

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Tuberculosis (TB) remains a major global health concern, with an estimated 9.6 million new cases and 1.2 million deaths in 2014 (1). Emerging drug resistance makes the control of TB especially difficult. Currently, one-quarter of estimated multi-drug resistant tuberculosis (MDR-TB) patients are detected, and only a half of them are successfully treated whereas 63% of drug-sensitive TB are detected and 85% of them are successfully treated (1). In Korea, approximately 1,000 patients with newly diagnosed MDR-TB have been reported annually (2).
The transmission of the drug-resistant TB strain is primarily responsible for MDR-TB cases (3). Close contacts with MDR-TB patients are persons at high risk for latent TB infection (LTBI) and active MDR-TB. Contact investigation in households of MDR-TB patients showed 47.2% of LTBI and 7.8% of secondary active TB (4). Secondary active TB appeared within 1 year of diagnosis of index MDR-TB in over half of patients, and had multi-drug resistance concordant with index MDR-TB in up to 90% (5).
LTBI treatment is important for contact with drug-sensitive TB in preventing the development of secondary active TB. Nevertheless, there is no established effective treatment for contact with LTBI to MDR-TB (6), with frequent side effects and at least a 6-month period of treatment, which cause treatment discontinuation in 58%–100% of contacts (7). Management of contacts with MDR-TB largely depends on close observation (8). Thus, early identification of secondary active MDR-TB in contacts is crucial (35). However, close observation with chest radiographic and symptom screening may be ineffective in detecting secondary MDR-TB at an early stage, due to lack of symptoms, scarcity of sputum (9), and vagueness of chest radiograph (10). Immunologic studies including tuberculin skin test and interferon gamma release assay (IGRA) had limitations in predicting the development of active TB from LTBI (11). Contacts are known to have low adherence to LTBI management, and are at risk of being lost to follow-up (12).
Several new biomarkers have been suggested for predicting progression from LTBI to active TB, but are not yet applicable and take time for clinical implementation (11). Computed tomography (CT) is one of the most widely used imaging modalities, offering high-resolution anatomic evaluation, though radiation is of concern (13). We preliminarily introduced submillisievert chest CT scans to investigate early identification of active secondary MDR-TB in close contacts.
Materials and Methods
Contact investigation
The index patient was a 35-year-old man with a 3-month history of a productive cough and a poorly controlled diabetes. The acid-fast bacilli (AFB) smear of his sputum was positive with a 3+ grade. The Xpert/RIF assay was positive for Mycobacterium tuberculosis and rifampicin resistance, followed by culture positivity. The drug susceptibility test confirmed resistances to isoniazid (Carolina Medical Products Co., Farmville, NC, USA), rifampin (sanofi-aventis U.S. LLC, Bridgewater, NJ, USA), and rifabutin (Pfizer Inc., New York, NY, USA).
Investigation of the present study was initiated for eligible close contacts as follows: individuals older than 20 years old, with household contact or working in the same room for more than 8 hours per day (ClinicalTrials.gov Identifier: NCT02454738). Close contacts underwent baseline, 3-month, 1-year follow-up submillisievert chest CT scans, along with conventional contact investigation. For full technical details of contact investigation, bacteriology and genotyping, see the Supplementary 1.
Submillisievert chest CT scanning
Unenhanced chest CT scans were obtained using a 64-channel multidetector CT scanner (Discovery CT750 HD; GE Healthcare, Waukesha, WI, USA) at a peak kilo-voltage of 120 kV and a tube current of 5 mAs. Patients were scanned craniocaudally from the lung apex to the costophrenic angle in the supine position at full inspiration during a single breath-hold. CT parameters were collimation of 0.625 mm × 64, a pitch of 0.984, and a gantry rotation time of 0.5 seconds, with images reconstructed by model-based iterative reconstruction (Veo; GE Healthcare), and 1.25-mm slice thickness in the transverse plane and 2.5-mm slice thickness in the coronal plane. Effective doses of chest CT scans were estimated by multiplying dose-length product by a chest-conversion factor of 0.0145 (14).
