

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Cholecystectomy is a common surgical procedure in adults, but is relatively uncommon in children.12 However, the number of cholecystectomy in children has increased over the past two decades.34 The widespread use of ultrasonography for the diagnosis of the pediatric patients who present with abdominal pain has increased the diagnosis of symptomatic gallstones and the rate of cholecystectomy in the pediatric population.5 Some authors67 report that increasing obesity among children has increased the prevalence of gallstones in children and cholecystectomy rate.
In contrast to adults, gallbladder disease in children is usually observed primarily in patients with morbid conditions, such as hemolytic disorder.8 Recently, some reports indicated that the proportion of hemolytic disease has decreased and that of other conditions without hemolytic disease has increased.34 Although biliary dyskinesia is reported as the most prevalent cause of pediatric cholecystectomy in western populations,91011 symptomatic gallstones remain the most common cause of pediatric cholecystectomy and idiopathic etiology is estimated between 20 and 65%.81112
In Korea, the reports on pediatric cholecystectomy for gallstone disease13141516 are limited. The aim of this study was to describe our experience and characterize pediatric patients who underwent cholecystectomy for symptomatic gallstone disease unrelated to hemolytic disorder in a single center.
Go to : 
MATERIALS AND METHODS
We retrospectively reviewed the medical records of pediatric patients (under 18 years old) who underwent cholecystectomy due to gallstone disease between May 2005 and December 2015 at Chung-Ang University Hospital. Patients who underwent cholecystectomy due to other diseases such as hemolytic disorder were excluded. Basic demographic characteristics included sex, age, high, body weight, body mass index (BMI). Clinical characteristics included laboratory and radiologic findings, pathologic results, and operative outcomes. BMI equal to or greater than 25 kg/m2 was considered overweight. Complicated disease were defined as choledocholithiasis, gallstone pancreatitis, or empyema.
Statistical analyses
All statistical analyses were performed using the Statistical Package for the Social Sciences version 21.0 (SPSS, Chicago, IL). Comparisons of nominal data were conducted using the Chi-square test, and continuous variables were compared using the student t-test. Statistical significance was determined at p<0.05.
Go to :
RESULTS
A total 20 pediatric patients (under 18 years old) underwent cholecystectomy during the study period. One case was excluded due to gall stones caused by hemolytic anemia. Finally, 19 cases were selected as the subject group. The subjects included 9 males (47.3%) and 10 females (52.7%) with a mean age of 14.9 years (range, 5-18), with the majority (66.7%) being older than 12 years. Mean body weight was 57.3 kg (range, 13.9-93.3), and mean BMI was 21.7 kg/m2 (range, 12.3-35.1), with BMI>25 kg/m2 in 5 patients (26.4%). The majority of patients (n=16, 84.2%) presented with abdominal pain at the right upper quadrant.
Four patients were classified as complicated disease; 2 cases were choledocholithiasis, 1 was gallstone pancreatitis and the other was empyema. The choledocholithiasis cases were managed by endoscopic retrograde cholangiography (ERCP) before cholecystectomy. There were no postprocedural complications. One patient with acute pancreatitis was diagnosed as gallstone pancreatitis following comprehensive investigation; the patients' symptom resolved following cholecystectomy.
All 19 patients underwent laparoscopic cholecystectomy with no conversion to open procedure. Mean operation times and mean hospital stay was 53.2±11.0 minutes and 5.4±2.9 days, respectively. There were no postoperative complication and no mortality.
Stone analysis indicated cholesterol stones in 10 patients (55.6%), and black pigment stones in 8 patients.
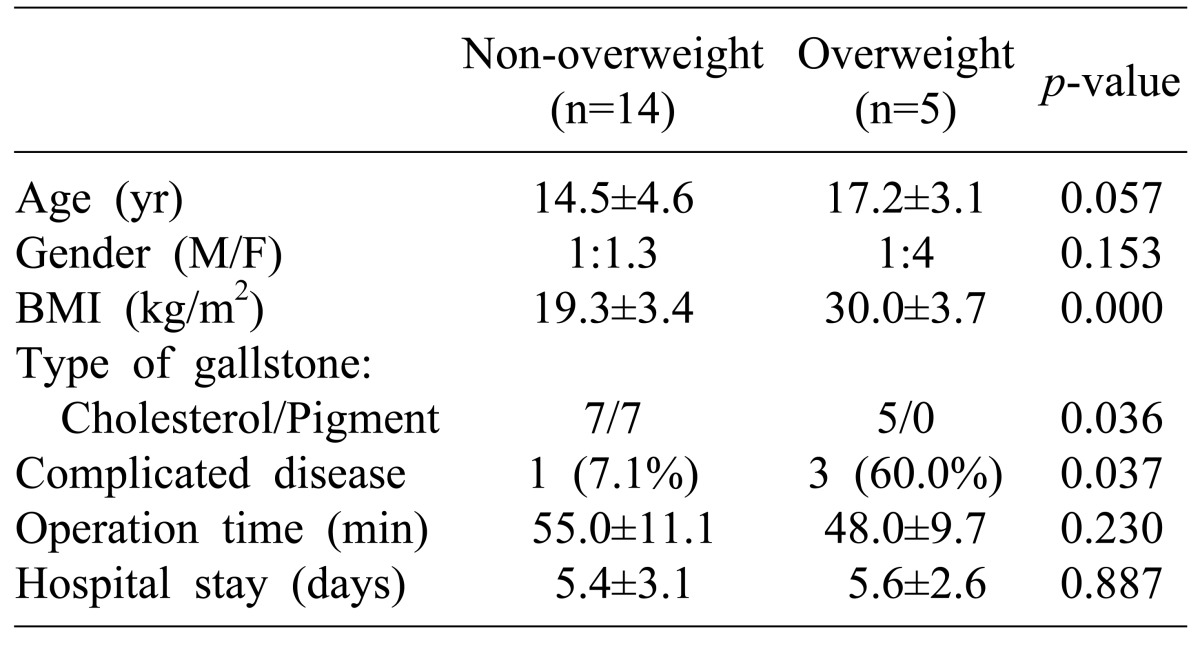
Comparison between overweight and non-overweight patients revealed that significantly more overweight patients had cholesterol stones (5/5 vs. 7/14, p=0.036) and were classified as complicated disease (3/5 vs. 1/14, p=0.037) (Table 1).
