

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Smoking is known to negatively affect female reproductive function. It has been associated with diminished ovarian reserve, increased risk of infertility, and decreased rate of fertilization and pregnancy following in-vitro fertilization (IVF) treatment (12345). In women undergoing IVF, the number of retrieved oocytes and live births were lower in smokers compared to never-smokers (4). However, in some studies, smoking was not associated with differences in the number of retrieved oocytes, fertilization rate, or miscarriage rate in IVF cycles (678). In a study of 127 Korean women undergoing intrauterine insemination (IUI) or IVF, pregnancy outcome was not affected by urinary cotinine positivity (9).
In a nationwide survey conducted by the Korean government, the incidence of smoking in 2012 was 43.6% in men and 7.9% in women aged 19 years or higher (10). In one study, the prevalence of positive urinary cotinine among infertile Korean women was 10.2%, which is higher than the rate reported in the nationwide survey (9). However, the prevalence of secondhand smoking was not reported among the infertile Korean women. Secondhand smoking has been associated with greater difficulty becoming pregnant and delayed conception in several studies (111213). Moreover, epidemiologic studies investigating smoking-associated personal factors in infertile Korean women are not currently available.
Here, we report the results of a large-scale questionnaire-based survey performed in 6 infertility centers in Korea. By using a self-reported questionnaire along with hospital records, we assessed the prevalence of current, secondhand, past, and never smokers, and we investigated possible associations between smoking and personal habits, major diseases (including depression), menstrual characteristics, and reproductive hormone levels in infertile Korean women.
MATERIALS AND METHODS
Study subjects
This study was a part of a multicenter survey comprised of 1,000 infertile women. Six major fertility clinics in Korea participated in this study (Seoul National University Hospital, Seoul National University Bundang Hospital, Maria Infertility Clinic, Hamchoon Women's Clinic, CHA Medical Center, and Ajou University Hospital).
Women who visited the infertility clinics between April and December 2014 were asked to participate in the study. Among the 1,000 women who chose to participate during this time period, 129 women with unknown smoking status and 86 women over the age of 42 years were excluded. Women over the age of 42 years were excluded because they have higher incidence rates of major diseases, menstrual irregularity, and reproductive hormone levels. Thus, a total of 785 women were included in the analyses. Seven past smokers were excluded from the analysis of variable parameters according to smoking status because this group had a small number of subjects. Women who were past smokers as well secondhand smokers were assigned to the secondhand smokers group.
Questionnaires
All participating women anonymously completed a structured, self-report questionnaire. The questionnaire included age, weight, height, final level of education (high school, college or higher), job status (with or without job), alcohol consumption (yes or no), sleep hours per day, exercise habits (days per week of mild, moderate, vigorous, and weight-training exercise), obstetric history, past medical and surgical history, current illness, age at menarche, irregular menstrual period (yes or no), duration of menstrual flow (days), and dysmenorrhea (yes or no).
Stress level was assessed by the 10-point Likert scale question, from 1 (no stress) to 10 (unbearable stress). A feeling of despair lasting 2 or more weeks during the previous year was also recorded (yes or no).
Cause of infertility and serum reproductive hormone levels (luteinizing hormone [LH], follicle stimulating hormone [FSH], estradiol, basal or random thyroid stimulating hormone [TSH], prolactin, and anti-Müllerian hormone [AMH]) were collected from medical records. Basal levels were recorded for LH, FSH, and estradiol, and basal or random levels were recorded for TSH and AMH. The age-related decrease in AMH levels were taken into account, and we compared them as its absolute value as well as age-specific multiples of the median (MoM) value calculated using the Korean reference value for each corresponding age. In the analysis of serum levels of TSH, women diagnosed with thyroid disease were excluded.
