

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Distal subtotal gastrectomy and proper lymphadenectomy are common surgical strategies used for treatment of gastric cancer affecting the middle or distal stomach, where gastric cancers commonly occur [1]. The selection of an appropriate reconstruction method after distal subtotal gastrectomy is very important, because reconstruction tends to affect the remnant stomach and the quality of life of patients [2]. The standard methods of reconstruction are gastroduodenostomy, also termed Billroth-I (B-I) reconstruction, and gastrojejunostomy, also termed Billroth-II (B-II) reconstruction, both of which involve a single anastomosis. Most surgeons prefer B-I reconstruction because it retains the physiologic passage of the ingested food, as long as it is anatomically possible [3]. However, the major disadvantage of B-I reconstruction is the reflux gastritis caused by the loss of the pylorus, which is the anatomical barrier preventing the reflux of bile into the stomach, and the reflux of bile eventually increases the risk of cancer in the remnant stomach [4]. In addition, the reflux of bile into the remnant stomach can affect the quality of life of patients after gastric cancer surgery [5]. Therefore, many surgeons have found Roux-en-Y (R-Y) reconstruction more favorable than B-I reconstruction due to the decreased likelihood of bile reflux [678]. In spite of these benefits, surgeons are reluctant to widely use the R-Y reconstruction method clinically because of some drawbacks of this method.
The R-Y reconstruction after distal gastrectomy requires 2 anastomoses, i.e., for the gastrojejunostomy and for the jejunojejunostomy, because this method involves the resection of a portion of the small intestine and its mesentery. The need for these complicated procedures has emerged as a major disadvantage of the R-Y reconstruction method. Several clinical studies have shown that R-Y reconstruction takes more time and has a higher complication rate than other methods [910]. To overcome these shortcomings, we performed a pilot study for developing a novel and simple method using 2 circular staplers for R-Y reconstruction; our results showed that compared with the B-I method, this method was safe, and it reduced the incidence of postoperative bile reflux [11]. However, to recommend this procedure as a novel method instead of conventional reconstruction method, a prospective randomized controlled clinical trial (RCT) was necessary to show the superiority of this method to the B-I method with respect to prevention of bile reflux into the remnant stomach and the safety of this procedure. To assess the effect of R-Y reconstruction on bile reflux as objectively as possible, we used three types of measurements, namely the results of histological examination, gastroscopic findings, and the quality of life of enrolled patients. Here, we present the results of this RCT conducted to evaluate the efficacy of the simple R-Y reconstruction method involving the use of 2 circular staplers.
MATERIALS AND METHODS
The institutional review board of the Ajou University Hospital, Suwon, Korea approved this RCT (AJIRB-MED-DEO-09-297); this study followed the ethical standards of the Helsinki Declaration of 1975. This study was registered at www.clinicaltrials.gov as NCT01142271 before enrollment of the first patient, and written informed consent was obtained from each patient prior to inclusion.
The patients were randomly assigned into two groups before the surgery: the B-I or R-Y reconstruction group. The patients and surgeons were not blinded to the randomized allocation, whereas the investigators and data collectors were blinded during the trial.
Patients were assessed for this RCT if they met the following inclusion criteria: gastric adenocarcinoma diagnosis, age between 25 and 74 years, primary tumor located in the middle or distal portion of the stomach that could be curatively resected using distal gastrectomy, and American Society of Anesthesiology (ASA) score of ≤3. Patients who were pregnant or those with uncontrolled systemic disease or synchronous malignancy were excluded from this trial. From July 2010 to November 2011, 120 patients were assessed for determining their eligibility for this trial.
Two surgeons (Sang-Uk Han and Hoon Hur), both with an experience of over 100 surgeries for gastric cancer when this trial began, performed surgery in all participants. The surgeries were performed according to the third edition of Japanese Gastric Cancer Treatment Guideline [12]. Laparoscopic surgery, including limited lymph node dissection (less than D1+), was performed according to the formal protocol of our institution in patients who were clinically diagnosed with early gastric cancer. For the laparoscopic surgery, a small incision (4–6 cm) was performed in the epigastric area to allow easy reconstruction after laparoscopic lymph node dissection. For patients from B-I group, gastroduodenostomy was performed according to the Tonado method using a 29-mm circular stapler (Ethicon Endosurgery Inc., Blue Ash, OH, USA), which has shown favorable results in a previous study reported by Yang et al. [13]. The methods for R-Y reconstruction were described in detail in our pilot study [11]. Briefly, we resected a portion the jejunum and its mesentery 30 cm distally from the Treiz ligament (Fig. 1A), and the anvil of a 21-mm circular stapler (Ethicon Endosurgery Inc.) was inserted into the proximal end of the resected jejunum (Fig. 1B). For the jejunojejunostomy, the body of 21-mm circular stapler was inserted into the distal end of the resected jejunum and passed through the Roux limb into the site of the jejunojejunostomy (Fig. 1C). With the Roux limb measuring >30 cm, the jejunojejunostomy was performed (Fig. 1D). Thereafter, the larger anvil of the 29-mm circular stapler (Ethicon Endosurgery Inc.) was placed at the distal end of the resected jejunum (Fig. 1E), and the gastrojejunostomy was performed in a manner similar to the Tonado method (Fig. 1F).
