

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Partial nephrectomy (PN) represents the current standard of care for T1 renal tumors that are 4 cm or less in diameter (123). For larger T1b tumors, several retrospective studies have reported that elective PN yields equivalent oncological, but superior renal functional outcomes compared with radical nephrectomy (RN) (45). By reducing surgery-induced chronic kidney disease (CKD), PN for these patients has been suggested to be associated with reduced cardiovascular morbidity and overall mortality (46). However, the only randomized study to date conducted by the European Organization for the Research and Treatment of Cancer (EORTC) on this subject could not demonstrate benefit in overall survival, despite a significant reduction in surgery-induced CKD (7).
Surgery for renal tumors is selected based on various patient and tumor characteristics, and anatomical tumor characteristics are among the most important determinants. Although many indices have been studied to objectively describe renal tumors and quantify relationships between tumor characteristics and measurements of perioperative outcomes, the RENAL nephrometry score (NS) is becoming increasingly accepted (891011). The NS has been demonstrated to correlate with various perioperative outcomes, including ischemia time and postoperative complications following open, laparoscopic, and robot-assisted PN (12131415). Furthermore, several researchers have suggested that this score can predict renal cell carcinoma (RCC) grades and survival outcomes after radical surgery (1617).
In the current study, we aimed to examine if there was a subgroup among patients with T1b renal tumors who could functionally benefit from PN and develop methods to objectively identify such patients preoperatively using the NS.
MATERIALS AND METHODS
This study was performed by reviewing medical records of all patients with pathological T1b RCC who had undergone nephrectomy from 1998 to 2010. Patients with a single kidney, multiple renal tumors, or follow-up without evidence of recurrence for less than 1 year were excluded. Finally, 483 RN-treated patients and 40 PN-treated patients with a normal contralateral kidney were included for analysis. The surgical margin was negative in all patients who underwent PN. A 1:2 propensity score analysis without replacement was performed in our current patient cohort to define groups with comparable variables that indicated the potential to influence progression to postoperative CKD, including age, past medical history (diabetes mellitus or hypertension), preoperative serum creatinine levels, and tumor size (11819). The ‘MatchIt’ package within R was used to perform matching according to propensity scores.
Serum creatinine levels, which were used to calculate the estimated glomerular filtration rate (eGFR) that is based on the modification of diet in renal disease (MDRD) equation, were measured before surgery, at 3, 6, and 12 months postoperatively, and then annually for 5 years. At each time point, the probability of eGFR < 60 mL/min/1.73 m2 and the 95% confidence interval (CI) were calculated. In our present analysis, postoperative CKD was defined as an eGFR that declined to < 60 mL/min/1.73 m2 and then remained below this threshold. The NS and kidney volume change before and after PN were based on computed tomography performed before surgery and at 3 months postoperatively, as described previously (20). The affected-side kidney volume was measured before and after PN in 34 (85.0%) patients using cross-sectional imaging studies. In 6 (15.0%) of the study patients, the kidney volume reduction after PN could not be calculated because the pre- or/and post-operative cross-sectional imaging studies had not been digitized.
Patients and tumor characteristics were compared between patients who underwent RN and PN using the Pearson's χ2 test and Student's t-test. The probability of developing 5-year postoperative CKD according to operative methods (PN vs. RN) and the risk factors for CKD were evaluated using Kaplan-Meier analysis, in which the continuous variables were dichotomized using median values. Generation of a Cox regression proportional hazards model with and without interactions and tests of the model that assessed the area under the curve (AUC) of the receiver-operating characteristics (ROC) curve were carried out to identify independent prognostic variables for CKD at 5 years. Additional analyses that stratified patients according to the NS (≤ 8 vs. ≥ 9) were performed within the propensity-adjusted analyses. Recurrence-free survival, cancer-specific survival, and overall survival according to the NS were calculated and compared using Kaplan-Meier analyses and the log-rank test. The mean follow-up duration was 105 months (median, 106 months; interquartile range [IQR], 66–139). All statistical comparisons were performed using SPSS software, version 21 (SPSS Inc., Chicago, IL, USA) and R version 3.0.2 (http://www.R-project.com). A threshold for statistically significant differences was set at P < 0.05.
RESULTS
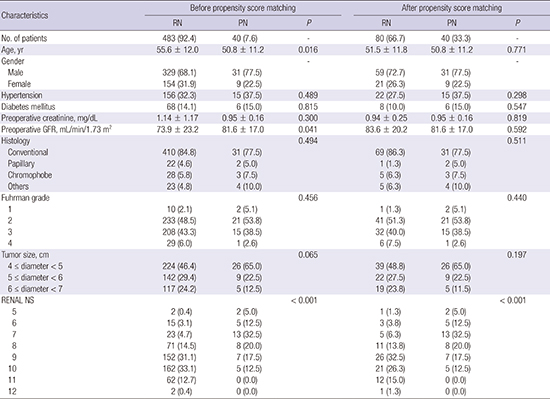
The patient and tumor characteristics for the entire study cohort are presented in Table 1. Prior to matching, the rates of CKD at 3 and 6 months postoperatively were 62.9% (95% CI, 58.9–67.2) and 62.7% (95% CI, 58.2–67.4) respectively, which was significantly reduced by 5 years postoperatively (50.0%; 95% CI, 43.0–57.0). After matching, there were no significant differences between the 2 groups except for the NS (P < 0.001). The postoperative 5-year CKD probability for the entire patient cohort was 32.1% (Fig. 1A), and was 40.7% after RN and 13.5% after PN (P = 0.005). A reduction in the rate of incidence of CKD by PN was more pronounced in patients < 50 years old, without a past medical history and with a preoperative eGFR < 80 mL/min/1.73 m2; however, compared to RN, PN reduced the risk irrespective of these characteristics (Fig. 1B-D). Additionally, the CKD probability was significantly lower following PN compared with RN in patients with an NS ≤ 8 (3.6% vs. 61.9%; P < 0.001), but not in patients with an NS ≥ 9 (33.0% vs. 38.3%; P = 0.746) (Fig. 1E).
Table 1
Patient and tumor characteristics before and after propensity score matching

