

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Postoperative ileus (POI) is a common complication after abdominal surgery, and involves a temporary impairment in gastrointestinal (GI) motility following surgery.123456 POI is characterized by a lack of coordinated intestinal activity and a substantial overall reduction in peristalsis.
The clinical manifestations of POI vary, but include nausea, vomiting, abdominal distension, abdominal pain, inability to eat, or delayed passage of flatus and stool.567 Patients may develop bloating and bilious emesis. The small bowel typically recovers movement within hours, and the colon recovers in 3-5 days following surgery, but POI is clinically distinct from this GI dysfunction.1
POI after GI surgery constitutes a major burden for healthcare globally, and may require repeated surgical interventions.4 Adhesions can result in serious clinical complications, such as intestinal obstructions, inadvertent enterotomy at reoperation, and secondary female infertility. Such complications require medical care as well as additional difficult surgical interventions, increasing the healthcare costs and leading to further complications.8910
Intraperitoneal adhesions after abdominal surgery are the main cause of POI. Peritoneal adhesions form after healing of the peritoneal wound.2310 As a result, various interventions have been developed to separate the damaged peritoneum from the surrounding tissues.11 Several clinical studies have reported the use of anti-adhesive film (AAF) significantly reduces the incidence of POI.489101213141516171819
However, few studies have evaluated the preventive effect of AAF for POI after major hepato-pancreato-biliary (HPB) surgery. Many studies about POI have focused on colorectal and obstetric surgery. Thus, the purpose of this study was to examine the safety and efficacy of polylactic film (Surgi-Wrap®) as one of the anti-adhesion products after major HPB surgery.
Go to : 
MATERIALS AND METHODS
Study population
This retrospective cohort study was performed by reviewing the medical records of patients who had HPB surgery at Dongguk University Ilsan Hospital between October 2005 and November 2014. HPB surgery included pancreaticoduodenectomy, distal or subtotal pancreatectomy, hepatectomy, bile duct surgery, and extended cholecystectomy. All medical records were reviewed by a clinical research nurse and a general surgeon. All operations were performed by four surgeons who specialized in HPB surgery, using standard HPB surgical methods.
Polylactic film
Surgi-Wrap® (Surgi-Wrap MAST Bioresorbable Sheet, MAST Biosurgery Inc., San Diego, CA, USA) was used as the AAF material. Surgi-Wrap is a bioresorbable polymer sheet material fabricated essentially from the same lactic acid building blocks that occur naturally in the body.20 The safety and effectiveness of Surgi-Wrap has been evaluated in preclinical animal studies.2122 Several clinical studies have demonstrated that polylactic acid film significantly decreased the incidence and severity of adhesions, as it separates the tissue during wound healing.10161923 Surgi-Wrap® was selectively used preferentially by the surgeon, as an intraperitoneal spread just before wound closure after surgery.
Postoperative Ileus
POI is traditionally associated with a combination of upper and lower GI symptoms. A radiological investigation may be used in conjunction with the clinical diagnosis to confirm POI, but is usually reserved to exclude a bowel obstruction or a precipitating cause.179172425 In this study, POI was classified into early and late types. Early type POI was defined as patients having unusual functional GI symptoms within the initial admission period. Patients with early POI were unable to start oral feeding at post-operative 5th day due to GI symptoms, which were observed as radiologic intestinal obstructions. The late POI type was defined as patients re-admitted due to POI.
Statistical analysis
The data were analyzed with SPSS ver. 19.0 software (SPSS Inc., Chicago, IL, USA). The groups were compared using the independent t-test. A p-value ≤0.05 was considered significant. Continuous variables were reported as mean±standard deviation (SD), and categorical data were presented as numbers and percentages.
