

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Sjögren’s syndrome (SS) is a systemic autoimmune disease involving the lacrimal and salivary glands with resultant keratoconjunctivitis sicca and xerostomia, and lymphocytic infiltration of exocrine glands and epithelium is a common pathological finding (1). SS is one of the most prevalent rheumatologic diseases and has female predominance (2). Approximately one-third of SS patients have extraglandular systemic involvement, and SS patients with or without other autoimmune rheumatic disease are defined as having secondary SS (sSS) or primary SS (pSS), respectively. In 2002, the American–European Consensus Group defined the rules for classifying pSS and sSS mainly using a serologic marker (the anti-Ro/La antibody level) and the histopathology of the salivary glands (3).
Conjunctival and corneal staining tests, the Schirmer test, and symptoms are worse in patients with than without SS among aqueous-deficient dry eye patients (4). Conjunctivocorneal epithelial disintegration results in blurred vision, severe discomfort, and increased risk of infection. Therefore, severe dry eye in SS patients results in an ongoing poor quality of life.
The first treatment option for dry eye symptoms is topical drugs such as artificial tears or cyclosporine A (25). However, topical treatment is not usually sufficient for severe dry eye in pSS patients. Because inflammatory markers are increased in SS patients, most systemic medications are aimed at immunologic pathways (6). Antimalarial drugs are frequently prescribed to SS patients as non-specific blockers of toll-like receptor 9/7 (TLR9/TLR7), but their effectiveness in dry eye is controversial. Improvement in levels of immunologic markers such as IL-6, the erythrocyte sedimentation rate (ESR), C reactive protein (CRP), and B-cell activating factor (BAFF), in addition to sicca signs such as the tear break-up test (TBUT) and Schirmer test, has been reported in a few studies after oral management with hydroxychloroquine (HCQ) (78). However, only two double-blind randomized trials for pSS have been performed so far, which demonstrated that HCQ treatment does not have clinical benefits for pSS patients (910).
Therefore, to evaluate the effect of oral HCQ treatment in dry eye in pSS, we conducted a prospective randomized, double-blind trial comparing the HCQ treatment with a placebo control.
MATERIALS AND METHODS
Patients
This randomized controlled trial was conducted at the Department of Ophthalmology at Seoul National University Hospital from May 2011 through August 2013. Inclusion criteria were 1) adult (aged > 18 years) patients with pSS diagnosed on the basis of the 2002 American–European Consensus Group (AECG) criteria (3) and 2) subjects who had the ability to give informed, dated, and signed consent before the beginning of any proceedings related to the trial.
Exclusion criteria were 1) previous treatment with HCQ with insufficient discontinuation time (3 weeks) after discontinuation of treatment; 2) known cardiac disease, respiratory disease, renal disease, or gastrointestinal disease (except gastrooesophageal reflux disease); 3) diabetes mellitus; 4) psoriasis; 5) known drug allergy or hypersensitivity; 6) previous or ongoing treatment with any other drugs (including topical drugs) that may affect the lacrimal system with insufficient washout time after discontinuance of treatment (e.g., SSRI, anti-histamines, and pilocarpine); 7) closed-angle glaucoma; 8) previous intraocular surgery; 9) macular disease; 10) previous or ongoing treatment with drugs that may have an effect on the macula; 11) pregnancy; and 12) planning pregnancy.
A double-blind, randomized control study was conducted in 39 subjects of 153 pSS subjects for 2 years. We were unable to recruit the intended 60 subjects within the 2-year recruitment period because many subjects with pSS did not meet our inclusion criteria. Most of the subjects did not wish to discontinue previous oral drugs because of severe systemic symptoms. During the study period, 153 pSS patients visited our clinic. Among them, only 67 subjects met all eligibility criteria. Twenty-eight subjects declined to participate in the trial, and 39 subjects were finally enrolled in this study (Fig. 1).
 | Fig. 1A double-blind randomized control study was conducted in 39 subjects of 153 pSS subjects who visited an eye clinic from May 2011 through August 2013.
|
During the study period of 2 years, a new criterion for SS was reported (11). Because this study was designed before the recent criterion was published, we enrolled subjects according to the previous criteria of the American–European Consensus Group to maintain consistency of the subject population.
