

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The prevalence of atrial fibrillation (AF), the most common sustained arrhythmia, was 0.7% in adults 40 years of age or older and 2.1% in adults 65 years or older in Korea.1 As reported in several precedent studies, an increase in age is a risk factor in patients with AF,2 thus as the population is aging, the incidence rate of AF is likely to increase and hospital utilization rate and the mortality rate are expected to increase as well. In addition, AF is a disease that becomes a risk factor for stroke and systemic embolism.3 In particular, strokes accompanied by AF showed a higher mortality rate and hospitalization costs than strokes not accompanied by AF.456 According to the results of a study of the ratio of patients immobilized due to stroke, patients with strokes accompanied by AF showed a higher invalidity rate than patients with strokes not accompanied by AF (41.2% vs. 23.7%, P < 0.0005).5 Likewise, various studies showed that the prognosis is much worse when accompanied by AF than when not accompanied by AF.
The 2014 American Heart Association (AHA)/American College of Cardiology (ACC)/Heart Rhythm Society (HRS) guidelines recommend medicines for preventive treatment according to the risk of a stroke for a patient with AF.7 However, many study results showed that patients are receiving treatment that does not correspond to the treatment guidelines or have even received no treatment at all in real-world clinical scenes. According to a systematic literature review of 54 studies reported from 1998 to 2008,8 less than 70% of patients were treated with an anticoagulant even after they were determined to be in a high-risk group by the CHADS2 score used to determine the stroke risk level, and 2/3 of the studies reported that less than 60% of the patient group with a history of stroke or transient ischemic attack was treated.
Vitamin K antagonist (VKA), which is considered to be a standard of care among the anticoagulant medicines to prevent strokes in patients with AF, has a very narrow therapeutic range, thus regular monitoring is required to avoid potential adverse events.9 However, according to the results of the Korean Patients with Atrial Fibrillation (KORAF) study conducted on AF patients in Korea, the international normalized ratio (INR) was adequately controlled in only about 40% of patients treated with VKA.10 A comparative study on severe adverse events (SAE) such as death, occurrence of thrombosis related to an anticoagulant, and additional administration of heparin between a patient group that had a poorly controlled INR value and a patient group that had a well-controlled INR value revealed that the SAE incidence rate of the patient group that had a poorly controlled INR was higher than that of the patient group that had a well-controlled INR.11 Thus, INR control is important when using a VKA.
The purpose of this study is to investigate the clinical and demographic characteristics of Korean patients with non-valvular AF treated with VKA for stroke prevention and determine the ratio of patients who have a well-controlled INR, and also evaluate the difference between the group that has a well-controlled INR and the group that has a poorly controlled INR. In addition, we tried to identify the patients' satisfaction with VKA treatment, continuation rate, and reasons for discontinuation of treatment.
METHODS
Study subjects
This is a Korean Atrial Fibrillation Investigation II (KORAFII) study with a multicenter, prospective, non-interventional design. The patients were enrolled at 20 cardiology clinics nationwide from April 2013 to March 2014. The study subjects were selected according to the following inclusion criteria: 1) Patients who are 20 years of age or over and diagnosed with non-valvular AF, 2) Patients who newly start VKA treatment (Daehwa Warfarin 2 mg or 5 mg Tab, Daehwa Pharmaceutical, Hoengseong-eup, Korea; Jeil Warfarin 5 mg Tab, Jeil Pharmaceutical Co., Seoul, Korea; Kufarin 2 mg or 5 mg Tab, Hana Pharm Co., Seoul, Korea) to prevent a stroke and systemic embolism or have started VKA treatment within the last 3 months, 3) Patients with CHADS2 ≥ 1, 4) Patients for whom regular INR monitoring is considered possible by the researchers, 5) Patients for whom one-year follow-up is possible, and 6) Patients who can understand the description of the written consent and the consent form and submit the consent form.