Beck Depression Inventory (BDI)
We used a modified and validated Korean version of the BDI (14). This is a widely-used questionnaire, which contains 21 items. Each item describes a specific thought or behavior associated with depression and scores for each item range from 0 to 3. Scores from each item were summed and 4 degrees of depression were assigned; these included no depression (sum 0–9), mild depression (sum 10–15), moderate depression (sum 16–23), and severe depression (sum 24–63). Subjects with self-reported depression were excluded from the BDI analysis.
Statistical analysis
Analysis of variance (ANOVA) with Bonferroni post-hoc tests were used to compare numerical variables between current, secondhand, and never smokers. χ2 or a Fisher's exact tests were used to compare proportions between groups. Statistical analysis was conducted using SPSS version 22.0 (SPSS Inc., Chicago, IL, USA). A P value below 0.05 was considered statistically significant. When missing data exceeded 25% of all subjects for a variable, the variable was not analyzed.
Ethics statement
The Institutional Review Board at each of the six hospitals (Seoul National University Hospital, Seoul National University Bundang Hospital, Maria Infertility Clinic, Hamchoon Women's Clinic, CHA Medical Center, and Ajou University Hospital) approved the study (IRB No. 1408-018-601, Seoul National University Hospital). Informed consent was obtained from all women prior to participation of the study.
RESULTS
Smoking status
Among 785 women, current, secondhand, past, and never smokers represented 12.7% (n = 100), 45.7% (n = 359), 0.9% (n = 7), and 40.6% (n = 319) of the study population, respectively. The prevalence of secondhand smoking among women that were not current smokers was 52.4%.
Participant characteristics
Age, age at marriage, body mass index (BMI), number of spontaneous or artificial abortion, and current number of children were similar between current, secondhand, and never smokers (Table 1). The proportion of primary infertility was significantly higher in the secondhand smokers (90.0%) than in current smokers (82.0%, P = 0.035) or never smokers (81.5%, P = 0.002). The cause of infertility did not differ based on smoking status (Table 1). Female factor infertility details are also shown in Table 1.
Table 1
Obstetric history and diagnosis of infertility

Participant habits
The proportion of women with college or higher education was significantly lower in current smokers (72.0%) than in secondhand (83.2%, P < 0.001) or never smokers (92.5%, P = 0.012) (Table 2). The proportion of employed women was highest in secondhand smokers (65.1%), and this was significantly higher than in never smokers (46.8%, P < 0.001).
Table 2
Educational level and job status

Alcohol consumption was more prevalent in current smokers (86.0%), and this was significantly higher than in secondhand smokers (70.8%, P = 0.002) or never smokers (65.5%, P < 0.001) (Table 3). Sleep duration was highest in current smokers, and this was significantly higher than that in secondhand smokers (7.7 vs. 7.4 hours, respectively, P = 0.041). The frequencies of mild, moderate, and vigorous exercise per week were similar between groups. However, the frequency of weight-training exercise was significantly higher in the current smokers (0.6 ± 1.4) than in secondhand smokers (0.5 ± 1.1, P = 0.038) or never smokers (0.3 ± 0.8, P = 0.006).
Table 3
Behavioral parameters
Medical history and current illness
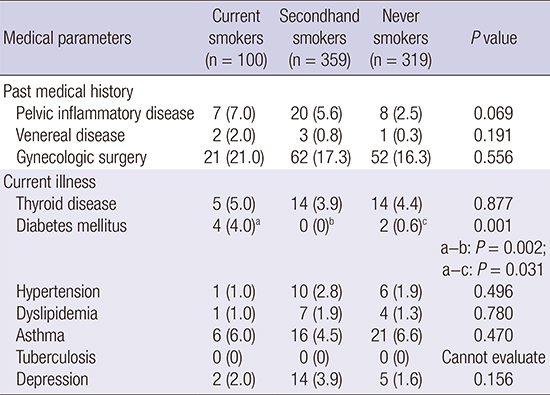
Self-reported history of pelvic inflammatory disease, venereal disease, or gynecologic surgery was similar between groups (Table 4). The prevalence of thyroid disease, hypertension, dyslipidemia, asthma, tuberculosis, or depression was also similar between groups; however, the prevalence of diabetes mellitus was significantly higher in current smokers (4.0%) than in secondhand smokers (0.0%, P = 0.002) or never smokers (0.6%, P = 0.031).