Go to :
RESULT
Patient clinical characteristics
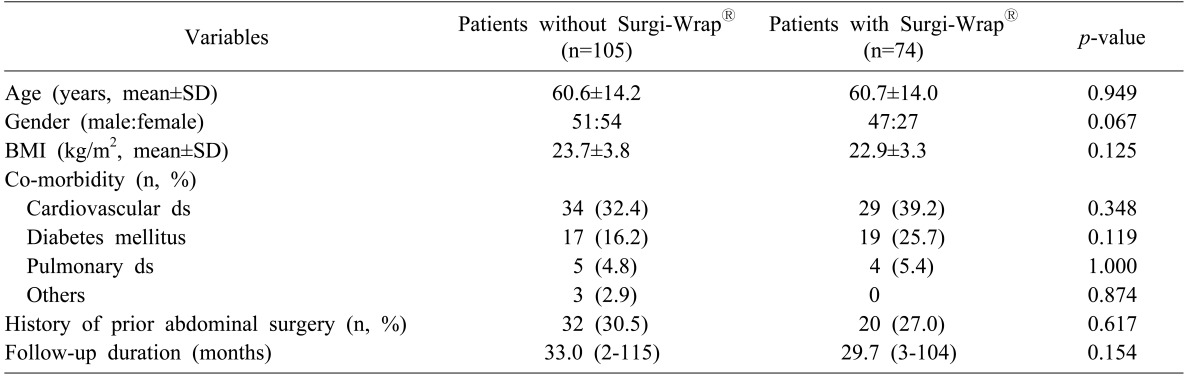
The study population consisted of 179 patients: 74 received Surgi-Wrap®, and 105 did not. No differences were observed in the patient characteristics, such as, age, sex, body mass index, co-morbidities, history of abdominal surgery, or follow-up duration between the groups (Table 1).
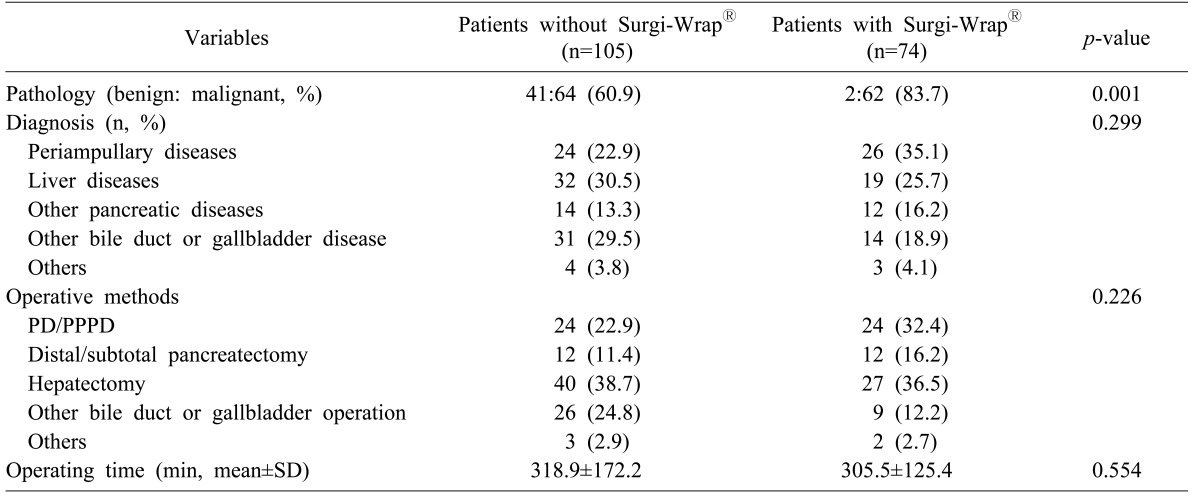
The proportion of patients with malignant disease was significantly higher in the group that received Surgi-Wrap® than in those who did not (60.9% vs. 83.7%, respectively; p=0.001; Table 2).
