

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
In-hospital death following intensive care unit (ICU) stay is estimated to be 5%–27% in various reports (12345). Despite improvements in ICU care quality and widespread utilization of step-down units over the last decades, a significant number of patients still die in the hospital following successful ICU discharge.
The short-term prognosis after intensive care can be determined by factors both within and outside the ICU (67891011). Several studies have shown that illness severity and high nursing workload required at the time of ICU discharge are associated with poor outcomes (3). On the other hand, others have focused on factors in the wards after ICU care and emphasized the role of special “watchdog” teams to identify those patients at risk of death (12). While intensivists work rigorously to reduce deaths after ICU care, some deaths seem inevitable or sometimes unpredictable.
In this study, we first investigated the causes of in-hospital deaths following successful ICU discharge; we were also interested in assessing the proportion of unexpected deaths on the wards. Second, we analyzed the data to discover the predictors of in-hospital mortality.
MATERIALS AND METHODS
Study design and subjects
We performed a retrospective, single-center cohort study using medical intensive care unit (MICU) registry data. This included all MICU admissions to the Seoul National University Bundang Hospital (a tertiary care university-based teaching hospital with MICU size of 16 beds of 1,356 hospital beds) from January 2011 to August 2013. Of 723 identified admissions, 383 patients who were discharged alive from their first ICU admission with at least 24 hours of ICU length of stay (LOS) were included (Fig. 1). Patients aged less than 18 years, who died in the ICU upon the first ICU admission, and who were discharged to surgical ICUs and ICUs at other hospitals were excluded from the analysis, as well as those with terminal discharges to the wards for hospice care. For patients with multiple ICU admissions during the same hospital stay, only the result from the first MICU admission was considered.

Variables
Demographic data including age, gender, body mass index (BMI), and body weight just before admission and upon discharge from ICU was recorded. Comorbidities diagnosed only before admission were considered. Illness severity scores (Acute Physiologic and Chronic Health Evaluation II; APACHE-II) and Sequential Organ Failure Assessment (SOFA) scores were calculated at ICU admission. Vital signs and laboratory findings upon ICU admission and discharge were also recorded: white blood cells (WBCs), hemoglobin (Hb) levels, platelet counts (Plt), absolute neutrophil count, arterial blood gas analysis, albumin (Alb), total cholesterol levels, prothrombin time, total bilirubin (Tbil) levels, serum creatinine, blood urea nitrogen (BUN), lactic acid, and C-reactive protein (CRP).
In order to determine reasons for in-hospital deaths, a single physician reviewed the entire hospital records of all non-survivors (n = 45), including MICU discharge summaries, ward notes, nurse records, and death certificates. We also recorded whether the patient and the family had documented do-not-resuscitate (DNR) orders or decisions to withhold futile treatments before death. Considering the purpose of our study, patients with documented DNR status before ICU admission or during ICU stay were excluded from the analysis, as shown in Fig. 1. Accordingly, patients with documented DNR status admitted in wards after successful ICU discharge were included in the analysis.
Statistical analyses
The patients' clinical variables were analyzed using descriptive statistics expressed as means with ranges or as percentages. Values were compared between survivors and non-survivors after ICU discharge. Differences in continuous variables were compared with Mann-Whitney U tests for non-normal distributions and independent t tests for normal distributions. Dichotomous variables were assessed with Pearson χ2 tests and Fisher's exact tests where applicable.
Univariate logistic regression analysis was conducted to identify possible predictors of in-hospital mortality after ICU discharge. Any variable with P value < 0.050 from the univariate analysis was considered as candidates for inclusion in the multivariate logistic regression analysis. In the final model, we first included a specific variable, SOFA score upon ICU admission (SOFAadm), because it had the smallest value of Akaike's information criteria (AIC) and was clinically relevant as well. Afterwards, we included significant variables from the univariate analysis (P < 0.050) and selected those with incremental effects on SOFAadm (e.g., time from ER to ICU admission; presence of solid cancer, ACS, and hematologic disease; and blood levels of Hb, Tbil, and BUN upon ICU admission). Then, with backward selection (P < 0.100), we selected SOFAadm, Hb upon ICU admission, and the presence of solid cancer and hematologic disease. Considering its clinical significance, we also added the Plt level to the final model of multivariate logistic regression. The variables were previously tested for interaction and none of them showed significant interaction with others. Calibration of the model was evaluated with the Hosmer-Lemeshow goodness-of-fit test. Two tailed P values less than 0.05 were considered statistically significant. The statistical tests were performed using Statistical Package for the Social Sciences (SPSS) version 17.0 (SPSS corp., Chicago, IL, USA).
Ethics statement
The present study protocol was reviewed and approved by the Institutional Review Board of Seoul National University Bundang Hospital (IRB No. B-1408-262-114). We were given an exemption from informed consent of participants due to the characteristics of our study as a retrospective observational study.
RESULTS
Of 383 patients who survived MICU care, in-hospital deaths occurred in 45 patients (11.7%). As primary causes of ICU admission, the most frequent cause was respiratory failure followed by sepsis in both non-survivors and survivors (Table 1).
Table 1
Causes of initial ICU admission in survivors and non-survivors

