

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Central precocious puberty (CPP) is defined as the early development of secondary sexual characteristics (before the ages of 8 years in girls and 9 years in boys) (12). Accurate diagnosis and treatment of CPP are essential because it is associated with compromised adult height as well as psychosocial and behavioral problems (34). The gonadotropin-releasing hormone stimulation test (GnRHST) has been used as the gold standard for diagnosing CPP, as it confirms the hormonal activation of the hypothalamic-pituitary-gonadal axis (567). The GnRHST could be inconvenient for both patients and clinicians because of repeated samples over 1 to 2 hours. Moreover, approximately 30% of individuals suspected with precocious puberty showed prepubertal response during the GnRHST (89). Therefore, it is important to accurately select patients who are expected to have a positive response during the GnRHST.
Skeletal maturity is assessed using bone age (BA), which is determined based on findings from the left hand and wrist radiographs (1011). BA is an essential part of the initial evaluation for pubertal disorders, as advanced BA is related to early exposure of sex hormones (12). Dental developments and maturity have been used to assess skeletal maturity after the development of a new dental age assessment by Demirjian et al. (13). In this context, dental maturity was assessed using morphological differences in the calcification stages of the mandibular canine, second premolar, second molar, or third molar (1415), and several studies have reported strong correlation between skeletal and dental maturity (161718). Dental maturity is affected by several diseases and conditions. Patients with juvenile rheumatoid arthritis showed advanced dental maturity (19). In contrast, dental development is retarded in patients with a constitutional delay in growth and puberty (20). However, only a few case studies have evaluated dental maturity in patients with precocious puberty (21).
The present study aimed to investigate the dental maturity of prepubertal girls and girls with CPP using data regarding the calcification stages of the mandibular second premolar and molar, to evaluate the usefulness of dental maturity as a screening test for CPP, and to identify anthropometric and laboratory factors affecting dental maturity and predictors of the pubertal response during the GnRHST.
MATERIALS AND METHODS
Participants
All girls who visited our pediatric endocrinology clinics between November 2013 and January 2015 were considered for participation in the study. Study participants were enrolled prospectively. A case-control study design was used.
The inclusion criteria were as follows: breast development of Tanner stage 2 or higher before 8 years of age, advanced BA (at least a 1-year difference between BA and chronological age [CA]), and have undergone the GnRHST between the ages 7.0 years and 8.9 years. Among them, participants with peak luteinizing hormone (LH) ≥ 5 IU/L and < 5 IU/L after the GnRHST were classified into the pubertal and prepubertal groups, respectively. The exclusion criteria were as follows: peripheral precocious puberty, precocious puberty caused by organic brain lesion, chronic endocrinologic disorders, oral or maxillofacial anomalies, orthodontic treatment, or permanent extraction of teeth.
The control group included girls aged 7.0–8.9 years without any secondary sexual characteristics. Subjects with basal LH ≥ 0.3 IU/L, BA advancement of ≥ 3 years (11), oral or maxillofacial anomalies, who had undergone orthodontic treatment, or who had had permanent teeth extracted, were not included in the control group.
A total of 114 subjects were screened. Of these, 11 controls were excluded because of basal LH ≥ 0.3 IU/L (3 subjects), BA advancement of ≥ 3 years (4 subjects), and orthodontic treatment (4 subjects). Thus a total of 103 subjects were included in the study.
Methods
From all study participants, clinical data, such CA, BA, height, weight and body mass index (BMI) were collected. Height and BMI were expressed as the standard deviation score (SDS), based on the 2007 Korean National Growth Charts (22). In the pubertal and prepubertal groups, laboratory data were obtained during the GnRHST. In the control group, fasting serum samples were used to measure the levels of LH, follicular stimulating hormone (FSH), estradiol, dehydroepiandrosterone sulfate (DHEA-S), insulin-like growth factor-I (IGF-I), the IGF binding protein-3 (IGFBP-3), and 25-hydroxyvitamin D3 (25[OH]D3).
The GnRHST was conducted during the morning after an overnight fasting. Intravenous injection of 100 μg of GnRH (Relefact; Sanofi-Aventis, Frankfurt, Germany) was administered after obtaining basal serum samples. Blood samples were also collected at 30, 45, 60, and 90 minutes after GnRH administration. BA was evaluated by a single pediatric endocrinologist (JHK) using the Tanner-Whitehouse 3 methods (11).
