

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Among patients with upper gastrointestinal (UGI) malignancies, about 5% suffer from acute UGI bleeding (UGIB) [12]. Primary gastric cancer is the most common UGI malignancy causing UGIB [12]. Recurrent tumor bleeding after initially successful hemostasis using endoscopic therapy occurs in 41%–80% of patients with inoperable gastric cancer [234]. Tumor bleeding is a distressing complication because it may delay a predetermined chemotherapy schedule, increase the need for transfusion, and be associated with poor survival [45].
Proton-pump inhibitors (PPIs) reduce gastric acid secretion by inhibiting H+ and K+-ATPase in the parietal cells of gastric mucosa, which stabilize blood clots [6]. Pre-endoscopic, intravenous use of a high-dose of the PPI omeprazole reduces the proportion of actively bleeding peptic ulcers and the need for endoscopic therapy [7]. The risk of re-bleeding after endoscopic therapy for peptic ulcer bleeding is also reduced by intravenous omeprazole [8]. Moreover, PPIs reduce recurrent bleeding and adverse ulcer effects in high-risk patients when used concomitantly with a cyclooxygenase-2 (COX-2) inhibitor [9] or regular use of low-dose aspirin [10]. Therefore, current guidelines recommend PPI therapy for management of non-variceal UGIB in patients, both before and after endoscopic therapy, and for the prevention of recurrent bleeding in high-risk patients [1112].
Although tumor bleeding frequently occurs in patients with inoperable gastric cancer, which may negatively affect their quality of life, effective methods for bleeding prevention have not been established. Therefore, we investigated the efficacy of oral lansoprazole treatment in preventing the occurrence of tumor bleeding in patients with inoperable gastric cancer.
MATERIALS AND METHODS
Study design and patients
This prospective, double-blind, randomized (1:1 allocation), placebo-controlled trial was conducted at 3 tertiary hospitals (National Cancer Center, Pusan National University Hospital, and Kosin University College of Medicine, Korea) from October 2009 until April 2014. The study protocol was approved by the Institutional Review Board (IRB) at the National Cancer Center (IRB No. NCCCTS09420), and by the IRBs of each participating institution. All patients provided written informed consent. This study was registered at ClinicalTrial.gov (identifier No. NCT02150447).
Eligible patients were ≥18 years of age with pathologically proven primary gastric adenocarcinoma. These patients had a treatment plan including first- or second-line palliative chemotherapy for inoperable, metastatic or locally advanced, unresectable gastric cancers. Patients were required to have an Eastern Cooperative Oncology Group (ECOG) performance status of 0 to 2 and adequate organ function. Patients with any of the following conditions were excluded: significant or uncontrolled gastrointestinal (GI) bleeding within 2 weeks before enrollment; any previous gastrectomy surgery; an inability to take oral medication; a history of allergy to PPIs; a serious concurrent infection or non-malignant disease; inadequate cardiovascular function, ischemic heart disease (unstable angina or myocardial infarction) within the past 6 months; a requirement for therapeutic anticoagulation, including aspirin or non-steroidal anti-inflammatory drugs; a requirement for therapeutic corticosteroids; and a need for PPI maintenance for uncontrolled reflux esophagitis or an active peptic ulcer. Data were collected, recorded, and managed using the clinical research coordination platform (eVelos system; Velos Inc., Fremont, CA, USA) and electronic case report forms.
Random assignment and intervention procedures
Eligible patients were randomly assigned in a 1:1 ratio to receive oral lansoprazole or placebo once per day. Random allocation numbers were generated interactively using the eVelos system at the National Cancer Center of Korea using permutated block randomization with block sizes of 2, 4, and 6. Stratification was based on the hemoglobin levels of the patients at the time of study enrollment (≥10 g/dL vs. <10 g/dL). Both patients and investigators were blinded to the intervention of the patient, and the randomization sequence was strictly concealed.
After assignment to intervention groups, patients started taking lansoprazole (30 mg) or placebo daily until a bleeding event occurred as defined in the next section. New study drugs were prescribed every 8 weeks (56 pills) after checking the numbers of pills taken by counting the returned pills. The use of study medication was stopped in patients that had a tumor bleeding event, were in poor general health, were transferred for supportive care, or were lost to follow-up.