ICU = intensive care unit, CAP = community-acquired pneumonia, HAP = hospital-acquired pneumonia, VAP = ventilator-associated pneumonia, CRRT = continuous renal replacement therapy, GI = gastrointestinal.
*If there were multiple primary causes for ICU admission, we permitted up to 3 causes for admission to the unit.
Indeed, the most common cause of mortality after ICU discharge was also respiratory failure (56%, 25/45) followed by sepsis (18%, 8/45), cancer progression (16%, 7/45), cardiopulmonary arrest of unknown cause (11%, 5/45), and cerebrovascular disease (11%, 5/45). The reasons for in-hospital death and ICU admission were the same in more than half of all deaths (64%, 29/45). Sudden unexpected deaths comprised about one-fifth of all deaths (18%, 8/45).
Table 2 shows demographic and clinical characteristics upon MICU admission. Non-survivors had higher prevalence of comorbidities such as chronic kidney disease, solid cancer, and hematologic disease and were more likely to be admitted from the wards. Hospital LOS before ICU admission was significantly longer in non-survivors. A similar result was shown for duration of emergency department (ED) stay until ICU admission. Severity scores including APACHE-II and SOFA were also higher in non-survivors. Duration of mechanical ventilation (MV) was longer in non-survivors than in survivors (Tables 2 and 3).
Table 2
Characteristics of patients upon ICU admission

Values are presented as number of patients (%) or mean ± standard deviation.
ICU = intensive care unit, NED = no evidence of disease, ED = emergency department, CPR = cardiopulmonary resuscitation, LOS = length of stay, APACHE-II = Acute Physiology and Chronic Health Evaluation II, SOFA = Sequential Organ Failure Assessment, Hb = hemoglobin, Alb = albumin.
*Night-time admission is defined as admission to the unit during 19:01–06:59.
Table 3
Clinical features during ICU stay and at the time of ICU discharge