Fig. 1
Surgical procedure for R-Y reconstruction included (A) division of the proximal jejunum and mesentery, (B) insertion of a 21-mm anvil into the resected distal jejunum, (C) insertion of the stapler body into the resected proximal jejunum, (D) anastomosis of jejunojejunostomy using a 21-mm circular stapler, (E) insertion of a 29-mm anvil into the proximal jejunum, and (F) anastomosis of the gastrojejunostomy by using the Tonado method with a 29-mm circular stapler.
R-Y = Roux-en-Y.

The primary end-point of this RCT was the reflux of bile into the remnant stomach at 6 months after surgery. Therefore, the patients underwent gastroscopy, and the degree of bile reflux was evaluated as per the classification suggested by Japanese surgeons [7]. With regard to residual food, grade 0 denoted no residual food, grade 1 denoted a small amount of food, grade 2 denoted a moderate amount of food with the entire surface of the remnant stomach visible, grade 3 denoted a high amount of food with some part of the remnant stomach visible, and grade 4 denoted non-visualization of the remnant stomach. Further, grade 0 gastritis denoted normal mucosa; grade 1 denoted mild redness; grade 2 denoted intermediate state; grade 3 denoted severe redness; and grade 4 denoted apparent erosion. Bile reflux was graded as grade 0 (absence) or grade 1 (present). Additionally, we determined the histological degree of bile reflux using specimens of the remnant stomach that were obtained during endoscopic biopsy. Histological grading of the specimen was carried out according to a previous report by Dixon et al. [14], considering the elongation and tortuosity of the glands, interstitial edema or congestion, paucity of chronic inflammatory cells, and the prominence of the smooth muscle cells in the lamina propria (Fig. 2). Two pathologists determined the score from point 0 to 3 in terms of hyperplasia or congestion of the laminar propria, and acute or chronic inflammation.
Fig. 2
Histological findings of biopsied tissues in the remnant stomach. (A) The tissue received a score of 0 on evaluation, as per the grading system suggested by Dixon et al. [14]. (B) The tissue received a score of 12.

The secondary outcomes were morbidity and mortality related to the surgery, the operation and reconstruction time, and quality of life scores determined using the European Organization for Research and Treatment of Cancer Quality Life Questionnaire-Core-30 (EORTC QLQ-C30) and a specific questionnaire for gastric surgery (QLQ-STO22) at 6 months after surgery.
The aim of this study was to show the superiority of the novel R-Y reconstruction method over the B-I method with respect to the incidence of bile reflux into the remnant stomach after distal gastrectomy as the primary end-point. We used a standard superiority design, and the sample size was estimated considering the following points: a 2-sided significance level of 0.05, 80% power, χ2 test results, and an alternative hypothesis based on the reflux rate of primary end-points of 10% in the R-Y group vs. 30% in the B-I group. The reflux rates were based on the results of a previous study by Ishikawa et al. [15]. Considering a 10% drop rate, 120 patients were necessary to detect any significant difference between the 2 groups.
Sample size was calculated using Excel 2011 (Microsoft Corp., Redmond, WA, USA), and statistical analysis was conducted using the SPSS version 18.0 (IBM Corp., Armonk, NY, USA). To compare the outcomes between the 2 groups, the Student's t-test and χ2 test were conducted for continuous variables and absolute variables, respectively. The continuous variables were expressed as means±standard deviations. Statistical significance was set at P<0.05.
RESULTS
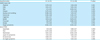
The recruitment and progression of this clinical trial are summarized in Fig. 3. Of 120 selected patients, 118 patients who agreed to participate in this trial were randomized. A total of 59 patients were allocated to each group. Of the 59 patients allocated to the B-I group, three patients underwent other methods of reconstruction using other methods, such as R-Y and B-II, because the length of the remnant stomach was too short for performing reconstruction via gastroduodenostomy. We performed total gastrectomy in one patient in the R-Y group to secure a tumor-free proximal margin. Finally, 56 patients in the B-I group and 58 in the R-Y underwent the allocated procedures. The clinicopathological and surgical characteristics of these patients are listed in Table 1. No major differences were observed between the 2 groups. Subsequently, the surgical outcomes were compared between the 2 groups.
