

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
On April 25, 2015, a 7.9 magnitude earthquake occurred in Nepal. Eighty-seven rescue teams from all over the world were dispatched to the disaster site (1). The Korean Disaster Relief Team (KDRT) established a base of operation (BoO) in Bhaktapur, Nepal to provide foreign medical team (FMT) type 2 medical services for 15 days. During this period, part of the team returned to Korea, and the remaining 6 members experienced a 7.3 magnitude aftershock, which occurred in Dolakha, Nepal, on May 12. Because it is rare for disaster relief team members to be exposed to a massive aftershock, we conducted this study to evaluate the stress of relief work and the prevalence of post-traumatic stress disorder (PTSD) among relief workers.
Berger et al. (2) defined a rescue worker as any person who professionally or voluntarily engages in activities devoted to providing out-of-hospital acute medical care, transporting individuals to definitive care, or freeing persons or animals from danger to life or well-being in accidents, fires, bombings, floods, earthquakes, other disasters, and life-threatening conditions. Due to the nature of the job, relief teams tend to be exposed to various physical and mental hazards. Yet, studies regarding stress and PTSD in relief teams have been relatively rare compared with those about primary disaster victims. The prevalence of PTSD in relief teams varies across studies. According to a meta-analysis conducted by Berger et al. (2), the prevalence was about 10%, which was higher than that in the general population, 1.3%–3.5%, and lower than that in primary victims, 19%–39%. Furthermore, Shin et al. (3) indicated that, PTSD prevalence in firefighters was 15.1% and that higher risk was associated with frequent traumatic experiences and being in the emergency medical service department. In addition to PTSD, relief teams have been found to suffer from comorbid psychological conditions (e.g., depression or panic disorder) (4), to visit hospitals more frequently with physical symptoms, and to report a decreased quality of life due to heavier non-prescription drug or sleeping pill use (5). For the reasons mentioned above, relief teams' need for psychological treatment, varying from simple counseling to medical intervention, is high. However, the psychological counseling services and surveillance programs available to relief teams are inadequate (6).
Some studies show that disaster relief work has a positive effect on the mental health of rescue workers. Areas of reported post-traumatic growth have included relationships with others, self-perceptions, appreciation of life, and spirituality. These post-traumatic growth factors had a positive, albeit weak, correlation with post-traumatic stress symptoms (78).
We conducted in-depth interviews with KDRT members about their experience in Nepal to evaluate stressors, positive effects, and motivation to engage in disaster relief work to develop approaches to the treatment of disaster relief workers in the future.
MATERIALS AND METHODS
Subjects
The sample for this study consisted of 11 KDRT members of the Nepal disaster relief team working at the National Medical Center. Six of the subjects experienced the massive aftershock on May 12. Participants provided signed informed consent forms, and all agreed to participate in the study.
Of the total of 11 subjects, 6 were male, and the mean age was 35.5 years. In terms of occupation, there were 4 doctors, 3 nurses, 2 office clerks, 1 emergency medical technician, and 1 pharmacist. The mean time subjects were KDRT members was 2.5 years, and 7 people had prior experience with overseas relief work. The mean time of arrival of subjects after the earthquake was 5.6 days, and the mean time spent in Nepal was 12.9 days. Six people experienced the aftershock on May 12 (Table 1).
Table 1
Demographics of the subjects

Interviews
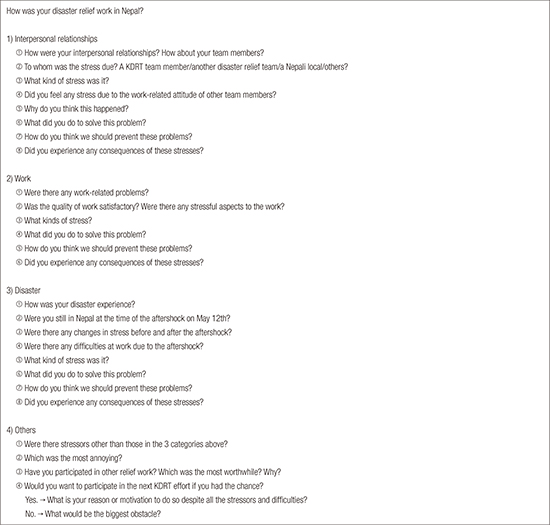
Individual in-depth interviews with 11 subjects were conducted by 1 researcher. The researcher conducted the interviews based on a questionnaire containing open-ended questions (Appendix 1) that were developed during research meetings and reviewed by an auditor. Questions addressed the stressors encountered during the relief work, the aftermath, and the motivation for joining the efforts. The interview was recorded with consent from participants.