Results
Baseline contact investigation and CT scanning
Seven close contacts who worked with the index patient were identified. There was no family living together. One contact was reluctant to contact investigation and study enrollment, so contact investigation was performed in six contacts (contact 1 to 6) (mean age, 35 years; age range, 30–37; male:female, 5:1) (Table 1). All six contacts denied any symptoms or signs, and had normal chest radiographic findings on baseline examination. Half of six contacts (contact 1, 3, and 6) turned out to have LTBI.
Table 1
Summary of contact investigation in close contacts to MDR-TB

The Korean national guideline for contact investigation for TB adopts a two-step strategy for LTBI, sequentially performing tuberculin skin test and IGRA.
MDR-TB = multi-drug resistant tuberculosis, TB = tuberculosis, IGRA = interferon gamma release assay, LTBI = latent tuberculosis infection.
*LTBI was assessed to be present when both tuberculin skin test and IGRA were positive. Cutoffs for positivity of tuberculin skin test and IGRA (corrected for Nil response) were 10 mm and 0.35 IU/mL, respectively. †Contact 2 did not have a positive conversion in the secondary tuberculin skin test which was performed 3 months later. ‡Contact 6 had a history of positive tuberculin skin test before, so tuberculin test was omitted.
![]()
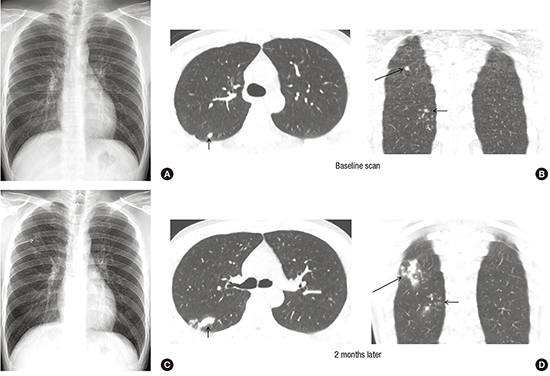
Baseline CT scans identified incidental parenchymal abnormalities in two of six contacts. In contact 1, a few ill-defined nodules and branching opacities were localized in the superior segment of the right lower lobe (Fig. 1). In contact 2, two sub-centimeter nodules were found in the apical segment of the right upper lobe (Fig. 2).
 | Fig. 1Chest radiograph and CT of a secondary case of MDR-TB in contact 1. (A) Chest radiograph at baseline contact investigation is normal. (B) Baseline submillisievert computed tomographic scans of the chest shows tuberculous granuloma and focal bronchiolitis (arrows) in the superior segment of the right lower lobe on baseline scan. (C) Chest radiograph 2 months later shows subtle opacities (arrow) in the right upper lung zone. (D) Submillisievert computed tomographic scans of the chest 2 months later shows the progression of pre-existing lesions into ill-defined lobular consolidation (arrows) in the superior segment of the right lower lobe. (E) Results of spoligotyping 24-loci MIRU-VNTR analysis are identical between index and secondary MDR-TB. (F) Chest radiograph taken after completion of 1.5-year of anti-MDR-TB treatment shows small residual opacity (arrows) in the right upper lung zone.
CT = computed tomography, MDR-TB = multi-drug resistant tuberculosis, MIRU-VNTR = mycobacterial interspersed repetitive units-variable-number tandem repeats, TB = tuberculosis.
|
 | Fig. 2Chest radiograph and CT in contact 2, having sub-centimeter-sized nodules. (A) Chest radiograph at baseline contact investigation is normal. (B) Baseline, 3-month, and 1-year follow-up submillisievert computed tomographic scans of the chest shows two suspected tuberculous granulomas (arrows). Lesions increased slightly 3 months later, and decreased after 1 year of observation.
CT = computed tomography.