Panoramic radiographs were obtained for all participants. Dental maturity was assessed according to the tooth calcification stages developed by Demirjian et al. (13). The characteristics of each stages according to Demirjian index (DI) (Fig. 1) were as follows (23): (A) Calcification of the occlusal points without fusion can be observed; (B) Fusion of the calcified points forms the occlusal surface; (C) Enamel formation at the occlusal surface is complete, dentin formation is observed, the pulp chamber has a curved shape, and no pulp horns are visible; (D) Crown formation is complete to the level of cemento-enamel junction, root formation is observed, the pulp horns are visible, and the walls of the pulp chamber are curved to the cervical region; (E) The walls of the pulp chamber are straight, the root length is less than the crown height, and radicular bifurcation is observed in the molar; (F) The walls of the pulp chamber form an isosceles triangle and the apex ends in a funnel shape, the root length is equal to or longer than the crown height, bifurcation has developed to give the roots a more definite form; (G) The walls of the root canal are parallel and its apical end is partially open; and (H) The apical end of the root canal is complete and the periodontal membrane is distinct. A dental radiologist (JWC) interpreted the panoramic radiographs of the mandibular second premolar and molar as one of 8 stages (A to H). The higher DI was assigned when a discrepancy between the left and right teeth was observed. Most participants exhibited nearly identical DI values for the right and left sides. To validate the reproducibility of the dental maturity index, the DI values were re-evaluated by the same dental radiologist (JWC) in 20 randomly selected subjects at 2 weeks after the initial evaluation.
 | Fig. 1Schematic illustration of the DI for dental maturity (13).
DI = Demirjian index.
|
Statistical analysis
Statistical analyses were performed using the Stata software (version 14.1; StataCorp LP, College Station, TX, USA). Kruskal-Wallis analysis was applied to continuous variables among the pubertal, prepubertal, and control groups. Post-hoc analysis was performed using the Mann-Whitney U test with a correction of type 1 error by Bonferroni's method. Categorical variables were compared using the χ2 test and P for trend. Logistic regression analysis was performed to identify factors predicting positive GnRHST results. The kappa statistics was applied for intra-observer agreement of DI. Data are expressed as median (interquartile range) or as odds ratios (ORs) and 95% confidence intervals (CIs). P values < 0.05 were considered statistically significant.
RESULTS
Clinical characteristics of study participants
A total of 103 participants (pubertal, 40; prepubertal, 19; and control, 44) were enrolled in the study. CA was not significantly different among the 3 groups. BA and the difference between BA and CA were significantly lower in the control group compared to other groups (P < 0.001; Table 1). No significant differences were observed in the anthropometric measurements, including height SDS, BMI SDS, and waist-to-height ratio (WHR) among groups.
Table 1
Clinical characteristics of enrolled subjects at baseline
Values are presented as median (interquartile range); Data were analyzed using the Kruskal-Wallis test. The post-hoc analysis was performed using the Mann-Whitney U test with Bonferroni's method. Peak LH and FSH levels were analyzed using the Mann-Whitney U test.
CA = chronological age, BA = bone age, SDS = standard deviation score, BMI = body mass index, LH = luteinizing hormone, FSH = follicular stimulating hormone, DHEA-S = dehydroepiandrosterone sulphate, IGF-I = insulin-like growth factor-I, IGFBP-3 = insulin-like growth factor binding protein-3, DI = Demirjian index.
*,†,‡Superscripts indicate significant differences between values with the same marks.
![]()
Basal LH and FSH concentrations were significantly high in the pubertal group. Basal estradiol level was significantly different between the pubertal and control groups. In participants who underwent the GnRHST, peak LH and FSH levels were high in the pubertal group (P < 0.001). The 25(OH)D3 concentrations were observed to be the highest in the control group (P < 0.001); however, there were no differences between the pubertal and prepubertal groups. IGF-I concentrations were the highest in the pubertal group and the lowest in the control group (P < 0.001), but the IGFBP-3 levels were not different among groups (P = 0.830).
