

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Osteoporosis is recognized worldwide as a major public health problem because it results in skeletal fractures that cause mortality, morbidity, and large health care expenditures (123). The reported prevalence of osteoporosis in the general population aged 50 years or more in Korea is 37.3% in women and 7.5% in men (4). This condition is treatable and fractures are preventable (5). Nevertheless, approximately 30% of women will be diagnosed with osteoporosis and about half of them will receive treatment following a fragility fracture (67). This situation in Korea is consistent with other studies. A recent study reported that the treatment rate for osteoporosis in Korea was only 12.8% in the general population (4).
To prevent osteoporotic fractures, a number of intervention programs have been introduced that have reported improvements in osteoporosis diagnosis and treatment. However, most studies were focused on hospitalized patients and/or those with fragility fractures (89101112). In addition, most community-based intervention studies focused on exercise-related programs that reduced the incidence of falls and thereby resulted in fewer osteoporotic fractures (13). Several studies regarding pharmaceutical treatments have shown the reduction rate of osteoporotic fractures range from 30% to 70% (141516). Theoretically, an intervention study using screening test and education of osteoporosis in community-dwelling populations is possible to improve diagnosis and treatment rate of osteoporosis and resulted in prevention of osteoporotic fracture.
This prospective intervention study was undertaken in order to study the impact of osteoporosis screening test and education on the treatment rate. In addition, we evaluated the change in prevalence of osteoporosis from 2004 to 2015 in the same cohort in Ibansung-myeon, Jinju, Korea.
MATERIALS AND METHODS
Study cohort
The cohort is based on Ibansung-myeon, Jinju-shi, which is located in the southern part of the Korean peninsula and has 23 towns with their own community centers. The population consisted of 1,795 persons (869 men and 926 women) in 2013. Of them, there were 960 persons aged 50 years and older. This cohort has the following relevant characteristics. First, movement of the population is less common than in other cohorts. Second, 90% of the population works in the agricultural sector. Finally, the population of this cohort has been decreasing since 2000 because of mortality. Since 1999, we have been performing an intermittent observational study evaluating the incidence of hypertension and osteoporosis (1718). In 1999, of 2,714 people, we performed an epidemiologic study to evaluate the incidence of hypertension in 1,440 people aged 30 years and older (17). In 2004, of 2,284 people, 735 people aged 50 years and older were tested for bone mineral density (BMD) using ultrasound bone densitometry (18). We included 960 people aged 50 years and older. We excluded people who were no longer residents of Ibansung-myeon or death.
Study design
From November 1, 2014 to August 31, 2015, 960 eligible candidates from 23 community centers were recruited through an announcement in the public office and by 2 health care providers. Patients provided written informed consent and baseline data in Table 1 was collected from each participant.
Table 1
Demographic characteristics

Intervention
The intervention involved a tailored education program on aspects of osteoporosis, including risk factors, BMD testing, lifestyle modification, calcium and vitamin D intake, and medications. Patients' BMDs were measured with a quantitative heel ultrasound (QUS) measurement using a GE Lunar Achilles Insight quantitative ultrasound densitometry machine and provided with printed educational materials (brochure developed by the Korean Society for Bone and Mineral Research). Interpretation of the results was discussed with each patient, and the QUS was reinforced as a tool to help with osteoporosis risk assessment rather than as a diagnostic test for osteoporosis.
Patients were encouraged to follow up with their primary care physician for further management. Additionally, study details were sent to the primary care physician for each patient, including information that their patient was eligible for BMD testing by the central dual-energy X-ray absorptiometry (DXA) based on national guidelines; the QUS results were also sent, with clinical interpretation. The researchers revisited the community centers after the initial visit 3 months later. The follow-up reinforced the previously delivered educational messages and determined if any of the study endpoints had been reached.
Outcome measures
Primary outcome measures were a composite endpoint of a BMD test with central DXA or the initiation of a new prescription medication for osteoporosis (any bisphosphonate, nasal calcitonin, raloxifene, teriparatide, or hormone therapy) within 6 months of study entry. Endpoints were measured by patient self-report and confirmed by receiving a copy of the BMD measurement from the primary care physician. The secondary outcome was the trend of osteoporosis in the same cohort.
Statistical analysis
A χ2 test was used for categorical variables and reported P values were 2 sided, with P < 0.05 indicating statistical significance. To evaluate trends in the prevalence of osteoporosis from 2004 to 2015, adjustments using population of Ibansung-myeon in 2014 were performed. Statistical analyses were performed using SPSS software version 19.0 (SPSS Inc., Armonk, NY, USA).
RESULTS
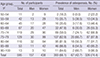
Of the 960 potential participants, 865 were included; 88 individuals did not live in Ibansung-myeon any longer and seven people had died. Of these, 595 people (68.8%; 157 men and 438 women) took bone densitometry measurements and completed the questionnaire. The mean age of the participants was 74.0 years (range, 51–94 years; mean age, 73.3 years for men and 74.3 years for women) (Fig. 1). Demographic characteristics of the 595 participants were described in Table 1. Of them, 205 persons had previously been diagnosed with osteoporosis and 104 persons were under treatment with anti-osteoporotic medication. The prevalence of osteoporosis (T score ≤ −2.5) as assessed by measurements with a GE Lunar Achilles Insight quantitative ultrasound densitometry machine was 393 people (66.1%) (67/157 [42.7%] for men and 326/438 [74.4%] for women) (Table 2).
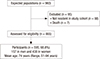
Table 2
Prevalence of osteoporosis by gender and age
Of the 595 participants, 263 persons (40.8%; 57 men and 186 women) underwent repeated screening tests between 2004 and 2015. The mean age at the screening test in 2015 was 76.9 years (76.3 years for women and 78.5 years for men). The prevalence of osteopenia and osteoporosis changed from 95 people (39.1%) and 117 people (48.1%) in 2004 to 46 people (18.9%) and 180 people (74.1%) in 2015, respectively. During the 11-year follow-up interval, 63 of 126 people (50.0%) who were diagnosed as normal or as having osteopenia progressed to having osteoporosis. After adjusting for the population in 2014, the prevalence of osteoporosis had increased from 43.1% to 54.3% during the study period (Table 3).
Table 3
Trend of prevalence of osteoporosis by adjustment with population of Ibansung-myeon in 2015