Study assessment
Patients underwent a baseline history and physical examination, including blood analysis for complete blood cell counts, as well as liver and renal function testing. During the intervention period, the complete blood cell counts of patients were monitored to determine bleeding events every 3 weeks. A patient was determined to have a bleeding event if they presented with melena or hematemesis confirmed by attending medical personnel, if their hemoglobin level decreased more than 2.0 g/dL in 1 week with endoscopic evidence of tumor bleeding, or if their hemoglobin level decreased more than 3.0 g/dL in 3 weeks with endoscopic evidence of tumor bleeding. Endoscopic bleeding evidence upon endoscopic examination included Forrest Ia (spurting hemorrhage), Ib (oozing hemorrhage), IIa (non-bleeding exposed vessel), and IIb (adherent clots), which were defined according to the Forrest classification [13]. Endoscopic examinations were performed if patients had a defined bleeding event or suspected tumor bleeding.
Outcomes
In this study, the primary endpoint was a tumor bleeding event in the intention-to-treat population. Secondary endpoints included a transfusion requirement of packed red blood cells, and overall survival (OS). Patient survival status was obtained from the medical records of patients who had regular follow-up visits or from the claim database of the Korean National Health Insurance Corporation for those who were lost to follow-up.
Statistical analysis
The study sample size was determined on the assumption that the risk of tumor bleeding in inoperable gastric cancer patients who received palliative chemotherapy was 30%, which was based on internal data from the National Cancer Center of Korea. Considering a dropout rate of 15%, an enrollment of 394 patients was calculated to give the study a power of 90% to reduce the tumor bleeding rate to 15% (50% reduction) in the lansoprazole group with a 2-sided alpha level of 0.05. The enrolled patients were followed-up for 2 years, if the patient had no specific causes for discontinuation of the study.
A χ2 test or Fisher's exact test was used for categorical variables, and a Mann-Whitney U test for continuous variables. Gray's test was used to compare time-to-tumor bleeding events between the lansoprazole and placebo groups after randomization in the intention-to-treat population among patients who took at least one dose of the study medication. The medication had competing risks of death without tumor bleeding events [14]. The Kaplan-Meier method with the log-rank test was used to compare OS curves between both groups. In addition, the Fine-Gray regression model was used to calculate the effect of lansoprazole on tumor bleeding event as compared with that of placebo [15]. All statistical analyses were performed with STATA software (version 13.1; StataCorp., College Station, TX, USA) or SAS software (version 9.3; SAS Institute Inc., Cary, NC, USA). A P-value of <0.05 was considered statistically significant.
RESULTS
Patient baseline characteristics
Patient recruitment started in October 2009; however, this study stopped recruitment prematurely in April 2014 due to a low recruitment rate. During that period, 397 patients were assessed for eligibility. Of those, 130 patients were enrolled; 66 were allocated to the lansoprazole group, and 64, to the placebo group. The enrolled patients were followed up until April 2015. Of those, 3 patients did not receive the allocated treatment; thus, 127 patients were included in the final analyses: 64 in the lansoprazole group and 63 in the placebo group. The detailed study flowchart is illustrated in Fig. 1.
 | Fig. 1CONSORT diagram of this study.
CONSORT = Consolidated Standards of Reporting Trials; ECOG = Eastern Cooperative Oncology Group; PPI = proton pump inhibitor.
|
The baseline characteristics were not significantly different between the lansoprazole and placebo groups (Table 1). Of the total enrolled patients, the median age was 56 years, 78.7% were male, and 20.5% had a baseline hemoglobin level <10.0 g/dL. On the endoscopic examination, proportion of tumors with ulcer findings (ulcerofungating and ulceroinfiltrative mass) was 81.9%. Most of the enrolled patients (98.4%) had metastatic disease. The proportion of patients who had received a concurrent 1st line chemotherapy was not different between the lansoprazole group and the placebo group (84.4% vs. 69.8%; P=0.059). The mean duration of medication administration was longer in the lansoprazole group than in the placebo group (204 vs. 158 days; P=0.252); however, there were no serious adverse events related to the study medication.
Table 1
Baseline clinical characteristics of the 127 enrolled patients
Values are presented as median (IQR), number (%), or mean±SD.
BP = blood pressure; ECOG = Eastern Cooperative Oncology Group; IQR = interquartile range; SD = standard deviation.
*Differentiated type denotes papillary-, well-, or moderately-differentiated adenocarcinoma, and undifferentiated type denotes poorly differentiated adenocarcinoma or signet ring cell carcinoma.
