

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Oxybutynin, tolterodine, propiverine, and solifenacin provide a therapeutic benefit in children with overactive bladder (OAB) in the clinical practice, but to our knowledge the optimal anticholinergic dose is still unknown (1). In pediatric patients with OAB, there are extensive difficulties in initiating and managing clinical studies, including enrollment issues due to non-approval of the solifenacin by the Food and Drug Administration in children, an insufficient placebo group, a lack of a regular follow-up after disappearance of OAB symptoms, parental consent, and others (2). Therefore, most prospective studies about anticholinergics medication have had failure of treatments after behavioral and medical therapy or presence of neurogenic bladder as inclusion criteria (1345).
Solifenacin is a once-daily formulation, and studies have shown that it significantly decreased OAB symptoms with few adverse effects (AEs) in adult patients with OAB (6). However, most studies on solifenacin treatment for pediatric OAB are retrospective. There have been only a few prospective studies on pediatric OAB that included mostly small numbers of patients (457). Until now, there have been limited data on the real use and benefits of solifenacin 5 mg fixed dose in pediatric patients with newly diagnosed idiopathic OAB. Therefore, we prospectively investigated the efficacy and tolerability of solifenacin 5 mg fixed dose in patients with newly diagnosed idiopathic OAB in our present study.
MATERIALS AND METHODS
Study design and patients
A total of 43 children with idiopathic OAB were evaluated from 6 hospitals between January 2012 and September 2014, and 34 patients who satisfied the inclusion criteria were prospectively enrolled. Idiopathic OAB was defined by the urgency or symptoms of urinary frequency (> 8 micturitions per 24 hours), with or without urgency urinary incontinence (UUI). Study inclusion criteria included no previous history of anticholinergic treatment for OAB and an age between 5 and 12 years. Exclusion criteria included the presence of neurological anomalies, psychological diseases, such as attention deficiency and hyperactivity disorder and mental retardation, sleep disordered breathing, and congenital urogenital abnormalities (e.g., posterior urethral valves, vesicoureteral reflux, ectopic ureter, or ureterocele). Patients who had or were being treated for primary monosymptomatic nocturnal enuresis, patients with urinary tract infection (UTI), kidney, liver, intestine, cardiovascular system and psychological problems, and patients with dysfunctional voiding in the emptying phase were also excluded from this study, as were patients who were allergic to anticholinergic agents or for the use of these drugs was contraindicated. Correctable diseases such as UTI and phimosis with preputial stricture were considered acceptable in our study cohort after correction.
Children with suspected OAB completed a screening visit (visit 0), including a complete questionnaire to determine the OAB symptom score (OABSS) (8) and symptoms related to AEs, physical examination, urine analysis, electrocardiogram (ECG), kidney and bladder ultrasound 2 weeks before initial solifenacin medication (Fig. 1). At the enrollment visit (visit 1), the patients and their parents were taught about standard urotherapy and received solifenacin 5 mg after study enrollment and underwent uroflowmetry with post-voiding residual urine (PVR). Standard urotherapy included explanation about patient's condition according to individual voiding diary, appropriate voiding, adequate fluid intake and avoiding the voiding postponements. PVR was checked using an ultrasound device (BladderScan® BVI 3000; Verathon, Bothell, WA, USA). We evaluated the questionnaire responses including current symptoms and AEs, physical examination findings, and the maximal bladder capacity (MBC)/micturition, mean volume voided (MVV)/micturition, and mean number of voiding episodes/every 24 hours from 3-day voiding diaries every month (visits 2–4) for three months. MBC and MVV were defined as biggest volume and average volume in 3-day voiding diary, respectively. Follow-up uroflowmetry with PVR was performed at 2 or 3 months after the beginning of solifenacin medication (visit 3 or 4).
Fig. 1
Study protocol.
OABSS = overactive bladder symptom score, PVR = post-voiding residual urine, AEs = adverse effects, ECG = electrocardiogram, F/U = follow-up.

Among the 34 children included in our study series, there were 16 boys and 18 girls (mean age: 7.2 ± 2.3 years; range: 5–12). All of these children had urgency, and 27 (79.4%) had UUI. The mean duration of OAB symptoms before anticholinergic treatment was 31.2 ± 15.2 months. The OABSS total score was 7.7 ± 4.2. The mean urinary frequency was 9.4 ± 3.0 times per day, and the average bladder capacity was 90.3 ± 44.4 mL. The peak flow rate was 16.4 ± 8.6 mL/sec, and the PVR was within 40 mL.
The OABSS questionnaire included frequency (score 0–2), nocturia (score 0–3), urgency (score 0–5), and urgency incontinence (score 0–5). The OABSS total score resulted from the sum (score 0–15) of the scores for each item (questions 1 to 4 of Table 1) (8). It has been proposed that the Korean version of the OABSS might offer clinicians a valid and reliable tool for the assessment of OAB symptoms in the Korean population (9). AEs were assessed using Common Terminology Criteria for Adverse Events (CTCAE) version 4 (10).