Dental development of study participants
The reproducibility of the DI was almost perfect (24). The kappa coefficient for intra-observer agreement was 0.854 for the second mandibular premolar and 0.811 for the second mandibular molar.
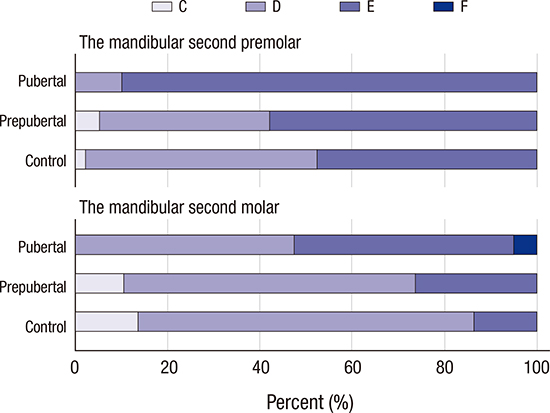
The DI of the mandibular second premolar and molar was distributed from stage C to F (Table 1, Fig. 2). The distribution of the maturation stage of the mandibular second premolar and molar was significantly different among groups (P = 0.001 and P = 0.038, respectively); a higher DI was observed in the pubertal group (Table 1).
 | Fig. 2Distributions of DIs among the participants according to teeth and groups.
DI = Demirjian index.
|
CA, BA, BA advancement, height SDS, peak LH after the GnRHST, and IGF-I were associated with an increased DI in both the mandibular second premolar and molar (Table 2, Fig. 3). BMI SDS and overweight and obesity were associated with a DI value of ≥ E for the mandibular second premolar. The basal FSH level was associated with an increased DI for the mandibular second molar.
Table 2
Factors affecting dental maturity of the mandibular second premolar and molar (a DI value of ≥ E)
DI = Demirjian index, OR = odds ratio, CI = confidence interval, CA = chronological age, BA = bone age, SDS = standard deviation score, BMI = body mass index, LH = luteinizing hormone, FSH = follicular stimulating hormone, IGF-I = insulin-like growth factor-I.
![]()

Logistic regression analysis for determining predictors of pubertal response in the GnRHST
The control group was considered as the prepubertal group with a prepubertal response in the GnRHST when logistic regression analysis was performed. CA, BA, difference between BA and CA, and levels of basal LH, basal FSH, basal estradiol, 25(OH)D3, and IGF-I were predictors associated with positive GnRHST results (data not shown). A DI value of ≥ E for both the mandibular second premolar and molar was a significant predictor of pubertal response in the GnRHST. The OR of the second premolar and molar was 8.7 (95% CI, 2.9–26.1) and 5.2 (95% CI, 2.2–12.7), respectively (Table 3). The sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) for predicting a positive response in the GnRHST for a DI value of ≥ E were 90.0%, 49.2%, 52.9%, and 88.6%, respectively for the mandibular second premolar and 52.5%, 82.5%, 65.6%, and 73.2%, respectively, for the mandibular second molar (Table 3).
Table 3
Diagnostic performance of the dental maturity at the mandibular second premolar and molar according to DI for the GnRHST result

DI = Demirjian index, GnRHST = gonadotropin-releasing hormone stimulation test, OR = odds ratio, CI = confidence interval, PPV = positive predictive value, NPV = negative predictive value.
![]()
DISCUSSION
In the present study, we observed that dental maturity, as assessed by the DI, was a useful marker for predicting a positive response in the GnRHST. A DI value of ≥ E for the mandibular second premolar and molar was a significant predictor of a positive response in the GnRHST in girls suspected to have CPP in this study. The OR of the mandibular second premolar and molar (a DI value of ≥ E) was 8.7 (95% CI, 2.9–26.1) and 5.2 (95% CI, 2.2–12.7), respectively. The mandibular second premolar with a DI value of ≥ E had a sensitivity of 90.0%. The mandibular second molar with a DI value of ≥ E showed a specificity of 82.5%. Dental development of both teeth was a useful indicator for diagnosing CPP. Moreover, a DI value of ≤ C for the mandibular second premolar and molar showed an NPV of 100.0% for the positive response of GnRHST. A DI value of ≥ F for the mandibular second molar showed a PPV of 100% for the pubertal response in the GnRHST.