Fig. 3
Study design according to the CONSORT diagram.
CONSORT = Consolidated Standards of Reporting Trials; B-I = Billroth-I; B-II = Billroth-II; R-Y = Roux-en-Y.

Table 1
Demographic and clinical characteristics of included patients according to the performed procedure
At the 6-month follow-up, 8 (6.7%) patients were lost to follow-up, 5 from the B-I group, and 3 from the R-Y group. Finally, the primary end-points occurred in 106 (89.8%) of 118 patients assessed in this trial, 51 from the B-I and 55 from the R-Y group. Their data were analyzed to compare the primary end-points of the 2 groups.
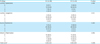
No significant difference in the surgical outcomes, such as intraoperative bleeding, the length of hospital stay, postoperative recovery time, and postoperative complication rate was found between the 2 groups (Table 2). Although most complications were resolved via medical or conservative treatment, reoperation was necessary in one patient with anastomosis leakage from the R-Y group. However, the patient fully recovered, and no mortality was reported in both groups.
Table 2
Surgical outcomes of patients according to performed procedure

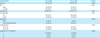
The time taken to perform the reconstruction was significantly longer in the R-Y group than in the B-I group (34.3 vs. 29.0 minutes, P<0.001). However, no statistical difference was detected in total surgery time between the 2 groups (P=0.112). The quality of life score at 6-month follow-up, determined using European Organization for Research and Treatment of Cancer (EORTC) questionnaires, was not significantly different between the 2 groups (Table 3).
Table 3
Change in quality of life of patients who were followed up 6 months postoperatively using EORTC questionnaires
Continuous variables were calculated as the ratio of score of the postoperative 6-month score to the preoperative score and presented as mean±standard deviation.
EORTC = European Organization for Research and Treatment of Cancer; B-I = Billroth-I; R-Y = Roux-en-Y; QLQ-C30 = Quality of Life Questionnaire-Core 30; QLQ-STO22 = Quality of Life Questionnaire-Stomach Cancer Module 22; GI = gastrointestinal.
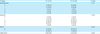
The gastroscopic finding showed that the reflux of bile in the remnant stomach was significantly reduced in the R-Y group compared with in the B-I group (23.6% vs. 62.7%, P<0.001). Gastritis in the remnant stomach was more severe in the B-I group than in the R-Y group (P=0.016) (Table 4). However, the findings regarding residual food in the remnant stomach were similar between the R-Y and B-I groups (P=0.117).
Table 4
Gastroscopic findings for patients who were followed up 6 months postoperatively using the RGB score
Histological evaluation was performed using biopsied specimens from 79 patients who agreed to undergo biopsy of the remnant stomach. Although no difference was found between the 2 groups when the scores were itemized for hyperplasia, congestion, and inflammation, the total score was higher in the B-I group than in the R-Y group (5.05 vs. 3.93, P=0.026) (Table 5), thereby showing the superiority of R-Y over B-I in preventing histological gastritis.
Table 5
Histological findings for the remnant stomach in patients who were followed up 6 months postoperatively using the scoring system suggested by Dixon et al. [14]
DISCUSSION
This RCT showed the efficacy of the novel R-Y reconstruction method involving the use of 2 circular staplers and no hand sewing after distal gastrectomy in gastric cancer surgery. Compared with the conventional B-I method, the novel R-Y reconstruction method did not yield poor surgical outcomes. Moreover, our postoperative endoscopic and histologic findings showed the superiority of the R-Y reconstruction method in preventing the bile reflux into the remnant stomach.
In this RCT, we introduced a novel method of using only staplers to make the relatively complicated R-Y procedure after distal gastrectomy as easy as the conventional B-I or B-II method. Currently, many surgeons are using staplers for performing anastomoses because they are safe and time saving; these advanced instruments facilitated the novel procedure in this study as well. To date, several studies have shown that using advanced stapling devices reduces the incidence of complications, such as leakage and bleeding; in addition, stapling makes anastomosis of the intestine easier and more secure than hand sewing [161718]. The advantage of using a stapling device is particularly evident in complicated procedures, such as the conventional R-Y reconstruction that requires many anastomoses. Because we used circular staplers for performing 2 anastomoses, we found it difficult to combine the anvils and the body of the staplers without an additional enterotomy. To overcome this problem, the body of a 21-mm stapler for the jejunojejunostomy was first inserted through the distal opening of the resected jejunum, and it was passed through 30–40 cm of the jejunum to combine it with the anvil fixed to the proximal end of the resected jejunum. Subsequently, the body of a 29-mm stapler for the gastrojejunostomy was inserted through the resected part of the stomach to combine it with the anvil inserted into the distal end of the resected jejunum; this procedure was not difficult because it was similar to the Tonado method for B-I reconstruction. Since additional hand sewn sutures for anastomosis were not required, the total operation time was not significantly longer than that for the B-I method that requires only one anastomosis. In addition, the operation time for patients from the R-Y group in this study was shorter than that observed in R-Y reconstruction in previous reports [715]. The acceptable operation time for R-Y reconstruction could have led to favorable surgical outcomes, with no major differences in the complication rate, length of hospital stay, and diet schedule between the R-Y and B-I groups.
