

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Upper tract urothelial cancer (UTUC) is an aggressive disease associated with significant morbidity and mortality (1). At presentation, 30% of patients demonstrate invasive and/or locally advanced disease, 30%–40% have regional lymph node (LN) involvement, and 20% harbor metastatic disease (2). Radical nephroureterectomy (RNU) with bladder cuff excision is considered the standard of care for most invasive UTUCs, but distant relapses are common following surgery for locally advanced, high-grade disease (3). For patients with advanced disease, systemic recurrence and progression rates range from 45%–60% (2). The 5-year survival rates for patients classified with pT2- and pT3-stage disease are 73% and 40%, respectively, and the median survival for patients with T4 stage disease is approximately 6 months. Given the inadequacy of radical surgery alone for patients with regionally advanced UTUC, a multimodal approach that includes perioperative chemotherapy regimens seems to be a promising approach (4). Systemic chemotherapy in an adjuvant or neoadjuvant setting with local tumor control was adopted in the 2013 National Comprehensive Cancer Network guideline (5). Nevertheless, there is lack of consensus regarding the accurate identification of patients who may benefit from adjuvant chemotherapy and determine what factors are barriers to systemic therapy eligibility. Renal insufficiency following RNU and nephrotoxic chemotherapy regimen seem to be challenges preventing the effective delivery of cisplatin-based chemotherapy (678). Although general condition and systemic illness could be barriers for perioperative chemotherapy and also significant determinants of survival, the prognostic influences of comorbidity/performance indices on eligibility for adjuvant chemotherapy and survival in patients with UTUC remains unclear.
The American Society of Anesthesiologists Physical Status (ASA-PS) classification system was first introduced in 1940 and has been updated and now includes a 6-point scale, ranging from a healthy person (class 1) to one with a severe systemic disorder that is a constant threat to life (class 4). Class 5 was representing for moribund persons not expected to survive 24 hours, with or without surgery and the 6 class is now used for declared brain-dead organ donors (9). The ASA-PS classification was originally designed as a standardized way for anesthesiologists to convey information about the patient's overall health status that allows outcomes to be stratified by a global assessment of their illness severity. In practice, however, the ASA-PS score is frequently used to explicitly or implicitly estimate operative risk because it is the only instance for which overall preoperative condition is consistently preoperatively recorded for a large number of patients, and it correlates well with surgical mortality and morbidity (9). Moreover, the ASA-PS system has a unique ability to quickly and concisely summarize multiple patient characteristics (10).
In this study, we tested our hypothesis that the ASA-PS system, as an assessment of systemic comorbidity/performance indices, may be associated with eligibility for adjuvant chemotherapy and potentially unfavorable survival outcomes in patients with UTUC who underwent RNU in 4 centers in Korea.
MATERIALS AND METHODS
Study population and data collection
We performed a retrospective analysis of 505 patients treated with RNU for UTUC at four academic centers in Korea. The database listed patient characteristics including age, sex, body mass index (BMI), bladder cancer history, surgical approach (open vs. laparoscopic), tumor stage, grade, LN status (lymphovascular invasion), concomitant carcinoma in situ, tumor location, use of adjuvant chemotherapy, prior endoscopic therapy, tumor multifocality, disease recurrence, and mortality from UTUC. The ASA-PS classification was obtained from the anesthesia chart. All of the patients who had complete follow-up data available were considered for the analysis. A computerized databank was generated for the data transfer. After combining the data sets, reports were generated for each variable to identify inconsistencies and other data integrity problems. Prior to the final analysis, the database was frozen, and the final data set was produced for the current analysis (by HYS). Patients with an incomplete data set or those who received neoadjuvant chemo/radiotherapy were excluded. To avoid biasing the survival estimates, we also excluded patients with a history of radical cystectomy (RC) for treatment of previous or concomitant muscle-invasive bladder tumor, distant metastases at diagnosis, and perioperative mortality within 1 month. The final study group comprised 416 patients.
Protocols for surgery and pathologic evaluation
RNU was performed by a standard double-access procedure (11). The kidney, ureter, and a bladder cuff were excised en bloc. The hilar and regional LNs adjacent to the ipsilateral great vessel were generally resected if they were palpable intraoperatively or suspected based on preoperative imaging. All surgical specimens were processed according to the standard pathologic procedures at each institution. The tumors were assessed according to the 2002 American Joint Committee on TNM classification (12). Tumor grading was performed using the 1998 World Health Organization/International Society of Urologic Pathology consensus classification (13). Tumor multifocality was defined as the synchronous presence of multiple tumors in the renal pelvis or ureter. Locally advanced UTUC was defined as ≥ pT3 and/or pN1 disease.