Calculation of number of subjects
According to the related literature, about 50%12 of the patients treated with VKA discontinued VKA administration within 1 year, and thus received inappropriate care. Among the remaining 50% of patients who continued to receive VKA administration, about 60%1 (i.e., 30% of total patients) also received inappropriate care because their INR level failed to reach level 2–3. In other words, the adequate control ratio of INR for patients treated with VKA was about 20% at the maximum, and the number of final target cases calculated at 95% confidence level with a margin of error of ± 2.5% using the PASS 2008 program (NCSS, Kaysville, UT, USA)13 was approximately 1,000.1415 In this study, a final 877 patients were enrolled according to their voluntary consent to participate and the selection criteria from among patients treated with VKA in all participating medical institutions.
Study data and follow-up
In this study, the characteristics of patients and VKA usage patterns were identified by following up for 12 months after the patient enrollment date, and the data collected to investigate the INR control, VKA treatment satisfaction and so on were largely classified into investigation variables at the baseline and at the follow-up point. The following variables were investigated as the baseline characteristics of patients: 1) Demographic/clinical characteristics (sex, age, body mass index [BMI], date diagnosed with non-valvular AF/AF type) and 2) stroke and hemorrhage risk factors (components of CHA2DS2-VASc and HAS-BLED scores). In addition, demographic variables that could not be gathered by the medical record review (smoking, drinking, underlying diseases, occupation and education) were collected with a patient questionnaire. The VKA treatment patterns (date/values of INR measurement, continuation of VKA prescription, etc.) were collected by the medical record review during the follow-up period, and treatment satisfaction was investigated with two types of questionnaires (a simple questionnaire and the Treatment Satisfaction Questionnaire for Medication, or TSQM).
Degree of INR control
The degree of INR control (well controlled or poorly controlled) was identified by 12-month follow-up and assessed by the proportion of tests in a range method. Time in therapeutic range (TTR) was defined as the ratio of the days showed the optimal INR level (2.0–3.0) to total visit days during 12 months. And the well-controlled INR group was defined as patients who showed TTR in equal to or more than 60%. The poor-controlled INR group was defined as patients other than well-controlled INR. The cut-off value, 60%, was defined by the investigators using insight based on extensive clinical experience. The INR values used in the analysis were from the patients whose INR was measured at least once during the 12-month follow-up.
VKA treatment satisfaction
The treatment satisfaction of patients was assessed by two types of self-completed treatment satisfaction surveys of all patients. A simple questionnaire simply asked if the patient was satisfied with the treatment and investigated the cause and presented the results in a percentage if the patient was not satisfied. The TSQM, which was composed of four domains (effectiveness, side effects, convenience, and global) was conducted as another survey tool. The score, which is from 0 to 100, is graded by domain, and a higher score means greater satisfaction. Multiple linear regressions were conducted to find the variables that affected satisfaction for each TSQM domain.
Definition of time to reach optimal dose
The time to reach the optimal dose was defined as the time from the baseline point to the initial point (day) at which the INR values were “consecutively” maintained within 2–3 scores twice or more. The subjects whose INR values were not consecutively maintained within 2–3 scores twice or more at each point of value measurement were processed as censored, and the time from the baseline to the final INR measurement date was considered to be the censored observation time. The Kaplan-Meier survival function was used to assess the time when they reached the optimal dose.
Statistical analysis
Baseline characteristics of study subjects
Continuous data was displayed by means, standard deviations or medians and was analyzed using Student's t-test or analysis of variance to compare the characteristics by group. Categorical data was displayed by absolute frequency and rate and was analyzed using a χ2 test or Fisher's exact test to compare the characteristics by group.
RESULTS
Baseline characteristics
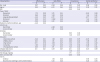
A total of 877 patients with NVAF (mean age, 67.7; males, 60.1%) were enrolled in this study. The mean CHADS2 scores of the patients was 1.85, and the ratio of high-risk group patients with scores of 2 or higher was more than half (56.0%). The mean CHA2DS2-VASc score was 2.9, and the ratio of high-risk group patients with scores of 2 or higher was considerable (83.6%). The mean HAS-BLED score was 1.5, and the ratio of high-risk group patients with scores of 3 or higher was 7.7% (Table 1).