In this RCT designed to prove the efficacy of the novel, yet simple procedure, we also determined whether this novel procedure could retain an important benefit of conventional R-Y reconstruction, i.e., prevention of bile reflux. Bile reflux into the remnant stomach after distal gastrectomy is usually detected by 24-hour bilirubin monitoring or biliary scintigraphy [819]. However, we used endoscopic and histological findings, because these findings would directly reflect the damage to the mucosal layer of the remnant stomach from the refluxed bile. Although different anastomotic procedures have been used in other studies, R-Y reconstruction has been shown to have improved gastroscopic and histological findings in the remnant stomach after distal gastrectomy compared with B-I or B-II reconstruction [2021]. To maintain objectivity in the evaluation of bile reflux into the remnant stomach in this RCT, the gastroscopic findings were examined by both a gastroenterologist and a surgeon. We classified the endoscopic findings into food stasis, mucosal gastritis, and bile presence, according to a previous report [7], to determine whether the patients experienced stasis of food in the remnant stomach along with the bile reflux. In addition, the degree of histological changes in the remnant stomach is an important measurable outcome for the bile reflux. Dixon et al. [14] classified the severity of reflux gastritis according to histological findings and found that the severity of reflux gastritis was correlated to the degree of alkalinity in the stomach. Two pathologists scored the biopsied specimens from the remnant stomach 6 months after surgery; their findings also demonstrated the superiority of R-Y reconstruction in the prevention of reflux gastritis.
In addition to the distinct drawback of the conventional R-Y reconstruction method as being a complicated procedure, the Roux stasis syndrome can also pose a serious postoperative problem [722]. This syndrome is characterized by epigastric discomfort and even pain after consuming food. This drawback cannot be addressed by our procedure using staplers because the problem is caused by the poor motility of the Roux limb after division of the jejunal mesentery. Therefore, we advised the patients of both groups to consume a small amount of food at a time during the immediate postoperative three months. Ultimately, the gastroscopic findings for food stasis did not show significant differences between the B-I and R-Y groups, and no patient from the R-Y group complained of symptoms related to Roux stasis syndrome. On the other hand, three patients from the R-Y group were treated for postoperative ileus as opposed to only one patient in the B-I group. Some physiological studies on intestinal motility have reported that the separation of the jejunum from the natural small intestinal pacemaker located in the duodenum could be the cause of decreased motility [2324]. However, there was no significant difference in the incidence of postoperative ileus between the 2 groups, and all three patients with ileus from the R-Y group were managed using conservative treatment only.
Postoperative quality of life is an important outcome to be considered when deciding on the reconstruction method after distal gastrectomy. Therefore, we evaluated the quality of life using the EORTC QLQ-C30 questionnaire, which was already well validated [2526]. This questionnaire helps researchers to analyze the physical, psychological, and social views of patients with cancer. However, more specialized questionnaires are necessary to examine the quality of life of patients after gastrectomy; therefore, we also used the EORTC QLQ-STO22 questionnaire that has several questions about gastrointestinal symptoms. Because gastrectomy has a temporary effect on the quality of life of the patients [27], we expected the R-Y reconstruction method to prevent any decline in the quality of life at six months after surgery. Previous retrospective studies using the EORTC QLQ-C30 and STO22 questionnaires also reported that the patients who underwent R-Y reconstruction showed better scores than those who underwent B-I or B-II reconstruction [28]. In contrast, we did not find any difference in any of the fields of the questionnaires between the groups, probably because our patients were well educated regarding food intake restrictions and adhered to the physician's instructions. Because previously mentioned retrospective study investigated the quality of life at a mean duration of 88 months after gastrectomy [28], the quality of life scores may have been different, according to the reconstruction methods and follow-up duration. We are planning to examine this aspect in the future for the same patients enrolled in this RCT.
In conclusion, the results of the present RCT showed that the R-Y reconstruction method using only staplers was favorable with respect to surgical outcomes. Therefore, this method can be considered an appropriate option for patients requiring distal subtotal gastrectomy for gastric cancer.
 XML Download
XML Download