Follow-up protocol
After surgery, each patient was monitored according to the standard guidelines (14). In general, patients were evaluated every 3–4 months for the first year following RNU, every 6 months from the second through fifth years, and annually thereafter. The follow-up included history taking, physical examination, routine blood and serum chemistry lab work, urinary cytology, chest radiography, cystoscopic evaluation of the urinary bladder, and radiographic evaluation of the contralateral upper urinary tract. Elective bone scans, chest computed tomography, or magnetic resonance imaging was only performed when clinically indicated. Adjuvant chemotherapy was administered at the surgeons' discretion based on tumor stage and overall health status.
Deaths were determined by reviewing medical records, and time to cancer-specific mortality (CSM) was calculated as the time from surgery to the date of cancer-attributable mortality. Any patients who died without any proof of metastasis or recurrence were considered to have cancer-independent mortality (CIM).
Statistical analysis
Continuous variables are shown as medians and interquartile ranges (IQRs). Differences in variables with continuous distributions across dichotomous categories were assessed using Mann-Whitney U tests. Fisher exact and χ2 tests were used to evaluate associations between categorical variables. Cohorts were defined by ASA-PS classification, and then pathologic results and adjuvant chemotherapy eligibility were compared. Kaplan-Meier curves for overall survival (OS) and cancer-specific survival (CSS) were generated and compared using log-rank tests based on ASA-PS classification. A subgroup analysis for locally advanced UTUC patients who may benefit from adjuvant chemotherapy was also performed. Univariate and multivariate survival analyses were performed using the Cox proportional hazard regression model.
Differences were considered significant at P < 0.05, and all reported P values are 2-sided. Analyses were performed using SPSS 20.0 software (IBM Corp., Armonk, NY, USA).
Ethics statement
The study was carried out in agreement with the applicable laws and regulations, good clinical practices, and ethical principles as described in the Declaration of Helsinki. The Institutional Review Board of Chungbuk National University approved this study protocol (Approval No.: GR2014-12-009). Informed consent was waived by the board.
RESULTS
Baseline characteristics
The clinical and pathologic characteristics of the patient cohort are shown in Table 1.
Table 1
Clinicopathologic characteristics of patients

Overall, 259 (62.3%) patients underwent laparoscopic nephrectomy, and the remaining 167 (38.0%) patients underwent open RNU. The stage distribution was 5.5% Ta, 1.9% Tis, 32.7% T1, 26.2% T2, 31.5% T3, and 2.2% T4. Overall, 75.2% had high-grade UTUC. A total of 207 (49.7%) patients underwent concurrent regional LN dissection and 18 (4.3%) had metastasis to regional LNs. Adjuvant chemotherapy was administered to 62 (14.9%) patients including 17 with localized but high-risk UTUC and 45 patients with locally advanced UTUC (defined as ≥ pT3 and/or pN1 disease).
ASA-PS score and adjuvant chemotherapy eligibility
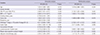
Of the 416 patients included in this study, 118 (28.4%), 262 (63.0%), and 36 (8.7%) were assigned to the score 1, 2, and 3 groups, respectively (Table 1). Patient age was significantly increased with higher degrees of ASA-PS classification (P < 0.001) (Table 2). In addition, patients placed in higher ASA-PS classes were less likely to be eligible for adjuvant chemotherapy in the total cohort (P = 0.029) (Table 2) and in the subgroup analysis limited to patients with locally advanced UTUC (P = 0.007) (Table 3). There were no significant differences according to ASA-PS classification in terms of other clinicopathologic characteristics including sex, history of previous or concomitant bladder cancer, pathologic stage or grade, LN status (lymphovascular invasion), tumor necrosis, concomitant carcinoma in situ, tumor location, or multifocality (all P > 0.05) (Table 2).
Table 2
Comparison of clinicopathologic parameters according to ASA-PS classification in UTUC patients treated with RNU
ASA-PS = American Society of Anesthesiologists Physical Status, UTUC = upper tract urothelial carcinoma, RNU = radical nephroureterectomy, SD = standard deviation, IQR = interquartile range, BMI = body mass index, BC = bladder cancer, CIS = carcinoma in situ.