Table 4
Self-reported past medical history and current illness
Stress and BDI
Daily stress level was highest in the secondhand smokers and was significantly higher than that in never smokers (5.9 vs. 5.6, respectively, P = 0.017) (Table 5). The percentage of women who reported despair in the past year was similar between groups, but none of the current smokers received treatment for despair. After excluding women with self-reported depression and women who did not complete the BDI, there were no differences between groups for the mean BDI score or the prevalence of mild, moderate, and severe depression.
Table 5
Stress and degree of depression

Gynecologic characteristics
The age at menarche, duration of menstrual flow, and percentage of women reporting an irregular period or dysmenorrhea were all comparable between groups (Table 6). Similarly, comparable menstrual characteristics were also observed after excluding women with known polycystic ovary syndrome (n = 122). Reproductive hormone serum levels did not differ between groups (Table 7), and similar serum hormone levels were observed after excluding women with known polycystic ovary syndrome (Table 8).
Table 6
Menstrual characteristics

Table 7
Serum levels of reproductive hormones
Table 8
Serum levels of reproductive hormones after excluding women with polycystic ovary syndrome

DISCUSSION
Here we firstly reported the prevalence of current, secondhand, and never smokers in infertile Korean women. The observed prevalence of current and active smoking (12.7%) was slightly higher than the 7.9% among women aged ≥ 19 from a nationwide survey reported by the Korean government and the 10.2% observed among infertile Korean women based on urinary cotinine measurement (910).
In the previous researches, the prevalence of secondhand smoking has been reported in two manners. In some studies, the prevalence of secondhand smoking was reported as the proportion of secondhand smokers among all women. The National Health and Nutrition Examination Survey (NHANES) III (1988–1991) estimated 33% of all women in the United States were secondhand smokers based on self-reports (15). When calculated likewise, the prevalence of secondhand smoking in our study was 45.7%. Considering the lower prevalence of current female smokers in Korea compared to the United States (7.9% vs. 18.8%, respectively), this is considerably high (1016). Secondhand smoking has also been reported as the proportion of secondhand smokers among those who are not current smokers. The second and third US National Reports on Human Exposure to Environmental Chemicals (part of NHANES; NHANES 1999–2000, 2001–2002, respectively) reported measurable urinary cotinine in approximately 50% of women who were not current smokers (17). In a study based on the 2008 Korea National Survey for Environmental Pollutants in the Human Body, the prevalence of self-reported secondhand smoking among women who were not current smokers was 39.2% (18). Calculated based on this method, the prevalence of secondhand smoking was 52.4% in our study, which was a 13.2% absolute difference. This difference may have been due to our subjects being comprised of infertile women under high stress, or it may have been due to the different distribution of employed women in our study group compared to that in the general population.
Secondhand smoking has been associated with difficulty becoming pregnant, delayed conception, increased pregnancy losses, increased risk of preterm labor, and increased incidence of chromosomal abnormalities and congenital malformations (12131719). The influence of secondhand smoking, compared to direct smoking, on natural or IVF pregnancy have not been studied in depth, and needs further investigation.
In the present study, current smokers were less educated and more likely to consume alcohol than secondhand or never smokers. Although a strong association between smoking behavior and lower educational status or alcohol consumption has previously been reported (20), we firstly confirmed these relationships in infertile women.