Treatment protocol
All subjects underwent initial medical and ophthalmologic history taking and physical examination at the baseline visit (week 0). The study eye was selected as the eye that showed the higher corneal fluorescein staining score (on a scale of 0–15; National Eye Institute scale [12]) at the baseline visit. Subjects were randomly assigned to the HCQ or placebo group by using sealed randomization envelopes. The placebo was manufactured to be identical in appearance to the active drug, and all tablets were kindly supplied by Kyung Poong Pharma Co. Both the investigators and subjects were blinded to the treatment assignments. The subjects were instructed to take two tablets (one 200 mg tablet and one 100 mg tablet) of the study medication, giving a total of 300 mg, once daily (qd) for 12 weeks and to report missed doses and adverse events. All subjects used Hyalein Mini ophthalmic solution 0.1% (0.1% hyaluronic acid; Santen, Osaka, Japan) six times per day. Other topical medications were restricted. Participants returned to the study site at 6 and 12 weeks for efficacy and safety evaluations. After 12 weeks, oral HCQ and placebo medication were withheld, whereas topical medication was continued in all subjects for 4 weeks. The subjects revisited the clinic at 16 weeks. At each visit, the visual acuity, corneal fluorescein staining score using NEI grading, Schirmer test score without anesthesia, tear film break-up time (TBUT), Hardy Rand and Rittler (HRR) color vision test, and fundus examination were performed. Schirmer test was done with a Schirmer strips (Eagle Vision, Memphis, TN, USA) for five minutes without topical anesthesia. TBUT was measured after instillation of one drop of 0.25% fluorescein dye into the conjunctival sac, and the subjects were asked to blink several times. Subjective assessment was performed using the ocular surface disease index questionnaire (OSDI) (13). The OSDI questionnaire was translated to Korean from the original English. Tear and blood samples were collected for measurement of IL-6, BAFF, ESR, and IL-17 levels in addition to Th17 cells that secrete IL-17.
Tear sample collection
Tear fluid was obtained from the patients at the same time at baseline and at 6, 12, and 16 weeks. Tears were collected from the medial and lateral canthus. Topical anesthesia was not used. To minimize ocular surface irritation, we obtained tear samples by using a Merocel sponge (PVA 0525; Oasis, Glendora, CA, USA) (14). After collection, the sponge was inserted into a 0.5-mL tube (Eppendorf, Fremont, CA, USA) and the tear fluid was subsequently recovered by centrifugation at 10,000 rpm for 10 minutes.
Measurement of tear and serum cytokine profiles
ESR was measured by conventional methods in our hospital laboratory on the day of the patient visit. For BAFF and IL-6, 0.5 mL of plasma was separated from heparinized peripheral blood and stored together with the tear sample at -70°C until further examination.
The concentrations of BAFF, IL-6, and IL-17A were measured using a commercially available enzyme-linked immunosorbent assay (ELISA) kit (R&D Systems, Minneapolis, MN, USA) according to the manufacturer’s instructions. ELISA using serum was performed in duplicate to ensure the reproducibility of the data. However, ELISA using tears was performed only once because of the lack of a sufficient amount of tears. Tear samples were diluted 1:12.5 and 1:100 for BAFF and IL-17, respectively.
The concentration ranges used for the standard curve were 62.5–4,000 pg/mL, 9.38–600 pg/mL, and 15.6–1,000 pg/mL of human recombinant BAFF, IL-6, and IL-17, respectively (R&D Systems).
Flow cytometric analysis for Th17 cells
Flow cytometry was also performed on the same day as the patient visit. Peripheral blood mononuclear cells (PBMCs) were isolated from whole blood by density gradient centrifugation (BIOCHROM Inc., Cambridge, UK). PBMCs were stimulated for 6 hours with 50 ng/mL 1-phorbol-12-myristate-13-acetate (PMA; Sigma-Aldrich, St Louis, MO, USA) and 1 μg/mL ionomycin (Sigma-Aldrich) in the presence of brefeldin A (BD Bioscience, San Jose, CA, USA) for the final 4 hours. The cells were fixed and permeabilized using a BD Cytofix/Cytoperm kit (BD Bioscience). The fixed cells were stained with anti-CD3-APC-Cy7 and anti-CD4-FITC for 30 minutes at 4°C for initial surface staining. For intracellular staining, the cells were incubated with anti-IFN-γ-PE-Cy7 (all from BD Bioscience) and anti-IL-17A-PE (eBioscience, SanDiego, CA, USA) mAb for 60 minutes at 4°C. Flow cytometric analysis was performed using a FACS BD LSR II (BD Bioscience), and the data were analyzed by FlowJo (Treestar, Ashland, OR, USA). Isotype mouse Ig G1-PE-Cy7 (eBioscience) and mouse Ig G1- PE (eBioscience) were used as controls.
