at the levels of T11-12, L2-3, L3-4, and L4-5. CT imaging was performed with a 512×512 matrix and a tube voltage of 120 kV. CT values were transferred to commercial three-dimensional software (Aquarius iNtuition, version 4.4.11, TeraRecon, California, CA, USA) and analyzed.

Physical fitness measurement (cardiopulmonary function and muscular endurance, strength, and flexibility)
To measure cardiopulmonary function, a cardiopulmonary exercise test using a modified Bruce protocol was utilized [13]. Prior to testing, the resting heart rate, blood pressure, and electrocardiograms (ECG) were recorded. After the beginning the exercise session, 12-lead ECG, heart rate, blood pressure, and rating of perceived exertion (Borg 6 to 20 scale) assessments were taken at 3-minute intervals. Patients were instructed to perform each test for as long as possible to ensure a true maximal attempt. Standard ACSM test termination criteria were monitored and followed throughout each test [11]. Breath-by-breath data were collected using a K4B2 Metabolic Measurement System (Cosmed, Rome, Italy) using real-time analysis.
To measure muscular endurance, a chair stand test and wall half squat test were used. The chair stand test was conducted to assess leg strength and endurance and measured the number of times a person could rise from a chair in 30 seconds [14]. The wall half squat test was administered to assess leg strength, targeting the quadriceps muscle. To perform the exercise, the participant assumed a sitting position with their back against a wall, feet flat on the ground, at a 90° angle at the hips and knees for as long as possible [15].
Muscular strength was measured by grip strength. To test grip strength, patients stood with their upper limbs relaxed down to the sides of their body and with their palms toward the torso. The elbow was extended without any flexion. The patients were then encouraged to exert their maximal grip [16]. The maximum force in kilograms was taken after 2 consecutive attempts in each hand using a dynamometer (TTM, Tokyo, Japan).
To measure flexibility, a back-stretch exercise and a sit-and-reach exercise were used. The back-stretch exercise measured upper arm and shoulder girdle flexibility, whereas the sit-and-reach test measured lower flexibility.
QOL
QOL was assessed using validated Korean versions of the European Organization for Research and Treatment of Cancer Core Quality of Life Questionnaire (EORTC QLQ-C30) and the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-Stomach Cancer-Specific Module (EORTC QLQ-STO22) [1718]. All scales and single item measures ranged in score from 0 to 100. Missing values were processed as recommended in the EORTC QLQ-C30 scoring manual [19].
Statistical analysis
Data are expressed as mean±standard deviation (SD) or frequency (percent). Data were evaluated using repeated-measures analysis of variance (ANOVA) to assess differences in study outcomes at the 3 assessment points (preoperative period, 1 week after discharge, and after completing PREP-GC). Outcomes for which only 2-time points were available were analyzed using Student's t-test. A P-value less than 0.05 was considered statistically significant. All analyses were performed using IBM SPSS Statistics, version 20 (SPSS Inc., Chicago, IL, USA).
RESULTS
Patients
Initially, 24 patients agreed to participate in the study and underwent baseline assessment. Of these, 4 patients dropped out of the study: 3 patients withdrew due to difficulty with traveling to the place of exercise intervention after baseline assessment, during the Home Exercise program, and after the follow-up assessment at 1 week after discharge, respectively; the other patient was excluded due to advanced disease requiring adjuvant chemotherapy. Finally, 20 patients completed the PREP-GC and were included in the analyses of body composition, physical fitness, and QOL (Table 1).
Table 1
Patient demographics and clinicopathological features

![]()
The patients who completed PREP-GC (n=20) were aged 30–64 years (mean, 45.9 years). Eleven patients were male (55%) and 9 were female (45%). The mean body mass index (BMI) was 24.0±3.2, and most patients (70%) were overweight or obese (BMI >25 kg/m2). The majority of patients underwent robotic surgery (60%), subtotal gastrectomy (95%), or gastroduodenostomy (60%). Because all of the patients were diagnosed with early gastric cancer preoperatively, D1+ lymphadenectomy was primarily performed (95%). There were no complications higher than grade III according to the Clavien-Dindo classification [20] and no deaths reported.
Safety and feasibility
None of the patients who participated in PREP-GC experienced any AEs related to the exercise program. During the In-hospital Exercise phase, all patients (n=22) participated in and finished the planned exercise program without modification (adherence and compliance rates of 100%). During the Home Exercise phase (n=21), 16 patients completed the prescribed exercise program; 4 patients completed the exercise program with modification; and one did not perform any of the exercises (adherence and compliance rates of 95.2% and 80%, respectively). During the Fitness Improvement Exercise (n=20), 14 patients (70%) participated in over 20 of the 24 scheduled exercise sessions (mean±SD, 22.4±1.3). The adherence to the Fitness Improvement Exercise was 79.4%±23.9%. An adherence greater than 80% was recorded for 14 patients, while adherence of 60%–79%, 40%–59%, and <40% was recorded for one, three, and 2 patients, respectively. Six patients recorded below-average attendance with a mean adherence rate of 45% for different reasons: having gout (n=1), not interested in the program (n=1), planned a long-term overseas trip (n=1), and had an early return to work (n=3). With the exception of these 6 patients, 14 patients attended 93.5% of the exercise sessions.