P value was based on the *Mann-Whitney U test or †Fisher exact test.
Table 3
Adjuvant chemotherapy status according to ASA-PS classification between the locally advanced and localized UTUC

ASA-PS score and survival in patients treated with RNU for UTUC
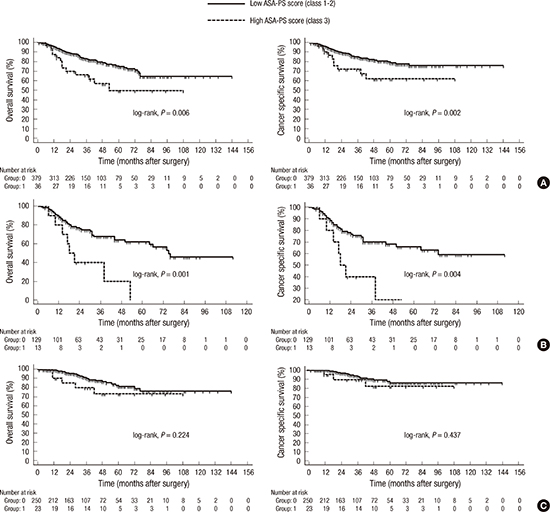
The median follow-up period of the study cohort was 30 months (IQR 15 to 52 months). During follow-up, 62 (14.9%) patients died of UTUC. Kaplan-Meier estimates showed that high-risk group (ASA 3) had a poorer OS and CSS compared to the low-risk group (ASA 1–2) in the total and locally advanced UTUC cohorts (Fig. 1A and 1B). However, there was no significant survival impact of ASA-PS score on OS or CSS in patients with localized UTUC (P = 0.475 and P = 0.399, respectively) (Fig. 1C). Multivariate Cox regression analysis revealed that age (hazard ratio [HR], 1.033; 95% confidence interval [CI], 1.004–1.062; P = 0.025), lower BMI (HR, 1.675 95% CI, 1.020–2.753; P = 0.042), tumor size (HR, 1.008; 95% CI, 1.001–1.015; P = 0.020), locally advanced stage (HR, 2.482 95% CI, 1.415–4.353; P = 0.002), lymphovascular invasion (HR, 1.991; 95% CI, 1.180–3.360; P = 0.010), and high ASA-PS score (HR, 1.919; 95% CI, 1.017–3.619; P = 0.044) were independent predictors of overall mortality (OM) (Table 4). Moreover, lower BMI (HR, 1.933; 95% CI, 1.115–3.350; P = 0.019), locally advanced stage (HR, 2.703; 95% CI, 1.417–5.157; P = 0.003), lymphovascular invasion (HR, 2.600; 95% CI, 1.469–4.602; P = 0.001), positive surgical margin (HR, 2.110; 95% CI, 1.025–4.342; P = 0.043), and high ASA-PS score (HR, 2.120; 95% CI, 1.023–4.394; P = 0.043) were independent predictors of CSM (Table 5).
Fig. 1
Kaplan-Meier analysis of OS and CSS in (A) total cohort, (B) subgroup with locally advanced tumor, and (C) subgroup with localized tumor in patients treated with RNU for UTUC.
OS = overall survival, CSS = cancer-specific survival, RNU = radical nephroureterectomy, UTUC = upper tract urothelial carcinoma, ASA-PS = American Society of Anesthesiologists Physical Status.
Table 4
Univariate and multivariate Cox regression models for the prediction of OM in UTUC patients treated with RNU
Table 5
Univariate and multivariate Cox regression models for the prediction of CSM in UTUC patients treated with RNU
DISCUSSION
In this study, we evaluated the prognostic value of the ASA-PS scoring system on adjuvant chemotherapy eligibility and survival in a multi-center cohort of patients with UTUC treated with RNU. Our results show that the ASA-PS classification as an assessment of systemic comorbidity/performance indices was associated with adjuvant chemotherapy eligibility and potentially unfavorable survival in this patient group.