![]()
Primary outcome evaluation: tumor bleeding event
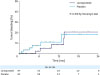
During the median follow-up time of 6.4 months (interquartile range, 3.1–12.8 months), the primary outcome (tumor bleeding event) occurred in 5 patients (7.8%) in the lansoprazole group and in 6 patients (9.5%) in the placebo group (Table 2). The hazard ratio [HR] in the lansoprazole group was 0.67 and 95% confidence interval [CI] was 0.21 to 2.11 (Table 3). There was no significant difference in the tumor bleeding events between the lansoprazole and placebo groups (P=0.515 by Gray's test; Fig. 2). However, when the follow-up period was censored at 4 months, the cumulative incidence rate of tumor bleeding in the lansoprazole group (0%) was lower than that in the placebo group (8.0%) (P=0.041 by Gray's test). Of the 4 patients in the placebo group who had tumor bleeding during initial 4 months follow-up periods, 2 patients received a 1st line chemotherapy and the remaining 2 patients had 2nd line chemotherapy. There were no deaths related to tumor bleeding among the patients who had a bleeding event.
Table 2
Outcomes of the 127 enrolled patients

![]()
Table 3
Risk factors associated with tumor bleeding
cHR = crude hazard ratio; CI = confidence interval; ECOG = Eastern Cooperative Oncology Group; NA = not applicable.
*Fine-Gray regression model; †cHR could not be estimated because no bleeding events occurred in patients with tumor sizes of less than 5 cm; ‡Differentiated type denotes papillary-, well-, or moderately-differentiated adenocarcinoma, and undifferentiated type denotes poorly differentiated adenocarcinoma or signet ring cell carcinoma.
![]()
Secondary outcome evaluation: transfusion requirement and OS
During the follow-up period, the proportions of patients who received a transfusion, as well as those who received a transfusion of more than 5 units, were not significantly different between the 2 groups. Seven patients (10.9%) in the lansoprazole group and 9 (14.3%) in the placebo group underwent urgent endoscopy for suspicion of tumor bleeding due to an abrupt decrease in hemoglobin levels (P=0.570; Table 2). However, the events in these patients did not meet the definition of a tumor bleeding event because endoscopic findings did not show evidence of bleeding. During the follow-up period, there were no patients who underwent palliative surgery due to tumor bleeding.
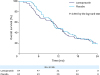
The median OS after randomization was 11.7 months in the lansoprazole group and 11.2 months in the placebo group, with the OS times not being statistically different between the groups (P=0.610 by log-rank test; Fig. 3).
DISCUSSION
In this trial, the use of lansoprazole, as compared with placebo, did not reduce tumor bleeding in patients with inoperable advanced gastric cancer. Furthermore, transfusion requirements and OS times were not different between the lansoprazole- and placebo-treated patients. However, lansoprazole-treated patients did not have any tumor bleeding events during the first 4 months after randomization, whereas 4 placebo-treated patients had bleeding events during the same period.
The effects of PPI therapy for bleeding have been largely investigated in patients with peptic ulcers. A meta-analysis of 21 randomized controlled trials showed that PPI treatment significantly reduces the risk of re-bleeding and the need for surgery in patients with peptic ulcer bleeding [16]. Furthermore, PPIs reduce ulcer bleeding and associated adverse effects in high-risk patients who use low-dose aspirin, nonsteroidal anti-inflammatory drugs, or COX-2 inhibitors [91017]. Although inoperable advanced gastric cancer patients have a high risk of tumor bleeding [18], there have been no well-designed studies to investigate whether PPI therapy can reduce tumor bleeding. This is the first clinical study to evaluate the effect of PPI treatment on the prevention of gastric cancer bleeding, no definite beneficial effects discovered.
PPI therapy maintains intra-gastric pH ≥6.0 [19], which is an adequate pH level for clot formation and stabilization [20]. In addition, PPI therapy can heal the ulcer itself, and as a consequence, it may be associated with the reduction of bleeding-associated adverse effects in patients with peptic ulcers. These ulcer healing effects were also reported in malignant gastric ulcer patients [2122]. In this trial, inoperable gastric cancer patients who received lansoprazole had significantly reduced tumor bleeding events compared with those who received placebo until 4 months after the initiation of drug administration; however, the differences between the 2 groups became insignificant after the first 4 months of treatment. One possible explanation might be the increased tumor burden due to cancer progression that occurred during palliative chemotherapy.