Table 1
Baseline characteristics
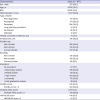
Data are presented as mean (standard deviation) or number (%).
BMI = body mass index, NVAF = non-valvular atrial fibrillation.
aUnknown: 149 cases.
![]()
Anticoagulation quality
During the follow-up period, among 852 patients whose INR was measured more than once, the cases in which VKA was discontinued accounted for 18.5%. Among the patients to which VKA was discontinued, 60.1% were changed to antiplatelets, and the medicine was changed to non-vitamin K antagonist oral anticoagulants (NOAC) in 37.3% among them. The number of patients who had a well-controlled INR were 226 (26.5%) (Table 2). Also, 335 patients newly started taking VKA and 215 among them maintained the optimal dose twice in a row during the follow-up period. The median time to reach the optimal dose twice consecutively was 154 days (95% confidence interval [CI], 133–179 days) (Fig. 1).
Table 2
VKA treatment and INR level of the patients who had INR measurement ≥ 1 during their follow up period

Data are presented as mean (standard deviation) or number (%).
VKA = vitamin K antagonist, INR = international normalized ratio, NOAC = non-vitamin K antagonist oral anticoagulants, TTR = time in therapeutic range.
![]()
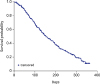 | Fig. 1Kaplan-Meier curve of time to optimal dose for VKA treatment with two-consecutive dose maintaining.VKA = vitamin K antagonist, CI = confidence interval.
|
The CHA2DS2-VASc score was higher in the group that had a well-controlled INR than in the group that had a poorly controlled INR (3.2 vs. 2.9, P < 0.001). Patients in the group that had a poorly controlled INR were younger than the group that had a well-controlled INR (66 vs. 72 years, P < 0.001) and had a higher HAS-BLED score (1.5 vs. 1.4, P = 0.03) (Table 3).
Table 3
Factors related with INR control (n = 852)

Data are presented as mean (standard deviation) or number (%).
INR = international normalized ratio, WC = well-controlled, PC = poor-controlled, BMI = body mass index, NVAF = non-valvular atrial fibrillation, VKA = vitamin K antagonist.
aP value calculated by χ2 test; bP value calculated by Student's t-test; cP value calculated by Mann-Whitney's U test.
![]()
Treatment satisfaction
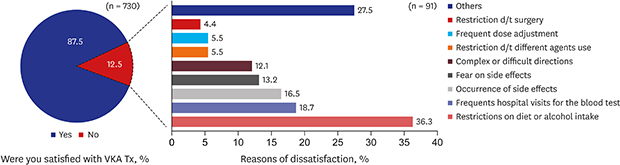
The patients' satisfaction with VKA treatment was investigated with a total of 730 patients (mean age, 67.9 years; males, 59.0%), and the mean of each domain of the TSQM was as follows: effectiveness (57.9 ± 12.0), side effects (96.3 ± 11.6), convenience (64.0 ± 13.5), and global satisfaction (55.6 ± 14.5) (Table 4). According to the simple questionnaire on treatment satisfaction, 91 patients (12.5%) replied that they were not satisfied with VKA treatment. The main reasons for dissatisfaction were restrictions on diet or alcohol intake (36.3%), frequent hospital visits for blood tests (18.7%), and side effects such as bleeding or bruising (16.5%) (Fig. 2).
Table 4
TSQM subscale scores (n = 730)

![]()
In multivariable linear regression analysis based on the univariate results and clinically selected variables, the associations with lower effectiveness score and global satisfaction score were shown in long standing persistent AF compared to that of first diagnosed AF (β = −5.6, P < 0.05; β = −6.8, P < 0.05). In addition, the presence of a comorbid mental condition compared to none was associated with lower effectiveness score (β = −4.5, P < 0.05). The higher convenience score was related to the higher VKAs dose (β = 1.7, P < 0.01), and high level education of at least post-graduation school compared to no education (β = 7.4, P < 0.05). Side-effect score was not related to any of the factors (Table 5).