Table 1
Overactive bladder symptom score (OABSS) questionnaire

Statistical analysis
All statistical analyses were two sided, with a P < 0.05 considered significant. Data were analyzed using IBM SPSS Statistics Version 21 (IBM Corporation, Somers, NY, USA). The Student t-test, paired t-test, and Mann-Whitney U-test were used to compare the parameters in the pre-treatment and post-treatment of groups. Descriptive statistics are expressed as means ± standard deviation. All statistical analyses were 2-sided and P < 0.05 was considered statistically significant.
Ethics statement
This open-label, single-group, prospective 12-week study was conducted in 6 institutions. The study protocol was approved by the Institutional Review Board of each hospital (e.g., Ulsan University Hospital IRB No. 2011-09-084) and by the Korean Food and Drug Administration. Written informed consent was obtained from each of the parents and patient consent was obtained in all cases. Clinical data on all the patients were prospectively obtained from the medical records and questionnaires.
RESULTS
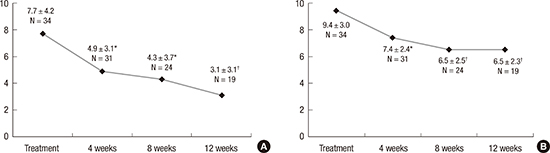
The mean OABSS total score significantly decreased after 4 weeks of solifenacin treatment (P = 0.002). After 4, 8, and 12 weeks of treatment, the mean OABSS total score also gradually decreased from 7.7 ± 4.2 to 4.9 ± 3.1, 4.3 ± 3.7, and 3.1 ± 3.1, respectively (Fig. 2A). The urgency domain significantly improved from 3.0 ± 1.8 to 1.1 ± 1.1 (P < 0.001) after the 12-week treatment, and complete resolution of urgency occurred in 38.9% of patients. The UUI domain also significantly improved from 2.0 ± 1.7 to 0.7 ± 1.0 (P < 0.001), and the percentage of children with UUI among urgent patients decreased from 79.4% to 57.1% (Table 2). There were no children with re-aggravation after improvement during the continued 12 weeks of solifenacin treatment.
Fig. 2
Treatment outcomes.
Overactive bladder symptom score (OABSS) (A) and frequency (B) had significantly improved after 12 weeks' treatment of solifenacin.
*P < 0.01; †P < 0.001.

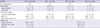
Table 2
Treatment outcomes of solifenacin at a 5 mg fixed dose in the study cohort
According to the 3-day voiding diaries, the mean voiding frequency during daytime significantly improved from 9.4 ± 3.0 to 7.4 ± 2.4 (P = 0.002), 6.5 ± 2.5 and 6.5 ± 2.3 times after 4, 8, and 12 weeks, respectively (Fig. 2B). The MVV increased from 90.4 ± 44.4 to 156.2 ± 67.3 mL after 12 weeks of treatment (P < 0.001). The MBC also increased from 180.5 ± 73.4 to 206.7 ± 79.7 mL after 12 weeks of treatment; however, this difference was not statistically significant (P > 0.05).
On uroflowmetry, the maximum flow rate did not change (from 16.4 ± 8.6 to 16.6 ± 8.6 mL/sec) and the PVR slightly decreased from 14.5 to 10.7 mL, without statistical significance.
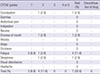
Drug-induced AEs were reported in only 7 of these cases (20.6%) in our current study cohort. Dry mouth occurred in only one (2.9%) patient (Table 3). There were no cases of hypertension, hypotension, or admission to the hospital because of AEs from the medication.
Table 3
Common Terminology Criteria for Adverse Events (CTCAE) findings in the study cohort
DISCUSSION
OAB can have a major impact on health-related quality of life (11). The prevalence of pediatric OAB is relatively high (16.6% in children between 5 and 13 years of age), although it is slightly lower than the rate in adults in Korea (12). Therefore, many urologic or pediatric doctors have adopted the use of various anticholinergics, including solifenacin (13). However, there have been few reports regarding the efficacy of solifenacin for newly diagnosed idiopathic OAB in children.