In the present trial, lansoprazole therapy did not reduce the requirement for transfusion in inoperable gastric cancer patients. In patients with GI-tract cancers, tumor bleeding occurs with chronic symptoms presenting as dark stool or positive occult blood in stool, rather than presenting with massive UGIB [23]. Moreover, chronic blood loss from the tumor, even without sudden bleeding episodes, can cause chronic anemia, including iron deficiency anemia, in patients with GI-tract cancers [24]. The mucosa of gastric cancer is vulnerable to spontaneous bleeding, and oozing hemorrhage is the most common type of endoscopic bleeding stigmata [18]. Thus, tumor bleeding is not a rare complication in patients with inoperable gastric cancer, and transfusion and diagnostic evaluation is frequently required. In this trial, more than 60% of the enrolled patients had large tumors (>5 cm), and as a result, there was a greater extent of mucosa prone to bleeding. We speculate that oral lansoprazole therapy is not as effective in reducing chronic, low-level blood loss from friable tumor mucosa.
Once a tumor bleeding event occurs, treatment becomes more complicated. Moreover, the re-bleeding rate after successful endoscopic hemostasis has been reported to be as high as 41% [4]. Tumor bleeding may cause a delay in the predetermined chemotherapy schedule or increase the risk of bleeding-related death. In addition, patients whose endoscopic hemostasis fails show shorter than expected OS [45]. Therefore, in our study, we evaluated the effect of daily oral PPI treatment on overall mortality of inoperable gastric cancer patients as a secondary outcome. However, daily lansoprazole therapy, as compared with placebo treatment, did not affect OS in our trial. This result may be due to the low bleeding rate and the lack of bleeding-related mortality occurrences in our study.
In the present trial, the placebo group had less tumor bleeding events than would be expected based on the sample size. There are several possible reasons for this discrepancy. First, the palliative chemotherapy may have improved the tumor status of the enrolled patients. Since the 1990s, clinical trials have shown that palliative chemotherapy with various regimens significantly increases tumor response and improves OS [25]. For instance, a recent phase III clinical trial using specific molecular targeting agents reported tumor response rates between 35% and 47% [2627]. Second, gastric cancer is increasingly diagnosed at earlier stages owing to the national cancer screening program that provides biennial endoscopic screening in Korea. Following initiation of this program, screening rates for gastric cancer have increased annually from 52% in 2004 to 80% in 2013 [28], and the proportion of early-stage gastric cancer has increased in patients who underwent a screening endoscopy between 2006 and 2011 [29]. We speculate that even the patients with stage IV cancer are being diagnosed at smaller sizes or with less prominent ulcers, both of which would lead to fewer bleeding events.
This trial is the first well-designed, randomized controlled trial assessing the effect of PPI therapy on a population of gastric cancer patients, but there are several important limitations. First, we could not complete the study of the initial 394 recruited patients, as the study was prematurely stopped. This is a consequence of the national cancer screening program, as the proportion of stage IV gastric cancers have been decreasing in Korea, resulting in insufficient study enrollment [30]. Therefore, the study power for the primary outcome is not enough to conclude that daily oral lansoprazole does not reduce the tumor bleeding incidence in patients with inoperable gastric cancer. Second, we only investigated the effect of a once-a-day dose of oral lansoprazole. For patients with inoperable gastric cancer, a higher dosing schedule may be more effective; thus, further studies will be needed to assess the effect of lansoprazole at varying doses. Third, the median follow-up duration was short, and the number of patients who were lost to follow-up was large. Despite the survival benefits associated with first- and second-line chemotherapy, a standard third-line regimen has not yet been investigated for progressed gastric cancer [31]. This may be the cause of the shorter follow-up duration and the increasing number of patients lost to follow-up in the current study. Finally, the placebo group included more patients who received 2nd line chemotherapy than the lansoprazole group, despite no statistical significance. Thus, this may affect tumor bleeding events during early periods in the placebo group, partly because of poor tumor control by the 2nd line chemotherapy.
In conclusion, this study found that maintaining daily oral lansoprazole in inoperable advanced gastric cancer patients did not significantly reduce the incidence of tumor bleeding. However, during the initial 4-month period of lansoprazole therapy, tumor bleeding events were significantly reduced compared with those in placebo-treated patients. Therefore, further studies are needed to evaluate whether PPIs can prevent tumor bleeding during the early phase of chemotherapy for inoperable gastric cancer.
 XML Download
XML Download