Table 5
Multivariable linear regression analysis for TSQM scoresa
TSQM = treatment satisfaction questionnaire for medication, BMI = body mass index, NVAF = non-valvular atrial fibrillation, VKA = vitamin K antagonist, INR = international normalized ratio.
aAdjusted variables were selected from univariate results (P < 0.1) and other clinically selected variables by physicians; bP value calculated by multiple linear regression analysis. Reference category: sex (female), type of NVAF (first diagnosed), mental co-morbid conditions (No), alcohol use (non-drinker), smoking (non-smoker), education (no education), VKA treatment (discontinue & no switching to other antithrombotics), INR (poor controlled).
![]()
DISCUSSION
The results of this study showed that the elderly and males comprised high proportions of non-valvular AF patients, the same as the study previously conducted on Korean patients with AF.1 The ratio of high-risk patients with a mean CHA2DS2-VASc score of 2 or higher was 83.6%, which was comparable to the fraction (85.4%) in the pre-direct oral anticoagulant period (January 2011 to July 2013) in the previous study.16 On the other hand, the percentage of high-risk patients with a HAS-BLED score of 3 or higher was 7.7%, which was somewhat lower than the percentage (32.3%) in the previous study.16
During the follow-up observation period, the percentage of patients that had well-controlled INR was 26.5%, which was within the 16.7% (Asia)–49.4% (Europe) range in the GARFIELD-AF study,17 a worldwide observational prospective study. The INR was especially poorly controlled in Asia compared to other regions, which is interpreted as being due to the characteristics of AF patients in Asia who have lower INR values than patients in other regions.18
The reason why the CHA2DS2-VASc score was higher in the group where the INR was more well-controlled than the group that was not might be because the doctors paid more attention to INR control for the people to whom a stroke could cause more harm.19 The group where the INR was well-controlled had a higher HAS-BLED score, but the difference was not clinically significant. In addition, the reason why INR is better controlled in the elderly is perhaps because the doctors prescribed medicine more carefully, since the elderly group was reported to be the group with a high risk of having a stroke.1
Patients' satisfaction with VKA treatment was low overall in all domains except for side effects. In particular, comparing the global satisfaction score to the score of patients with other diseases (hypertension [72.1],20 epilepsy [68.4],21 and coronary heart disease [69.2]22) measured by TSQM, the measurement tool like ours, it showed a much lower satisfaction level. The reasons why the patients who replied to the simple question of satisfaction with the treatment that they were not satisfied were restrictions on diet or alcohol intake,2324252627 frequent hospital visits for blood tests2829 and occurrence of bleeding,303132 which were the same as those reported in previous studies.
The long duration of AF was a variable related to the low effectiveness of VKA treatment and overall satisfaction, and patients with co-morbid mental conditions showed low effectiveness of treatment. The higher the education level was and the higher the VKA prescription dosage was, the higher the convenience of VKA administration became. According to A PREFER in the AF Registry sub-study,33 the patients who switched to NOAC from VKA showed lower incidence rates of hypertension and heart valve dysfunction, fewer cases of combined therapy with antiplatelet/anti-inflammatory agents, and lower CHA2DS2-VASc scores. As shown in these results, it is likely that patients who had AF for a long time and were taking VKA had a more sensitive response to the effectiveness of treatment because the treatment effectiveness of VKA was lower than that of NOAC. In addition, there were many cases in which patients who had low anxiety/depressive traits expressed dissatisfaction with VKA and switched to another medicine.33
The limitations of this study are as follows: First, the participants in this study were patients who took part in it voluntarily, and the data was gathered at the time of their visit to the hospital as outpatients during the one-year follow-up period. Thus, the time of visit was different for each patient during the follow-up period. Second, unmeasured variables in this study were not considered as the potential confounders.
In spite of these limitations, in the real-world practice of Korea, INR was poorly controlled in patients. The principal reasons for dissatisfaction about VKA therapy were dietary restrictions, and regular monitoring etc. The global satisfaction score was lower among VKA users with NVAF than those of previous studies on treatment satisfaction in other diseases. Alternative oral anticoagulant therapy should be considered for patients with NVAF for enhancing treatment satisfaction and doing INR control well.
 XML Download
XML Download