Clinical outcomes
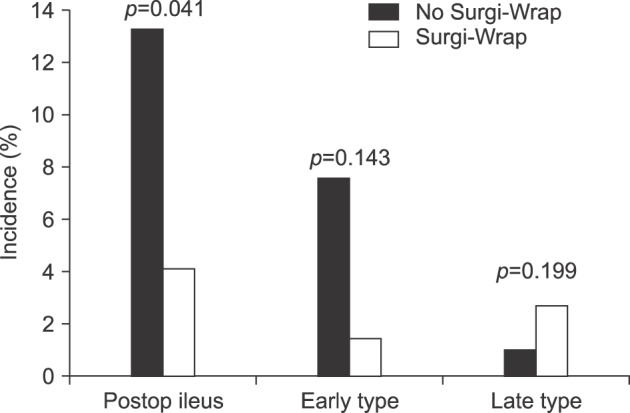
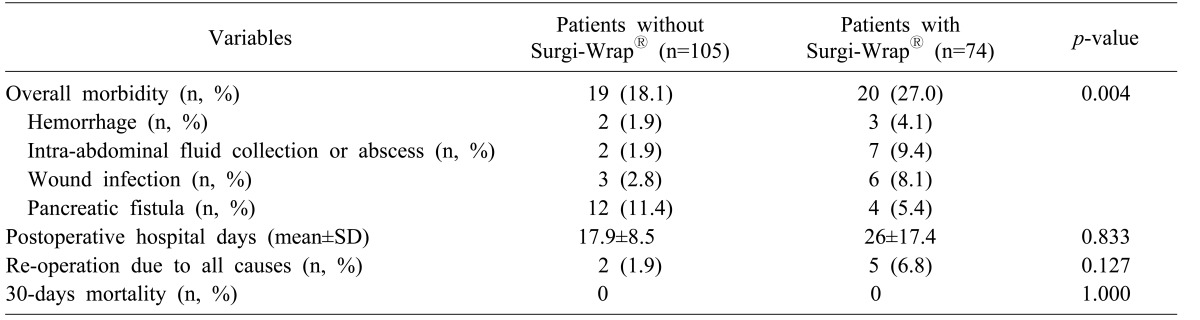
As shown in Fig. 1, patients without Surgi-Wrap® had a significantly higher POI rate than those with Surgi-Wrap® (n=14, 13.3% vs. n=3, 4.1%, respectively; p=0.041). All 17 patients were treated with conservative management. Patients who did not receive Surgi-Wrap® had a significantly lower morbidity rate than patients with Surgi-Wrap®, such as postoperative hemorrhage, intra-abdominal fluid collection, and wound infections (n=19, 18.1% vs. n=20, 27%, respectively; p=0.004; Table 3). On the other hand, rate of pancreatic fistulas was higher in patients without Surgi-Wrap® than in patients with Surgi-Wrap® (n=12, 11.4% vs. n=4 5.4%, respectively; Table 3). Re-operations were performed in 7 patients due to postoperative bleeding (n=3), wound dehiscence (n=2), and wound infection (n=2), all of which were unrelated to POI.
Go to :
DISCUSSION
Postoperative adhesions are a common cause of POI due to pathophysiology of peritoneal wound healing.1710 Postoperative adhesions account for 40% of POI cases, and 30-40% of these patients require reoperation to relieve POI.123 Effective methods are being researched to prevent adhesions, and a diverse clinical techniques and agents have been advocated for preventing postoperative adhesions, including anti-inflammatory agents, antibiotics, fibrinolytic agents, solution barriers, and synthetic solid barriers.145691126 Many studies have demonstrated the efficacy and safety of AAF for preventing POI, by separating the peritoneum from the damaged serosal area.910111213151617181923 Fazio et al.15 reported that AAF reduces POI after colorectal surgery, since their study observed a significant difference in the incidence of POI requiring reoperation, when compared with or without AAF. A prospective randomized trial in Korea showed that AAF significantly reduced POI after colorectal surgery.17 Conversely, other studies have reported that although AAF significantly reduced the severity of postoperative adhesions, no difference in the incidence of POI was observed.918 In the present study, the incidence of POI after major HPB surgery was significantly lower in the group of patients who received Surgi-Wrap® than those who did not (Fig. 1). Another study reported no benefit of Surgi-Wrap® in HPB surgery.27 The gastric stasis rate were 2.3% and 3.2% in Surgi-Wrap® group and control group, respectively (p=0.77). However, the incidence rate was too low in both groups, and further studies are necessary to prove the actual effect of Surgi-Wrap®.