Comorbidity and performance status indices are useful clinical tools to estimate the risk of comorbidities, which may guide decision making regarding operative procedures or multimodal therapy approaches. The most commonly used comorbidity indices in the literature are the Charlson comorbidity index (CCI, age-adjusted Charlson comorbidity index [ACCI]), the ASA-PS, the Adult Comorbidity Evaluation-27 (ACE-27), the Eastern Cooperative Oncology Group (ECOG) performance status, and the Karnofsky Performance Status scale (KPS). The ASA-PS score was first described in 1940 by Saklad (15) and is the oldest evaluation score that assesses perioperative risk. Although the ASA-PS score was originally designed as a uniform system for anesthesiologists to convey information about the patient's overall health status, it has been shown to accurately predict perioperative morbidity and mortality (91617). Furthermore, numerous studies have suggested that the ASA-PS score as an assessment of systemic comorbidity/performance indices may provide prognostic information in many cancer surgeries including urological malignancies such as prostate, bladder, and renal cell carcinoma. Anudeep and colleagues found that ASA-PS score was associated with OS after minimally invasive partial nephrectomy for renal cell carcinoma (18). The survival impact of ASA classification was also recognized in the radical prostatectomy setting (192021). The predictive capacity of the ASA-PS scoring with regard to OM and CSM in patients who underwent RC for bladder cancer remains unclear (222324). Several studies have also supported the prognostic role of comorbidity/performance indices in patients with UTUC after RNU. For example, a large national multi-center collaborative study found that the ASA classification significantly correlated with CSS after RNU for UTUC. In this study, the 5-year CSS differed significantly between ASA 1, 2, and 3 patients (83.8%, 76.9%, and 70.6%, respectively), and there was a threefold higher risk of OM and CSM at 5 years for patients rated as ASA 3 compared with ASA 1 (25). In a recent study by Aziz et al. (26), 4 comorbidity indices (ASA-PS, CCI, ACCI, and ECOG-PS) were compared with regard to recurrence-free survival (RFS), CSS, OS, and CIM. The ACCI and ECOG-PS were associated with RFS and CSS, whereas the ASA-PS and ACCI scores were associated with CIM.
Our results were similar to those described in previous studies in which a high ASA-PS score was associated with poorer survival in patients with UTUC who underwent RNU. However, the present study is unique for several reasons. We analyzed the survival influence of ASA-PS classification on the total cohort and also performed subgroup analyses for patients with localized or locally advanced UTUC. We found that the survival influence of ASA-PS classification was limited to locally advanced UTUC. There were no significant differences with regard to OS or CSS between the low and high ASA-PS groups in patients with localized disease. Thus, radical surgery for localized UTUC might be reasonable and appropriate in patients with comorbidities. Of course, patients with a higher ASA have a higher need for preoperative optimization and critical postoperative care. Another strength of our study was that it considered a potential effect of adjuvant chemotherapy on survival outcomes in patients treated with RNU for UTUC. Such regimens could influence the long-term survival, especially CSS. Patients with a higher ASA-PS class tended to less likely to be prescribed adjuvant chemotherapy in the locally advanced stage, and decreased eligibility for adjuvant chemotherapy in the high-risk ASA category may influence poorer survival in these patients. Although there is lack of evidence regarding a survival benefit for perioperative platinum-based chemotherapy in patients with high-risk UTUC, adjuvant chemotherapy in this clinical setting may have an effect on survival given the high risk of relapse in patients with locally advanced UTUC (27).
Our study had several inherent weaknesses. There are limitations due to the retrospective and multicentric nature of the study; we excluded patients for whom we could not obtain complete information, which could have led to selection bias. Moreover, we could not adjust for surgeons' preferences, experience, or surgical techniques. There was also a lack of centralized pathologic review. However, all surgeons and pathologists operated at centers dedicated to the management of UTUC that followed the standard practice guidelines. Because comorbidities were measured using ASA-PS scores obtained from the anesthesia chart, an effect of interobserver variability in ASA scoring between different anesthesiologists at the four study institutions cannot be ruled out. Finally, we did not have access to data on perioperative renal function, which could be confounding factor affecting chemotherapy eligibility. Nevertheless, our study provides evidence supporting the use of the ASA-PS classification to determine adjuvant chemotherapy eligibility and survival in patients with UTUC after RNU.
In conclusion, high ASA-PS score was significantly associated with reduced eligibility for adjuvant chemotherapy and poorer survival of patients with UTUC after RNU. The subgroup analysis revealed that the influence of ASA-PS score on survival was limited to patients with locally advanced UTUC. The lower feasibility of adjuvant chemotherapy in the high-risk ASA category may contribute to the lower survival rate in this group.
 XML Download
XML Download