Nine patients completed the Fitness Improvement Exercise regimen without any modification, whereas 11 patients completed it with modifications. Only 17 (0.6%) of the total 2,908 exercise components performed were modified during the Fitness Improvement Exercise phase. Compliance during the Fitness Improvement Exercise was 99.4%. Three modifications were recorded for a single patient, while 2 modifications and a single modification were observed for 4 and 6 patients, respectively. Major reasons for modification were incision site pain caused by “side bend” and dizziness. Nevertheless, the patients continued to follow the Fitness Improvement Exercise without exacerbation of symptoms. Other reasons for modification included pre-existing medical conditions before surgery, such as intermittent arthralgia.
Changes in body composition and physical fitness
Body weight decreased significantly during postoperative recovery (61.6±10.2 kg) and after completing the PREP-GC (60.6±9.9 kg) compared to the preoperative period (65.1±11.8 kg) (P<0.001). Skinfolds and circumferences at all sites were also significantly reduced after completion of the PREP-GC (P<0.05), except for the circumference of the lower arm. Thigh circumference measurement was significantly higher after completion of the PREP-GC than during postoperative recovery (2.61%±5.4%, P<0.05), although it was still significantly less than that in the preoperative period (4.56%±5.5%, P<0.001) (Fig. 4).
 | Fig. 4Changes in body composition and physical fitness. (A) Body weight and BMI. (B) Fat and muscle volume based on CT. (C) Circumference measurements at each site. (D) Skinfold measurements at each site.BMI = body mass index; CT = computed tomography; PREP-GC = postoperative recovery exercise program developed specifically for gastric cancer patients.
*P<0.05 versus preoperative period; †P<0.05 versus after postoperative recovery.
|
Both visceral fat and subcutaneous fat volumes on CT images decreased at all measured levels upon completion of the PREP-GC compared to the preoperative period. In particular, statistically significant decreases were observed for visceral fat and subcutaneous fat at level L4–5 and subcutaneous fat at level L3–4 (P=0.011, 0.029, and 0.034, respectively). Meanwhile, no significant differences in muscle volumes were recoded between the preoperative period and upon completion of the PREP-GC at any measured level.
All parameters related to physical fitness changed significantly upon completion of the PREP-GC. Compared to that during the preoperative period, the peak oxygen consumption (VO2 peak) significantly decreased during postoperative recovery and then increased to the preoperative level upon completing the PREP-GC. The chair stand, wall half squat, and sit and reach measurements significantly decreased in the postoperative recovery period and significantly increased upon completion of the PREP-GC, compared to baseline measurements (Table 2).
Table 2
Effects of the PREP-GC on physical fitness

The P-values indicate analysis of variance results.
PREP-GC = postoperative recovery exercise program developed specifically for gastric cancer patients; VO2 peak = peak oxygen consumption.
*P<0.05 versus preoperative period; †P<0.05 versus after postoperative recovery.
![]()
Changes in QOL
Global health status reduced significantly during the postoperative recovery period and improved upon completion of the PREP-GC when compared to the preoperative period (Fig. 5). Emotional functioning improved significantly upon completing the PREP-GC compared to the preoperative and postoperative recovery periods. The other functional measures all declined after postoperative recovery, but recovered upon completing the PREP-GC. Fatigue, nausea and vomiting, pain, and dyspnea scores on symptoms scales were highest after the postoperative recovery period but recovered to scores similar to those in the preoperative period upon completing the PREP-GC. Appetite loss scores were significantly lower upon completing the PREP-GC than those after postoperative recovery; there were no differences between appetite loss scores during the preoperative period and after completing the PREP-GC. Moreover, scores for dysphagia, abdominal pain, and disorders of taste increased significantly after postoperative recovery compared to the preoperative period, although they recovered upon completing the PREP-GC.
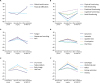 | Fig. 5Changes in QOL. (A, B) Mean changes in QOL score by EORTC QLQ-C30. (C-F) Mean changes in EORTC QLQ-STO22.QOL = quality of life; EORTC QLQ-C30 = European Organization for Research and Treatment of Cancer Core Quality of Life Questionnaire; EORTC QLQ-STO22 = European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-Stomach Cancer-Specific Module.
*P<0.05 versus preoperative period; †P<0.05 versus after postoperative recovery.
|
DISCUSSION
In the present study, we found that PREP-GC was safe and feasible for use in gastric cancer patients who underwent minimally invasive gastrectomy, with a high adherence and compliance rate and no AEs. Compared to preoperative measurements, anthropometric parameters, and muscle volumes were well preserved with the PREP-GC, whereas fat volumes significantly decreased. Moreover, completion of the PREP-GC recovered and improved physical fitness status and QOL.