Postoperative diagnoses confirmed by pathologic examination were acute or chronic cholecystitis (17 cases), empyema (1 case), and adenomyomatosis (1 case).
Go to :
DISCUSSION
Cholecystectomy is rarely performed in pediatric patients, but is a very common operation in adults. Recently, several studies have reported increasing cases of cholecystectomy in pediatric patients, and change in the indication for cholecystectomy from hematologic disease to non-hematologic gall stone disease.35 The reason for the increase in cholecystectomies in the pediatric population is likely multifactorial. The widespread use of abdominal ultrasound in the diagnosis of non-specific abdominal pain5 and increasing prevalence of obesity in children67 are considered as main reasons for the increased rate of cholecystectomy. However, a genuine increase in the incidence of cholelithiasis is expected from recognized predisposing factors, such as total parenteral nutrition, obesity, and prematurity, etc.1611 In western counties, there has been an increasing rate of cholecystectomy for biliary dyskinesia789 and in the United States, biliary dyskinesia is an indication in 20-50% of cholecystectomies.1718 In the present study, during study period only one patient (5%) underwent cystectomy due to gallstones related to hemolytic anemia.
While boys and girls are equally affected in early childhood, as in adults, most previous studies reported a female predominance in pediatric gallbladder disease starting from puberty.45 In the present study, we found equal sex distribution overall and even above the age of 12 years. Although the reason of the discrepancy is unclear, in Eastern countries, the female predominance is not apparent even in adults.19
There is clear association between obesity and gallstone formation, especially in early puberty.20 However, this phenomenon is only now gaining recognition in the pediatric population.212223 Compared to adults, it can be somewhat difficult to accurately evaluate childhood obesity in terms of BMI and this has led to inconsistent results in the previous reports.424 In our study, 5 patients were classified as overweight; of these, significantly more patients had cholesterol stones than the non-overweight patients (5/5 vs. 7/14, p=0.036). The result suggested that obesity is associated with the formation of cholesterol stones. In the overweight patients group, significantly more patients were classified as complicated disease (3/5 vs. 1/14, p=0.037); thus, overweight might be a potential aggravating factor in pediatric gallstone disease. Thorough evaluation and more care are recommended in obese pediatric patients with gallstones.
Acute and chronic cholecystitis, ascending cholangitis, common bile duct stones and choledocholithiasis, and pancreatitis are the major problems and complications observed in patients with gallstone. The frequency of complications varied in the published literature. Generally, choledocholithiasis is found in 8-10% of adult patients with cholelithiasis and 10% to 15% of pediatric patients with gallstones.521 Two patients with choledocholithiasis in the present study were successfully managed by ERCP without complications. However, considering the 11% complication rate that accompanies ERCP in children and the high rate of general anesthesia for the procedure,2526 effective management method of choledocholithiasis remains debatable.
In Western countries, biliary dyskinesia is an increasingly recognized diagnosis and an indication for surgery in 20-50 % of cholecystectomies.789 The diagnosis of biliary dyskinesia is defined as gallstone-like pain attacks combined with an ejection fraction below 35% during hepatobiliary iminoacetic acid (HIDA) scanning.27 Supportive scientific evidence for cholecystectomy in cases of biliary dyskinesia is not adequate. Further prospective randomized trials with long-term follow-up are needed to determine the true efficacy of surgical treatment of biliary dyskinesia.
In conclusion, because overweight patients can experience complications such as choledocholithiasis or gallstone pancreatitis, more careful evaluation and management for overweight patients is needed. It is difficult to suspect symptomatic gallstones in pediatric patients who present with abdominal pain due to symptoms that are rarely clear-cut. However, because the rate of symptomatic gallstones has increased in the pediatric population, pediatricians and surgeons should have a high suspicion for gallstone disease.
Go to :
 XML Download
XML Download