After four-color compensation, lymphocytes were gated in the forward scatter (FSC)/side scatter (SSC) gate, and CD4 T cells were then gated by CD3hi and CD4hi expression; finally, the cells were gated by IFNγ and IL17 expression (Fig. 2). The percentage of Th17 cells was calculated by summing the amounts of IL17hi cells and IFNγ/IL17 double hi cells.

Sample size calculations
A previous literature review on SS did not include results for the tear IL-17 concentration after HCQ medication. The tear IL-17 concentration of SS patients was 504.91 pg/mL and 352.45 pg/mL in the total and mild keratoconjunctivitis sicca groups, respectively, in this previous report (15). We assumed that the tear IL-17 concentration after HCQ medication would be similar to that of the mild keratoconjunctivitis sicca group from the previous study. A sample size of 60 patients (30 in each group) was needed to detect a significant difference between 504.91 ± 136.38 pg/mL and 352.45 ± 136.38 pg/mL in the 2 groups using a 2-sided test with a power of 80% and the significance level controlled at 5%. The Medical Research Collaborating Center of Seoul National University Hospital assisted in the sample size calculation.
Statistical analysis
Primary analyses of the data were based on the per-protocol population, which included all participants who took the 12-week course of study medication. Statistical analyses were performed using PASW software for Windows (v. 19.0; SPSS Inc., Chicago, IL, USA). P < 0.05 was considered statistically significant. The Shapiro–Wilk test was applied to evaluate data normality. The two groups were compared with Student’s t-test (two-tailed) of the Mann–Whitney U test depending on normality. To compare changes within groups at different time intervals, a paired sample t-test and Wilcoxon signed-rank test were used depending on normality. Differences between the HCQ and placebo groups during the course of the treatment were analyzed by repeated-measures ANOVA and linear mixed models when data were missing.
Ethics statement
Written informed consent was obtained from all subjects, and the study was granted ethical approval by the institutional review board of Seoul National University Hospital (IRB number: H-1104-083-359). This study was conducted in accordance with the tenets of the Declaration of Helsinki. This study was registered with ClinicalTrials.gov (Identifier: NCT01601028).
RESULTS
General complications of the subjects and characteristics of drop-out subjects
Of the 39 recruited subjects, 26 were treated per protocol. Thirteen subjects including five in the placebo group and nine in the HCQ group did not complete the study. The initial age, ESR, TBUT, Schirmer score, corneal staining score, and OSDI were not significantly different between complete and incomplete groups. In the placebo group, three subjects did not keep their follow-up appointments and were unavailable to be reached, one subject suffered dyspepsia, and one subject was found to be unsatisfactory for enrolment. In the HCQ group, two subjects did not keep their follow-up appointments and were unable to be contacted, three subjects suffered dyspepsia, one subject did not have the time for follow-up examinations, two subjects were found deficient with regard to the enrollment criteria, and one subject developed incidental subretinal hemorrhage because of occult myopic choroidal neovascularisation (CNV) with accompanying impaired vision 3 days after medication, which was not regarded as a drug-related complication. There were no other drug-related side effects with regard to ocular complications (optic neuropathy or maculopathy) or general subjective complications except dyspepsia (10.3%).
Characteristics of the study population at baseline
Of the 26 pSS subjects analyzed, 11 subjects were randomly assigned to receive HCQ and the remaining 15 subjects were randomly assigned to receive the placebo. All subjects were women with a mean age of 56.85 years (range, 35–74). The mean (range) age was 55.0 (35–73) years in the placebo group and 59.4 (44–74) years in the HCQ group, which was not significantly different (P = 0.263, independent t-test). The initial results for ESR, serum IL-6, BAFF, Th17, tear BAFF, TBUT, Schirmer score, corneal staining score, and OSDI are shown in Table 1. There were no significant differences between the groups for all of the demographic factors and parameters.