In the clinical setting, dental maturity might be a useful screening tool when the decision regarding whether to perform the GnRHST confirmatory test for CPP is equivocal, based on the patient's clinical presentation and given that GnRHST is a time-consuming procedure requiring repeated samples. Dentists could relatively easily refer girls with advanced DI and pubertal signs to a pediatrician for further evaluation.
Previous researchers have reported that dental maturity is associated with CA and BA (16171825). In this study, we revealed that a higher DI value was associated with higher CA, BA, and difference between BA and CA. Costacurta et al. (26) reported that dental development was related to body adiposity among children. Obese children with higher body fat showed accelerated skeletal-dental age. In this study, BMI SDS, abdominal obesity, and WHR showed a positive association with higher DI values of the mandibular second premolar.
In the present study, dental maturity was assessed using the DI because it is reported as a reliable indicator of skeletal maturity (1827). Moreover, using the DI is advantageous because the maturation stage can be classified based on the crown-to-root ratio of the tooth rather than the absolute length; furthermore, magnification errors related to panoramic radiographs can be eliminated. In this study, a DI value of ≥ E indicated a high predictive value for diagnosing CPP. In panoramic radiographs, it is not difficult to distinguish between DI stages of D and E because the existence of a straight pulpal wall and bifurcation in the second molar is a distinct feature of stage E (13).
In panoramic radiographs, there is a superimposition of the palatal root and anatomic structures (e.g., the palate, zygomatic arch, or the inferior nasal concha), which makes it difficult to observe the roots. Thus, previous researchers generally evaluated dental maturity of the mandibular canine, second molar, or third molars (151618). However, we used the mandibular second premolar and molar for evaluating dental maturity in this study. The reasons for this were as follows: 1) roots of the mandibular anterior tooth intermittently overlapped with the ghost image of the cervical vertebrae on the panoramic radiographs; 2) the third molars are commonly missing in humans; and 3) the third molars cannot be clearly visualized in children who are less than 7 or 8 years old.
Panoramic radiographs visualize both jaws and their dentition continuously by a rapid, simple, and convenient procedure. Owing to these advantages, panoramic radiography has been widely used in screening for dental disorders and epidemiologic studies (28). Compared to the GnRHST, dental maturity can be examined easily during routine dental examination with panoramic radiography. The effective dose for panoramic radiography was reported to range from 14 to 24 μSv, which is equivalent of 2 to 3 days of additional background radiation exposure (2930).
According to previous studies, the predictors of a positive GnRHST were basal LH levels, basal FSH levels, previous height velocity, 25(OH)D3 levels, BA, BA advancement, and IGF-I levels (8931). Houk et al. (32) suggested that the unstimulated LH level using the third generation assay was adequate for diagnosing CPP in most cases. Nam et al. (9) reported that rapid growth velocity with a cut-off value of 3.8 cm over 6 months was a useful marker for predicting CPP in participants who have undergone the GnRHST. Lee et al. (31) showed the possibility of an association between CPP and lower 25(OH)D3 concentrations. Similarly, in the present study, the positive GnRHST response was associated with BA, the difference between BA and CA, and levels of basal LH, basal FSH, basal estradiol, 25(OH)D3, and IGF-I.
This study has several limitations. First, the number of enrolled participants was insufficient. Second, this study was performed only in girls because cases of CPP were relatively rare among boys. Third, the DI value determined based on panoramic radiograph findings might vary depending on the dental radiologists. Fourth, dental maturity might also be affected by other genetic, ethnic, nutritional, and environmental factors, which were not analyzed in this study (3334). However, to the best of our knowledge, this is the first study to use an age-matched control group to validate the usefulness of dental maturity for predicting a diagnosis of CPP.
In conclusion, dental maturity assessed using the DI is a strong predictor for diagnosing CPP using the GnRHST. The OR of the mandibular second premolar and molar (a DI value of ≥ E) is 8.7 and 5.2, respectively. Furthermore, dental maturity is associated with BA, CA, BA advancement, and obesity. Therefore, evaluating dental maturity in girls who are suspected of having precocious puberty may help determine whether they should undergo the GnRHST.
 XML Download
XML Download