ICU = Intensive care unit, LOS = length of stay, CRRT = continuous renal replacement therapy, MV = mechanical ventilation, NIPPV = nasal intermittent positive pressure ventilation, SBP = systolic blood pressure, DBP = diastolic blood pressure, HR = heart rate, RR = respiratory rate, BT = body temperature, GCS = Glasgow Coma Scale, WBC = white blood cell, Hb = hemoglobin, Plt = platelet counts, INR = international normalized ratio, Tbil = total bilirubin, Alb = albumin, BUN = blood urea nitrogen, CRP = C-reactive protein, SOFA = Sequential Organ Failure Assessment.
*A night-time discharge is defined as discharge from the unit during 19:01–06:59.
When comparing laboratory values, Hb, and Alb were initially higher in survivors at ICU admission (Table 2). Upon MICU discharge, non-survivors had decreased Hb, Plt, and Alb and elevated Tbil and BUN (Table 3).
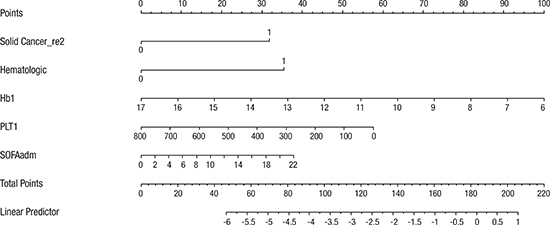
The results of univariate analysis are shown at the Supplementary Table 1. With the described methods, we selected the final model of multivariate logistic regression analysis (Table 4), which included SOFAadm, presence of solid tumor, hematologic disease, and Hb and Plt count upon ICU discharge. Based on the logistic regression model, we constructed a nomogram to predict post-ICU mortality (Supplementary Fig. 1). The calibration plot of model-development showed that the nomogram was well fitted (Hosmer-Lemeshow test: χ2 = 7.670, P = 0.470, area under the curve [AUC] = 0.785, Supplementary Fig. 2).
DISCUSSION
In this retrospective review of 383 patients discharged from the MICU over 3 years, we found that the post-ICU mortality in our hospital remains an important problem. Compared with the mortality rate of 5% obtained in a recent multicenter study in Australia and New Zealand by Santamaria et al. (13) and the post-ICU mortality rate of 10% in the European Sepsis Group by Azoulay et al. (14), our result of an in-hospital mortality rate of 11.7% after ICU discharge was much worse (n = 45/383). This difference can mainly be attributed to the exclusion of patients in surgical ICUs, resulting in a relatively severe disease severity in our study; differences in ICU capacity and subtle management skills may also have contributed to this difference (15). The most common cause for in-hospital mortality after MICU discharge was respiratory failure followed by sepsis, which is consistent with other studies (16). Extended duration of MV was seen in non-survivors, which may provide one explanation for respiratory complications after intensive care (17).
Most patients had the same reason for post-ICU death and initial ICU admission, which implies that the main problem was not completely solved during their ICU stay. Several attempts have been made to explain this finding in previous studies (69). For example, premature discharge from the MICU due to high demands and shortage of ICU beds may have resulted in poor prognosis in those patients. While it can be attributed to problems in allocation of resources to some extent, we are yet unsure that deferring ICU discharge would result in better patient survival. In spite of utilization of multiple step-down units, a significant number of patients still die in the wards after successful ICU discharge. Unexpected death accounted for one-fifth of all deaths (n = 8) including unknown cardiopulmonary arrest (n = 5).
Independent predictors for hospital mortality after ICU discharge included low levels of Hb and Plt upon ICU discharge. While there still remains controversy regarding the optimal target level of Hb in ICU patients and about the role of transfusion (18), our result shows that there is a close relationship between Hb and prognosis after ICU discharge. Recent studies including a prospective cohort study in Korea also suggested the role of Plt counts in predicting mortality in critically ill patients (1920). In accordance with the literature, our result demonstrates that thrombocytopenia is associated with increased in-hospital mortality even after critical illness. Possible explanation includes that Plt reflects the degree of catecholamine surge, inflammatory response, sepsis, and disseminated intravascular coagulopathy (212223). If Hb and Plt count did not improve to an optimal level at the time of ICU discharge, it may indicate that the patient could not fully recover from the critical condition and may deteriorate after ICU discharge.
The authors acknowledge that this study has several limitations. First, it was conducted in an MICU of a single center university-based tertiary hospital, so the result may not be applicable to patients in surgical ICUs or in different hospital settings with different patient characteristics. For example, 28 out of 45 deaths (62%) in our study occurred in patients with solid cancer, hematologic malignancy, or immunocompromised status. This may suggest that a significant proportion of cancer patients with poor prognosis comprised our study population, whose high mortality seems to be expected. However, it may also reflect the current patient composition in tertiary centers in Korea, with a shift towards chronic, severe underlying medical disorders, especially malignancy. Second, all patients were from Asia and did not include other ethnic groups. Third, our study size was small with 45 deaths in the hospital after ICU discharge. However, previous studies have shown similar numbers of participants. Indeed, our results were robust in terms of the statistical analysis, and despite the size, we think that some important clinical implications can be drawn from our results. Fourth, we did not substantiate our results using a validation cohort, which can be sought in the future.
One of several strong points of this study is that in-hospital mortality was assessed for all patients admitted to the medical ICU. We did not sub-group patients with MV only as it was done in most of the other studies. Therefore, our result can be more applicable to a general population of medical patients in the medical ICU setting. Second, we do have survival data of all patients included in the study, which we obtained from the national death records. Nevertheless, the result drawn from a multiple regression model using the survival data was not different from the one shown here.
In conclusion, more than half of the patients died of the same reason that prompted their admission to the MICU; the causes of only one-fifth of in-hospital deaths after ICU discharge were unpredictable. Patients who die in the hospital after successful MICU discharge tend to have higher severity scores upon admission, with comorbidities of hematologic disease and solid tumor, and relatively anemic and thrombocytopenic statuses upon ICU discharge. Further studies are warranted in the future to reflect changes and updates in hospital environments and ultimately to reduce reversible portions of hospital mortality after ICU discharge.
 XML Download
XML Download