Data analysis
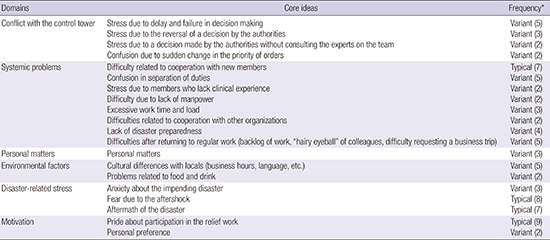
Following the Consensual Qualitative Research (CQR) method (9), each researcher developed domains and core ideas from the first several interview transcripts. Domains are topics used to group or cluster data, and core ideas are summaries of the data used to abstract the interview data within domains. These domains and core ideas were reviewed, followed by the consensus process, at a research meeting and then reviewed again by an auditor. Refer to Table 2 for the full list of domains and core ideas of our study. The remaining interview transcripts were then coded into domains and core ideas by 2 different researchers, who cross-analyzed the data process. The core ideas within the domains were reviewed several times until a consensus between researchers was achieved. After the cross-analysis process was reviewed by the auditor, core ideas were categorized using frequency labels: “general” was applied to ideas mentioned by 10–11 of the 11 respondents, “typical” was applied to ideas mentioned by 6–9 (i.e., at least 50% but less than 90%), “variant” was applied to ideas mentioned by 2–5 (i.e., at least 20% but less than 50%), and findings applying to single cases were placed in a miscellaneous category and not included in the results (Fig. 1).
Table 2
Results of the questionnaire


RESULTS
Data analysis yielded 6 domains: 1) conflict with the control tower, 2) systemic problems, 3) personal issues, 4) environmental factors, 5) disaster-related stress, and 6) motivation. See Table 2 for a complete list of domains, categories, and frequencies.
Conflict with the control tower
This domain included stressors due to conflict between the domestic authorities and the KDRT. Stressors in this domain were divided into 4 categories: stress due to delay and failure in decision making, stress due to authorities reversing a decision, confusion due to a sudden change in the priority of orders, and stress due to authorities making a decision without consulting experts in the team.
Stress due to delay and failure in decision making was the most commonly mentioned item in this domain (n = 5). They stated, “Because we went to the disaster site later than other relief teams, we wondered whether this dispatch was too late. And because many of the patients were chronic patients, we were skeptical about whether we had given help to the really needy and thought: ‘Shouldn't we have gone to some place nearer to the disaster site?’” Many of them felt disappointed about having to see chronic patients due to a delay in decision making when their expectation was to offer help to acute patients.
Stress arising from authorities reversing a decision was reported by 3 members, and one stated, “We would rather like to get a definite order from the control tower, but since we didn't get one, we were all confused about what to do.” They complained about difficulties created by the control tower by reversing orders related to the work and about stress due to disagreements between the authorities themselves. Confusion due to a sudden change in the priority of orders was reported by 2 of the team members who had to contact the authorities most frequently. The team leader reported, “The biggest problem was that the whole system was shook up because the control tower was changed all of a sudden. So the priority of orders had also changed.” They complained that it was hard to follow an entirely new work system. Two people also reported stress due to authorities making a decision without consulting the experts in the team. One of the respondent, a member of the advance party, said, “It's not a communication problem, but the problem is that the decision is not mine.” They also said that the authorities gave orders that were inappropriate for relief work.
Systemic problems
This domain was divided into the most diverse categories, and it addressed difficulties concerning the systemic problems of the relief work and general support for the relief work. The first category concerned stress due to relationships between the KDRT members, the second related to stress due to overwork, and the last addressed stress due to lack of support for relief work.