Employed women were more prevalent in the group of secondhand smokers, and this may be related to more frequent exposure to secondhand smoke in their workplace. Although the age at marriage was not significantly different among groups, working women tend to try to get pregnant later in life, and this may be an explanation why secondhand smokers were more likely to be diagnosed with primary infertility than current smokers or never smokers. This may also explain why sleep time was comparable between current smokers and never smokers but significantly shorter in secondhand smokers. Occupational status may also be responsible for the high stress level observed in secondhand smokers. Stress level was not significantly different between current and never smokers. While there may be no association between smoking and stress level in these two groups, an alternative interpretation is also possible. Current smokers may have been under more stressful conditions that were relieved by smoking (or by the accompanied alcohol consumption). This speculation is supported by the fact that fewer current smokers sought for treatment for self-reported depression, despite a similar prevalence for depression between all three groups. A survey report from the American Psychological Association indicated a stress level of 4.8 in women in the general population. The stress level found in our study was slightly higher in all three groups (5.6, 5.9, and 5.6 in current, secondhand, and never smokers, respectively), likely reflecting the stressful environment infertile women face.
Exercise patterns were similar between groups, but current smokers did weight-training exercise more frequently than secondhand smokers or never smokers. However, the absolute frequency was less than once a week in all three groups, and thus the small difference may not have any clinical significance.
The prevalence of diabetes mellitus (4.0%) was significantly higher in current smokers than in secondhand smokers (0.0%) or never smokers (0.6%). This finding is consistent with the existing literature, as smoking is a well-known risk factor for diabetes mellitus (2122). Several cohort studies in Korea have also reported that smoking was associated with an increased risk for developing diabetes (2324); a 55% increase in the risk of diabetes was reported among men and women who smoked 20 cigarettes a day (24).
Infertile women are prone to emotional instability, and depression is one of the most important conditions possibly associated with infertility, although controversy exists (25262728). The prevalence of self-reported depression was 2.7%, and, according to the BDI inventory, mild-to-severe depression and moderate-to-severe depression were found in 32.9% and 10.7% of women, respectively. Although we did not directly compare the prevalence of depression between infertile and fertile women, the prevalence of depression observed in our study was higher than in previous reports. As many as 20%–50% of women undergoing IVF cycles were found to have mild-to-moderate symptoms associated with depression, and 2% had severe symptoms. Further, symptoms gradually worsened after failed cycles (29303132). Although we did not find a significant difference in the degree of depression based on smoking status in infertile women, we are the first to report the prevalence of depression in infertile women in Korea.
Among the 97.3% of women who had never been diagnosed with depression, moderate-to-severe depression assessed by the BDI which required professional counseling was as high as 10.7%. In addition, only 9.5% of patients with a previous depression diagnosis and 16.5% of women who experienced despair received treatment for those conditions. Infertility practitioners should be aware of the risk of depression in infertile women. Based on our findings, screening for depression and appropriate expert consultation is highly recommended in infertile women.
In the present study, there were no differences in menstrual characteristics or serum reproductive hormone levels based on smoking status. A close association between smoking and menstrual irregularity or serum TSH level has been reported in non-infertile women (1333435). The effect of smoking on serum prolactin level showed conflicting results in previous studies (363738). It must be emphasized that our study population included infertile women with a relatively low prevalence of smoking compared to western countries, and this might explain why smoking habits were not significantly associated with reproductive hormone levels; further research in this area is needed. Higher FSH, fewer antral follicle counts, and lower AMH values in smokers were reported in several studies. However, the influence of smoking on ovarian reserve is largely controversial (134353940).
Our study has several limitations. Questionnaire-based studies are intrinsically susceptible to recall bias, and intentional false responses may have been presented. Further, this was a cross-sectional study, and therefore did not allow for the establishment of causal relationships. Another limitation was subject heterogeneity, as participants were recruited at various stages of fertility treatments. Finally, information on follow-up treatments and pregnancy outcomes were not available.
In conclusion, higher probability of concurrent alcohol drinking, higher prevalence of diabetes mellitus, and lower education status were found in current smokers compared to never smokers. On the other hand, higher prevalence of primary infertility, higher proportion of employed women and lower education status were found in secondhand smokers compared to never smokers.
 XML Download
XML Download