|
Follow-up contact investigation and CT scanning
Due to concern about branching opacities and nodules for baseline CT scan in contact 1, follow-up was advanced by one month. Contact 1 denied any symptoms or signs at a 2-month follow-up. Sputum AFB smear, Xpert/RIF test, and mycobacterial culture were negative. CT scan depicted increase of pre-existing nodular and branching opacities in the same lobe, while chest radiograph showed subtle opacities in the right upper lung zone (Fig. 1). The pulmonologist decided to perform a bronchoalveolar lavage. Pre-procedural chest radiograph for bronchoscopy was taken 3 weeks later, showing overt progression of radiologic abnormalities. The bronchoalveolar lavage fluid was positive for M. tuberculosis and rifampin resistance on same-day Xpert/RIF test, leading to immediate isolation. The mycobacterial culture of bronchoalveolar lavage fluid was positive after 13 days in liquid media and 8 weeks in solid media. The result of the drug susceptibility test in contact 1 was identical with that of the index case. The pattern of spoligotyping and 24-loci mycobacterial interspersed repetitive units–variable-number tandem repeats (MIRU-VNTR) between index patient and contact 1 was matched identically (M. tuberculosis strain, Beijing; 24-loci MIRU-VNTR, 244233352544425173353824). Contact 1 was treated with kanamycin, pyrazinamide, moxifloxacin, prothionamide, and cycloserine. During the treatment, serial expectorated sputa were negative for smear and culture. He was cured after 1.5-year of treatment.
Other contacts did not have symptoms at 3-month and 1-year follow-up. In contact 2, a 3-month follow-up CT scan showed a slight increase in nodule size. One of two nodules decreased on follow-up CT scan 1 year later (Fig. 2). There were no abnormalities in follow-up CT scans in four of six contacts, and none with negative initial LTBI test had a positive conversion in the secondary LTBI test.
Radiation dose of submillisievert chest CT scanning
Median dose-length product and effective dose per CT scan were 14.91 milligray-cm (range, 13.08–16.90) and 0.21 millisievert (range, 0.19–0.25), respectively, with 1-year cumulative dose-length product of 44.52 milligray-cm (range, 43.28–49.18) and 1-year cumulative effective dose of 0.65 millisievert (range, 0.63–0.71).
Discussion
Radiation exposure ought to be the main concern for the use of chest CT scans in contact investigation of TB (13). Low dose ionizing radiation of medical imaging below 100 millisievert may increase cancer risk in children, who are more radiosensitive than adults (15). However, the estimated effective dose of our submillisievert chest CT scans (average, 0.21 millisievert; range, 0.19–0.25) is much lower than that of conventional chest CT scans (average, 7.0 millisievert; range, 4.0–18.0), two times higher than posteroanterior and lateral chest examinations (average, 0.10 millisievert; range, 0.05–0.24), and ten times higher than posteroanterior chest radiographs (average, 0.02 millisievert; range, 0.01–0.05) (16). Submillisievert radiation is negligible for cancer risk when compared with radiation from natural source of 3.1 millisievert per year in adults.
TB granuloma is the earliest pulmonary parenchymal abnormality (17). Baseline CT scan depicted sub-centimeter-sized nodules suspected of TB granuloma in contact 1 and 2, which were not shown on chest radiograph. However, the presence of parenchymal CT abnormalities in contacts are not indicative of active disease without overt CT findings of active TB, such as extensive tree-in-bud appearance and cavities (18). The hallmark of active TB is the progression of parenchymal abnormalities on follow-up. Thus, we introduced repeated submillisievert CT scans for determining active disease. Indeed, repeated CT examinations revealed that TB granuloma gradually progressed in contact 1, while sub-centimeter-sized nodules was stabilized in contact 2, potentially in line with the inter-individual and within-host variability of TB (17).
Based on the radiologic progression of repeated submillisievert CT scans, contact 1 was further evaluated and diagnosed with secondary MDR-TB in asymptomatic periods. This led to a favorable treatment outcome with minimal residue, and early isolation of MDR-TB at the lowest infectivity, consequently minimizing transmission of drug-resistant strain. In a risk-benefit perspective, submillisievert chest CT may be considered in adult contacts at risk for MDR-TB in high-resource setting, such as health care workers (19). Given that active TB most commonly develops in the first 2 years of TB exposure, annual follow-up chest CT may be performed up to the first 2 years. In addition, submillisievert chest CT may not be recommended in contacts with negative LTBI but it needs to be considered that false-negative rate of LTBI test is 8%–19% and increased in immunocompromised contacts (20). Further investigation is required for these issues.
In conclusion, early identification of secondary MDR-TB is feasible with submillisievert chest CT scans in contact investigations of MDR-TB, minimizing of MDR-TB transmission and offering a favorable treatment outcome.
 XML Download
XML Download