Stress due to relationships between the KDRT members included difficulties related to cooperation with new members, which was typically reported by 6 members, the most common core idea except disaster-related stress. One member stated, “There should be some kind of an orientation or something. Putting people who had never met together and telling them ‘You're a team from now on, so work together isn't sufficient. Should I say that we didn't feel any sense of belonging?” Many reported finding it difficult to cooperate with members of other organizations with no prior orientation. Stress due to confusion regarding the division of duties and members who lacked clinical experience was also reported by 5 and 2 members, respectively.
Stress due to overwork included difficulty related to lack of manpower and excessive work time and load, which were reported by 2 and 3 members, respectively. Most members agreed, “The meetings should be shorter and more concise. And we would appreciate more sleep.” They said that the medical service itself was appropriate, but the extra work, such as meetings or other logistical responsibilities, was too much.
Concerning the lack of support for the KDRT work, there were stresses related to cooperating with other organizations, lack of disaster preparedness, and difficulties after returning to regular work; these were reported by 2, 4, and 5 members, respectively. They said that cooperation among other organizations, including with regard logistics and other aspects, is necessary and that prior education about coping with disasters is also needed. Most of all, they said that it is hard to engage in the KDRT work because of the lack of consideration accorded to their original work situation, including their backlog of work, the weariness of their colleagues, and the difficulty of requesting a business trip to perform relief work. One said, “Even though I'm using my holiday to participate in this KDRT work, I get hairy eyeballs from my colleagues and have to return to work after 1 day of rest. In this condition, I don't think I can volunteer for the KDRT relief work next time.”
With the exception of stress due to difficulty related to cooperation with new members, every core idea in this domain was labeled as variant.
Personal matters
Variant core ideas, ranging from personal dislike of to personal conflict with others, were reported by 4 members in this domain.
Environmental factors
Problems due to environmental factors were addressed in this domain. Stress due to cultural differences and problems related to food and beverages were variantly reported by 5 and 2 people, respectively. Difficulties with communication and differences in usual business hours and medical systems were included in the area of cultural differences. For example, one member stated, “It's like we opened at about 8 a.m., but the locals usually started moving at about 10 a.m.”
Disaster-related stress
Stressors related to disaster, including the aftershock, were addressed in this domain. Core ideas were divided into anxiety about the impending disaster, frightening experiences due to the aftershock, and consequences of the disaster.
Three members reported anxiety about the impending disaster, saying that they felt insecure during the relief work due to this anxiety. Eight members, including 2 members who only experienced minor aftershocks, reported stress due to a fearful aftershock experience, saying that it was a horrible experience that felt unreal. One member described the experience as follows: “The concrete floor was swaying like a wave, the wreckage of the building was falling, and people were running this way and that. It was like starring in a disaster film, and the shock was too much; I felt sad, stunned, and depressed all at the same time.” Seven members reported consequences of the disaster, and one said, “My heart races when I feel a wave from a passing dump truck or bus, and I feel unsafe when staying inside a building. I think this will remain a trauma to me.”
The first core idea was categorized as variant, whereas the second and third were categorized as typical. However, only 6 subjects were in Nepal at the time of the aftershock. Thus, by limiting subjects to members who had experienced the aftershock, we were able to classify the second and third core ideas as general, as all 6 responded in this way.
Motivation
The last domain concerned motivation to engage in relief work, and typically 9 of the subjects suggested that pride led them to participate in this work. One member stated, “I feel it is worthwhile to help other people in need, and this feeling is still larger than the stress of this work. So, I'd like to participate in the future if I have a chance.” Variantly, 2 members said that their participation reflected only a personal preference.
Summary
In summary, none of the stressors related to relief work met criteria for classification in the general category, and the typical category included difficulty related to cooperation with new members, having a frightening experience, and consequences of the aftershock. However, stress related to having a frightening experience and consequences of the aftershock qualified as general when we limited subjects to individuals who had experienced the aftershock. Many other stress-related factors were placed in the variant category. The pride of being on the team was the most common motivation for relief work, as it was typically chosen by nine subjects. Only personal preference was coded as a variant opinion.