Table 1
Demographics and initial characteristics of the subjects
HCQ, hydroxychloroquine; ESR, erythrocyte sedimentation rate; IL, interleukin; Th17, T helper 17 cells; BAFF, B-cell activating factor; TBUT, tear film break-up time; OSDI, ocular surface disease index.
*Independent t test; †Mann–Whitney U test.
![]()
Changes in parameters
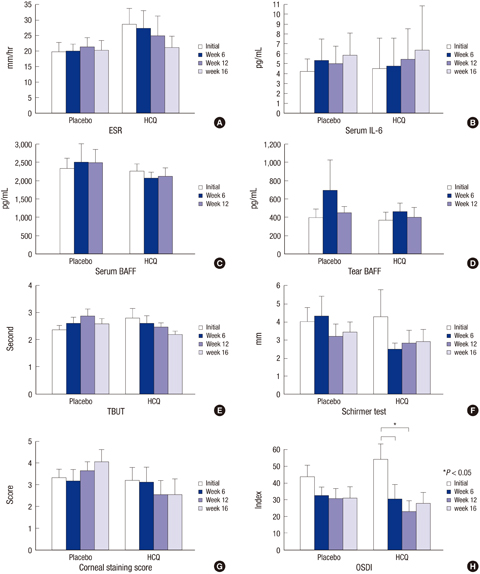
Changes in parameters are shown in Table 2 and Figs. 2 and 3. Regarding systemic inflammatory parameters, the mean ESR tended to continuously increase in the placebo group and decrease in the HCQ group, although there were no significant differences between the groups. The mean serum IL-6, BAFF, proportion of Th17 cells, and tear BAFF were not significantly different between the groups. Tear IL-17 was not detected in almost of all the samples.
Table 2
Changes of the parameters between the HCQ and placebo groups during follow-up

HCQ, hydroxychloroquine; ESR, erythrocyte sedimentation rate; IL, interleukin; Th17, T helper 17 cells; BAFF, B-cell activating factor; NA, not available; TBUT, tear film break-up time; OSDI, ocular surface disease index.
*Repeated-measures ANOVA; †Linear mixed model.
![]()
 | Fig. 3Changes of ocular and systemic parameters in the hydroxychloroquine (HCQ) and placebo groups during follow-up. ESR (A) and serum IL-6 (B) levels, serum (C) and tear (D) BAFF levels, tear break-up time (TBUT) (E), Shirmer test score (F), corneal staining score (G), and ocular surface disease index questionnaire (OSDI) (H) are shown. Bars represent the mean + standard error.
|
With respect to the ocular signs and symptoms, TBUT did not change significantly from the baseline to week 12 in either group. The Schirmer test score did not significantly change in either group. The HCQ group tended to show continuous reduction of the corneal staining score, although the reduction was not significant. OSDI was significantly decreased between the baseline and weeks 6 and 12 only in the HCQ group (P < 0.05, baseline vs. 6 weeks; P < 0.01, baseline vs. 12 weeks; paired t-test; Fig. 3H), suggesting improvement of subjective symptoms. However, the HCQ and placebo groups were not significantly different (P = 0.209, repeated-measures ANOVA).
After discontinuation of the oral medication, only the proportion of Th17 cells was significantly increased in both groups (P < 0.01, repeated-measures ANOVA). However, there was no difference between the groups (P = 0.566). Other parameters did not show significant changes after the oral medications were discontinued (Table 2, Fig. 2).
DISCUSSION
No definite beneficial effect of the use of HCQ in the treatment of dry eye in pSS was found in this study, although there was evidence of improved subjective ocular symptoms. The study did not support an effect of HCQ treatment on tear production and inflammatory parameters such as ESR, IL-6, BAFF, and Th17 cell levels in pSS patients.