In this study, the rate of other complications other than POI was higher in patients with Surgi-Wrap® than in those without Surgi-Wrap® (Table 3). Among these complications, intra-abdominal fluid collection or abscess occurred frequently in patients who received Surgi-Wrap® (Table 3). Several studies have reported the incidence rates of postoperative intra-abdominal abscess or fluid collection.48912141725 Some reported that AAF significantly increased the incidence of anastomotic leakage or intra-abdominal abscesses after surgery, and suggested that AAF may interfere with the formation of “good” adhesions created by the inflammatory response.912 Another possible reason is that Surgi-Wrap® could produce a foreign body reaction, and disturb absorption of the fluid and ascites remaining after surgery.
A wide range of natural and synthetic materials, including Surgi-Wrap®, are used as solid barriers and as absorbable or non-absorbable foil or membranes. Solid barriers must be directly applied to the damaged surface, which carries the risk of leaving uncovered wounded areas as a result of inappropriate application. The entire lesion must be covered and may need to be fixed with sutures, which can induce adhesions.10 Using liquid, low viscosity barrier materials could prevent abscess formation without acting as a solid physical barrier. They are easy to apply as compared to solid barriers, and the barrier cannot be placed incorrectly since the entire peritoneal cavity is covered.10 A prospective study has been planned in future, to confirm this hypothesis using a liquid barrier to prevent POI after major HPB surgery.
In this study, the incidence rate of wound infection was higher in patients with Surgi-Wrap® than without Surgi-Wrap® (Table 3). Theoretically, a surgical implant can affect the incidence of wound complications by a foreign body reaction.28 However, no differences in the incidence of wound complications have been observed in many other studies evaluating polylactic films.16202123 As a result, more observational or prospective studies are needed to confirm the safety of polylactic films for wound infections.
Some studies reported that patients receiving AAF experience a slightly greater frequency of pulmonary embolisms than those who do not.1213 However, other reports have suggested that AAF are safe with respect to pulmonary embolisms, when administered to patients undergoing abdominal surgery.25 In our study, none of the AAF or control patients experienced a postoperative pulmonary embolism (Table 3). Because of the relatively rare incidence of pulmonary embolism and the small cohort of our study, we are unable to comment conclusively on the relationship between Surgi-Wrap® and pulmonary embolism.
Interestingly, pancreatic fistulas were more frequent in patients who did not receive Surgi-Wrap® than in those who did (Table 3). Because pancreatic fistulas are a major complication after pancreatic surgery, numerous clinical studies have been conducted to prevent pancreatic fistulas.293031 However, no clear preventive methods to reduce pancreatic fistulas have been reported after pancreatic surgery. These results could be due to increased intraluminal pressure caused by postoperative adhesions that disturbs the flow of pancreatic juice into the anastomosed intestine or duodenum in patients without Surgi-Wrap®. We strongly expect that this will be a topic for future prospective trials to confirm this hypothesis.
This study had several limitations. As with all retrospective studies, the present study was limited in its ability to produce cause-effect relationships and to control all possible confounders. Because of the relatively small cohort of patients, it was impossible to perform subgroup or multivariate analyses, and contain heterogeneity of diseases or surgical procedures. Also, there were missing data values due to unavailable patient records and the retrospective nature of our analysis.
A limitation of Surgi-Wrap® as AAF lies in its handling characteristics, as it is brittle and difficult to apply. Moreover, since adhesions can form in all areas of the intra-abdominal cavity, it would be very expensive to apply this special covering to all areas. As mentioned above, liquid devices may be more useful in this setting. In the near future, we plan to perform a prospective study to test the preventive effect of a liquid AAF for POI after major HPB surgery.
In conclusion, use of Surgi-Wrap® during major HPB surgery decreased the incidence of POI. However, the frequencies of intra-abdominal fluid collection and abscess were higher in patients with Surgi-Wrap® than in those without Surgi-Wrap®. More evidence is needed regarding the efficacy and safety of Surgi-Wrap® to reduce POI, avoid repeated operative interventions, and for the improvement of quality of life. A further well-designed prospective randomized study to evaluate the effect of anti-adhesion products on POI after major HPB surgery is needed.
Go to :
 XML Download
XML Download