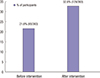
Of the 393 participants diagnosed with osteoporosis, excluding 85 participants who were undergoing management of osteoporosis prior to the start of the study, 65 participants received bone densitometry measurements while hospitalized and osteoporosis management was newly initiated in 44 participants. The osteoporosis management rate in the cohort increased from 21.6% to 32.8%, with osteoporosis diagnosed in 66.2% of participants at the latest follow-up (Fig. 2).
DISCUSSION
The results of this study indicate that the rate of detection and treatment of osteoporosis after intervention with screening tests with ultrasound bone densitometry and educational programs increased from 21.6% to 32.8%, with osteoporosis diagnosed in 66.2% of participants at the latest follow-up. Intervention studies that have investigated the treatment rates of osteoporosis have seldom been reported in the literature. This study demonstrates an effective and easily applicable intervention method.
The prevalence of osteoporosis as assessed by our methods is quite difficult to compare with that of other studies because of the equipment used for bone densitometry, the characteristics of our study population such as age and gender, and ethnic differences. Recently, Choi et al. (4) evaluated the prevalence, diagnosis rate, and treatment rate of osteoporosis in 4,946 adults aged 50 years or older using data from the fourth Korean National Health and Nutrition Examination Survey 2008–2009. They reported that the prevalence of osteoporosis was 35.5% in women and 7.5% in men and the diagnosis and treatment rate were 26.2% and 12.8%, respectively (4). In 2004, we performed screening for osteoporosis in 735 adults in the Ibansung cohort aged 50 years or older (mean age, 69.4 years in men and 69.0 years in women) using ultrasound bone densitometry. The prevalence of osteoporosis was 48.4% (28.7% in men and 57.4% in women). In 2015, we performed a follow-up study using ultrasound bone densitometry in the same cohort and found that the prevalence of osteoporosis had increased from 48.4% to 66.1% (42.7% for men and 74.4% for women). Another study documented trends in the prevalence of osteoporosis and incidence of hip fracture using single-photon absorptiometry at the distal radius in 456 women aged 50 years or over who lived in the same city. They reported no change in the prevalence of osteoporosis but an increase in the incidence of hip fractures during three separate time periods (26).
To improve the diagnosis and treatment of osteoporosis in community-dwelling populations, several intervention studies have been performed using phone call services, e-mails, patient education, screening tests for osteoporosis, and combinations of these methods (19202122). The outcomes were inconsistent. Heyworth et al. (19) reported that interactive telephone voice services were effective in improving screening for osteoporosis, but e-mail services were not. Studies using screening tests for osteoporosis with ultrasound bone densitometry have been proven effective at initiating diagnosis and treatment of osteoporosis in a community cohort (20232425). Elliott et al. (23) performed an observational study after screening for osteoporosis using peripheral bone densitometry in 133 women who lived in a community. They reported that 20% had calcaneal osteoporosis and nine women (7.0%) received further evaluation using central DXA or started osteoporosis treatment. Naunton et al. (25) performed an observational study after screening using heel ultrasound bone densitometry and an educational program for 345 elderly women living in a rural area and found that 38 (11.0%) had had a BMD test. Yuksel et al. (20) performed a prospective randomized control study on 262 patients and reported that BMD or osteoporosis treatment was done for 28 patients (22.0%) compared with 14 controls (11.0%) (relative risk [RR] 2.1; 95% confidence interval [CI] 1.1–3.7). In this study, of the 393 participants diagnosed with osteoporosis, excluding 85 participants who were already diagnosed with osteoporosis, 65 (21.1%) participants additionally received bone densitometry measurement while hospitalized and osteoporosis management was newly initiated in 44 (14.3%). Our findings are similar to those of previous studies.
This study has several limitations. First, measurement of osteoporosis using ultrasound bone densitometry was performed at community centers in each county. Therefore, persons who had severe mobility problems and lived far from their community center could not participate in this study. These issues are the main reason why only 68.5% of candidates could complete measurement of and education for osteoporosis. Second, the education level of participants and the small print in the educational booklets made it difficult for some to understand the effect of osteoporosis management and the importance of exercise. Finally, ultrasound bone densitometry is known to have a lower rate of reproducibility and limitations rendering it unsuitable for monitoring patients' response to treatment (27). In addition, different types of ultrasound bone densitometry were used to measure bone density in 2004 and 2015.
In conclusion, this prospective intervention study demonstrated a high rate of osteoporosis. Screening test and an educational brochure increased the treatment rate from 21.6% to 32.8%. Therefore, dissemination of knowledge about osteoporosis and a better understanding of osteoporotic fracture risks can be helpful in increasing the treatment rate of osteoporosis in community-dwelling individuals.
 XML Download
XML Download