The main anti-inflammatory mechanism of HCQ is considered to be non-specific antagonism at TLR9 and TLR7 (1617). Circulating DNA- and RNA-containing immune complexes in the blood may stimulate plasmacytoid dendritic cells (pDCs) through TLR9 and TLR7 (1718). Activated pDCs produce IL-6, which can induce co-stimulatory molecules, and the stimulated co-stimulatory molecules combine with T cell receptor activate T helper (Th) cells (1920). A recent study revealed that the number of Th17 cells is increased and that these cells are involved in the main pathogenic pathways in RA, SS, SLE, and GVHD (2122), and many studies have shown that the IL-17 level is increased in the serum, saliva, and tears in SS patients (15222324). In addition, activated pDCs interact with B cells, which produce BAFF. BAFF is an essential homeostatic cytokine for B cells that regulates both innate and adaptive immunity (25). IL-6 and BAFF are over-expressed in SS patients (26). The lack of tear production in SS subjects limited our selection of inflammatory parameters. Therefore, we analyzed the levels of ESR, IL-6, Th17 cells and BAFF in the serum and those of BAFF and IL17 in tears.
We evaluated the effect of HCQ on dry eye and systemic changes of inflammatory parameters. Serum and tear BAFF levels were not significantly changed. In two previous reports on BAFF levels after HCQ treatment, serum BAFF levels were decreased after HCQ medication, and tear BAFF levels were increased after HCQ discontinuation (827). However, the patients of these two reports constantly took oral HCQ mediation for more than 2 years before enrollment. This could have introduced a bias in that only patients whose condition had improved after HCQ medication remained on HCQ medication at the time of enrollment. ESR and serum IL-6 levels were not significantly changed, which was comparable with a previous study (9). However, there are a few reports that ESR and serum IL-6 levels were significantly decreased after HCQ treatment (710). Possible reasons for the lack of change in ESR and IL-6 are as follows: 1) HCQ may have no clinically beneficial anti-inflammatory effect. 2) Short-term usage (12 weeks) may have been inadequate to stop the chronic inflammatory process and vicious cycle, although an effective drug concentration is reached in the serum within 2 weeks. 3) Previous studies of HCQ in SS patients permitted low doses of oral steroid or topical cyclosporine A (828). Our patients were not allowed any other oral or topical anti-inflammatory medication, which may have caused the results in our study to differ from those of the other studies. 4) The small number of enrolled subjects might have prevented the results from reaching statistical significance. HCQ showed no definite effect on Th17 cells, and the possible reasons are as mentioned above. In addition, the dosage of 300 mg daily may not be sufficient to ameliorate inflammation such as that involving activated Th17 cells.
Regarding ocular changes, the Schirmer test score did not change significantly during follow-up after HCQ treatment and showed no difference between the groups, which suggests that the HCQ treatment did not affect tear production in this study. The presumed reasons for this finding are as follows: 1) HCQ actually has no clinically beneficial anti-inflammatory effect. 2) Considering the age of the subjects (mean age, 56.8 years), most of the lacrimal gland may have been destroyed by chronic inflammation before treatment. HCQ treatment may thus only affect tear production in younger individuals with early inflammation.
The subjective symptoms represented by the OSDI score improved while taking the medication in the HCQ group, but the difference was insignificant between the groups. The small group size may explain the lack of significant difference between the two groups.
Taken together, the present findings show that HCQ medication did not significantly improve pSS during the study period. However, we did not investigate all of the anti-inflammatory cytokines and inflammatory cells because of the small quantities of collected tears and blood. Therefore, we may have missed some other anti-inflammatory function of HCQ.
There were several limitations in this study. First, the appropriate sample size to obtain statistical significance could not be achieved. Many of the pSS patients were already taking oral medications such as HCQ, pilocarpine, steroids, or other immunosuppressants and were reluctant to stop these medications for a sufficient wash-out period. Furthermore, budget constraints prevented prolonging the study to achieve the targeted sample size. Second, the study schedule was short. Previous studies that reported significant positive results of HCQ in pSS ran for 12 months (7910) or included cessation of 3 months after 48 months or more of treatment (8). Third, the small number of enrolled patients may have prevented significant differences from being obtained. Fourth, symptoms (OSDI) and signs (Schirmer test) of patients in this study were milder than previous studies (829). Selection bias can affect the results. Nevertheless, our study is important because it supports other reports and provides evidence that HCQ does not have a definite beneficial effect on dry eye or systemic inflammation.
 XML Download
XML Download