DISCUSSION
Most subjects felt stressed by the disaster experience and its aftermath. However, surprisingly, stresses arising from systemic problems were also commonly mentioned, with stress associated with difficulty related to cooperation with new members the most common. There have been several studies reporting results consistent with ours. According to Armstrong et al. (10), stressors other than trauma exposure, such as longer work hours, cooperation with other organizations, and conflict between colleagues, can cause confusion, stress, or fatigue in rescue workers. According to Marmar et al. (11), other than peritraumatic stress, greater stress from routine work was also associated with PTSD symptoms.
Meanwhile, lack of disaster preparedness was also mentioned as a variant stressor. Specialized training and preparedness has been associated with a lower level of stress (1213), but the benefit of previous disaster-related experience is controversial. Some studies found previous experience had an immunizing effect (1415), but others found no significant differences (1617), and one found prior experience was associated with greater distress (18). Accordingly, it is necessary for relief workers to undergo training about safety and disaster damage prevention before dispatch and to be screened for distress due to prior experiences.
Stress due to systemic problems can be prevented by improving the system, and it thus differs from disaster-related stress, which is not fully preventable. For this reason, we must focus on and discuss ways to improve our systems. The stress experienced by rescue workers should be addressed immediately, and there are various ways to do this. In some organizations, staff is expected to seek help from direct superiors; in another, peer support groups are used; and, in another, respected peers have been trained as counselors (19).
As mentioned above, the PTSD risk of rescue workers is higher than that of the general population (23), and other comorbid mental disorders are common in this population. Rescue workers are occupationally exposed to psychological trauma, and even ‘repeated/extreme indirect exposure in the course of a professional job’ is defined as a cause of PTSD in the revised fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-V) (20). According to Stellman et al. (4), 11.1% of rescue workers met the criteria for probable PTSD; however, 8.8% also met the criteria for depression, and 5.0% also met the criteria for panic disorder. Nearly half (45%) fulfilled Schuster's criteria for a substantial stress reaction. About 24% of alcohol users reported drinking more than usual following 9/11, and about 47% reported that they drank more during the time they were working at the World Trade Center (WTC) in rescue and recovery operations. According to long-term follow-up studies, the prevalence of PTSD increases over time. One study concerning the WTC disaster showed that 9.8% of firefighters exposed to the disaster met the criteria for an elevated risk of PTSD in the first year. Subsequently, 9.9%, 11.7%, and 10.6% of firefighters met the criteria at 2, 3, and 4 years, respectively. According to another study, 12.1% of rescue workers met criteria for PTSD 2–3 years after the WTC disaster, and 19.5% met criteria 5–6 years after. Elevated PTSD risk was associated with earlier arrival time at the WTC site, prolonged work at the site, difficulty functioning at home or at work, damage to home or office, the use of various coping methods under specific stress conditions, and lower level of perceptions of social support (21222324). Accordingly, it is important to develop a screening tool that uses related predictive values to identify PTSD in rescue workers and to provide effective treatment and surveillance.
This research examined the stressors and PTSD risk of rescue workers at a disaster site using a unique analysis, the CQR method. However, this study has several limitations. The number of subjects of this study was 11, which was sufficient for the performance of a CQR analysis but too small for a statistical analysis based on PTSD-related scores. Additionally, our in-depth interviews addressed only the stressors of and motivations for disaster relief work, and we did not perform evaluations based on the diagnostic criteria for PTSD; thus, we could not determine the prevalence of PTSD. Future research with a similar disaster relief team that experiences an aftershock should rely on a large-scale analysis and a long-term follow-up assessment for purposes of comparison with the results of this study.
Unlike primary disaster victims, rescue workers are repeatedly exposed to disaster-related stress and require continuous psychological counseling about the stress (6). Efforts to reduce stress related to disaster relief work are also needed. Disaster-related stress is reducible by enhancing disaster preparedness through training and education. Man-made problems, especially those that were mentioned most commonly, problems with cooperation and teamwork, are solvable by improving systems and conducting preliminary trainings.
In conclusion, many subjects in this study suffered from various stresses after the relief work, but they had no other choice but to attempt to forget about their experiences over time. We hope that the mental health of disaster relief workers will improve through the further development of effective treatment and surveillance programs in the future.
 XML Download
XML Download