Adherence and compliance rates to the PREP-GC were high and similar to those reported in previous studies on patients undergoing abdominal surgery [42122] and to the rates derived from a systematic review on the health effects of exercise during cancer rehabilitation [23]. Notwithstanding, the subjects in these previous studies were all cancer survivors who had completed treatment. The high adherence in our study is important as the exercise intervention was conducted beginning from the early postoperative period. Achieving high adherence was possible owing to the advantages of MIS, tailoring the exercise program specifically for gastric cancer patients, and the supervision by an exercise specialist of the program. MIS facilitates reduced postoperative pain and early functional recovery [24], making early exercise intervention feasible. The specialized exercise program, comprising tension-free motion at the upper abdomen and maintenance of erect movements to prevent esophageal regurgitation, allowed participants to complete the exercise regimen without any AEs. Additionally, the exercise specialists ensured proper physical form and provided emotional support throughout the program. Nevertheless, we found that side bend caused some incision site pain, which reduced compliance and might have resulted in potential adverse effects. Therefore, we suggest that the side bend motion be limited and applied carefully during the early postoperative period after upper abdominal surgery.
In this study, we found that the relative VO2 peak and the absolute VO2 peak values decreased by approximately 15% and 20%, respectively, during postoperative recovery. Studies have established that exercise training can improve these values by about 15%–20% in healthy middle-aged individuals [25]. Upon completing the PREP-GC, we also observed improvements of about 23% in relative VO2 peak and 21% in absolute VO2 peak. Therefore, we suggest that early gastric cancer patients subjected to MIS can experience improvements in cardiopulmonary function similar to those in healthy individuals. Another unique finding of this study was that the PREP-GC led to clinically important improvements in muscular endurance. Of particular note, patients in this study not only showed recovery of their physical fitness with a return to baseline levels but also exhibited improvements above their preoperative measurements, despite body weight loss.
In this study, muscle volumes measured on CT scans were well preserved after completing the PREP-GC, even though the patient's total body weight decreased as also observed in most studies [262728]. Muscle mass reportedly decreases significantly in the early postoperative period, failing to recover to baseline levels at 6 months after a gastrectomy [26]. In the present study, the mean weight loss was 4.59 kg (7.2%), which is similar to that in previous reports. However, muscle volumes at 10 weeks after surgery completely recovered to their preoperative level. This finding suggests that early postoperative exercise could prevent muscle volume consumption, thereby maintaining muscular strength, endurance, and function.
According to a comparative study on QOL after gastrectomy, most function and symptom scales do not recover until 6 months after surgery [2930]. Moreover, a randomized controlled study on QOL after gastrectomy showed a better QOL is achieved for patients undergoing laparoscopy-assisted gastrectomy compared to open surgery; nevertheless, most QOL parameters still did not return to their baseline levels at 90 days after surgery [27]. Our newly developed systemic postoperative exercise program, however, provided full recovery of baseline QOL within 10 weeks after MIS. Accordingly, we suggest that exercise starting from the early postoperative period could facilitate faster recovery of QOL after minimally invasive gastrectomy.
At present, we believe this study to be the first prospective interventional study to validate the safety and feasibility of an exercise intervention program designed specifically for gastric cancer patients undergoing gastrectomy using a comprehensive assessment of anthropometric parameters, body composition using CT scan, physical fitness, and QOL. As a distinctive feature of our study, we enrolled patients who underwent MIS of the upper abdomen in exercise intervention from the very early postoperative period (postoperative day 1). Despite the positive findings, this study has several limitations. Because this was a single-arm, non-comparative study, we could not evaluate the benefits of PREP-GC in comparison to no exercise intervention. Currently, we are carrying out a randomized controlled study (NCT01637909) to address this limitation. Furthermore, we only included patients undergoing MIS without any scheduled chemotherapy. Additionally, the majority of the enrolled patients were young, well-educated, and lived in a large city, which limits the generalizability of our results. A study with expanded inclusion criteria for patients, such as older age, conventional open surgery, and receiving chemotherapy, should be performed in the future. Additionally, diet and routine physical activity were not measured and controlled for in this study. Future studies addressing these issues will provide more precise evaluation of the effects of PREP-GC after surgery.
In conclusion, we found our newly developed postoperative exercise program, PREP-GC, to be feasible and safe, facilitating the recovery and improvement of physical fitness and QOL after MIS for gastric cancer patients. For improved care of gastric cancer patients after minimally invasive gastrectomy, surgeons should encourage gastric cancer patients to participate in systematic exercise intervention programs in the early postoperative period. Meanwhile, results from randomized studies evaluating the benefits of exercise intervention during postoperative recovery are needed.
 XML Download
XML Download