In our current study, we prospectively investigated the efficacy and tolerability of solifenacin (5 mg fixed dose) in Korean children with newly diagnosed idiopathic OAB. The urgency domain in these cases significantly improved after the 4 weeks of treatment with solifenacin (P < 0.001). Moreover, the mean urgency domain score gradually decreased from 3.0 ± 1.8 before treatment to 1.1 ± 1.1 after 12 weeks of medication. Complete resolution of urgency occurred in 38.9% of cases. Our study series included a high proportion of children with UUI symptoms among the subjects with urgency. The percentage of children with UUI among urgent patients decreased from 79.4% to 57.1%, and the UUI domain score also decreased from 2.0 ± 1.7 to 0.7 ± 1.0 after 12 weeks of medication. The efficacy of the treatment in our current study is difficult to compare with those of previous studies on the use of solifenacin, because inclusion criteria and definitions of efficacy are often heterogeneous in different publications. We educated parents for patients to perform the standard urotherapy. Standard urotherapy itself might have improved OAB symptoms. Hoebeke et al. (7) retrospectively reported an 85% positive response and AE frequency of 6.5% after treatment with solifenacin 5 mg in 138 children with oxybutynin-resistant non-neurogenic OAB. Another small, nonrandomized, uncontrolled study on the combination of two anticholinergics including 10–30 mg oxybutynin and 4 mg tolterodine and/or 5–10 mg solifenacin in children obtained satisfactory results (4). In a study of 72 children (27 with a neurogenic bladder) with OAB refractory to oxybutynin or tolterodine, solifenacin was an effective alternative to improve symptoms (5). In a recent Korean retrospective study, solifenacin among various anticholinergics had a 66.7% improvement rate (13).
The long-term use of solifenacin during 5.6 months might elevate the improvement rate of urgency (66.7%) rather than the resolution rate (38.9%), as highlighted in the current study. In an earlier prospective randomized placebo-controlled phase 3 clinical trial, 8 weeks of medication with propiverine yielded similar results to the findings of our study (2). In that report on 171 randomized children, there was a decrease in voiding frequency (−2.0 episodes for propiverine vs. −1.2 for placebo; P < 0.001) and an improvement in incontinence episodes (−0.5 vs. −0.2 episodes per day; P < 0.001). Similarly, in another retrospective and observational cohort study, after administration of propiverine 15.1–15.5 mg/day (n = 437) or oxybutynin 9.6–9.8 mg/day (n = 184), continence was achieved in 61.6 vs. 58.7% of children with OAB of age 5–14 years (1415). Until now, there have been no reports on the clinical efficacy of fesoterodine, although a study has been published on its pharmacokinetics, safety, and tolerability (16).
In our present analysis, the MVV was increased from 90.4 ± 44.4 to 156.2 ± 67.3 mL after a 12-week treatment (P < 0.001). MBC was also increased from 180.5 ± 73.4 to 206.7 ± 79.7 mL after 12 weeks of treatment, although without statistical significance (P = 0.247). The MBC of 219 healthy Korean children aged 3–13 years in a previous study was 232.7 ± 84.6 mL (range: 161–301 mL) from 3-day voiding diaries (17). Although the symptoms improved in the OAB patients in our current study, the MBC after a 12-week treatment with solifenacin was still less than that of the healthy population. We think that OAB patients' groups included the MBC of unimproved patients after treatment unlike healthy population. Therefore, the above-mentioned retrospective Korean study presented results similar to those of our current study, as the MBC was significantly increased from 145.5 ± 66.9 to 196.8 ± 80.3 mL (13).
Drug-induced AEs were found in only 7 of the cases (20.6%) in our current study. According to a previous Korean study that included 326 children with OAB, all AEs occurred in only 14 (4.3%) children. 6 of whom (1.8%) had interrupt to their medication as a result (13). This lower AE incidence, similar to that (6.5%) reported in the study of Hoebeke et al. (7) may have been caused by the retrospective nature of the analyses, as compared with our current prospective study, i.e., it is possible that not all AEs were recorded in these earlier reports. In reality, it is unlikely that patients and their parents will be queried about AEs in detail by the treating physicians unless it is part of a planned prospective study. However, the incidence of AEs in our present study was as still lower than that reported in adult OAB patients 32%–47% (18192021). Moreover, the frequencies of dry mouth and constipation were extremely low in our current series, and arose in only one (2.9%) patient, respectively.
Our study has several limitations. First, there was a significant drop off over the twelve weeks of the protocol. Only 19 (56%) of enrollees completed the protocol. Solifenacin has been not approved for children although many doctors already have used for pediatric OAB (13). Therefore, we respected the parents' opinion to decide whether to continue the study or not. However, 4 of 15 enrollees who dropped off wanted to stop the protocol due to symptom improvement and only one stopped the study due to no symptom improvement. We lost follow-up of ten enrollees (Fig. 1). It is supposed that solifenacin had a good or no effect for them, or their parents just freely wanted a new drug to know the efficacy of solifenacin for them. Second, we could not check the ECG after the 12-week treatment although we did not use a dose titration. Therefore, we meticulously checked the clinical symptoms and AEs from a self-reported form and history taking simultaneously. Third, urodynamic data is missing. Despite these limitations, our study results contain important and practical information for the treatment of solifenacin 5 mg fixed dose in children with OAB. Solfenacin at a dose 5 mg is effective against OAB symptoms in children with an acceptable tolerability without significant AEs.
 XML Download
XML Download