Fig. 1
CKD probability according to operative methods. Solid line, all patients; dotted line, RN; dashed line, PN. (A) Entire cohort (P = 0.005); (B) Patients aged < 50 years (P = 0.013) and ≥ 50 years (P = 0.063); (C) Patients with a past medical history (HTN or DM; P = 0.132) and without a past medical history (P = 0.008); (D) Patients with a preoperative estimated GFR < 80 mL/min/1.73 m2 (P = 0.014) and ≥ 80 mL/min/1.73 m2 (P = 0.073); (E) Patients with a RENAL NS ≤ 8 (P < 0.001) and ≥ 9 (P = 0.746).
CKD = chronic kidney disease, RN = radical nephrectomy, PN = partial nephrectomy, HTN = hypertension, DM = diabetes mellitus, GFR = glomerular filtration rate, NS = nephrometry score.

The pre- and post-operative operated-side kidney volumes were 224.7 ± 42.6 mL and 136.2 ± 34.3 mL, respectively, in patients who underwent PN. The absolute kidney volume reduction was 88.6 ± 47.7 mL and the percent volume reduction was 38.0% ± 15.9%. Preoperative kidney volumes were similar between patients with an NS ≥ 9 and ≤ 8 (234.3 vs. 222.2 mL; P = 0.510). The percent volume reduction was slightly greater in patients with an NS ≥ 9 compared to ≤ 8, but this difference was not statistically significant (48.1% vs. 35.4%; P = 0.060). Ischemia time was recorded in 31 (77.5%) patients who underwent PN; among these patients, cold ischemia was performed in 7 (22.6%) patients. There were no significant differences in the ischemia time between patients with an NS ≥ 9 and ≤ 8 (24.3 vs. 21.2 minutes; P = 0.363).
We also tested for variables associated with CKD. By univariate analysis, an older age at operation (P < 0.001) increased the risk of CKD, whereas a higher preoperative eGFR (P < 0.001) and PN (P = 0.008) reduced this risk. We observed a significant interaction between the NS and the operative methods (hazard ratio [HR], 17.65; P = 0.015), and we found that the model was significantly more robust after accounting for this interaction (AUC, 0.878 vs. 0.825; P = 0.030). Therefore, in the Cox regression analysis for postoperative CKD progression at 5 years post-surgery, we stratified patients according to the surgical methods — RN or PN. In our present analysis, PN significantly reduced the CKD probability in patients with an NS ≤ 8 (HR, 0.054; 95% CI, 0.007–0.411), but not in patients with an NS ≥ 9 (HR, 0.996; 95% CI, 0.333–2.981; Table 2).
Table 2
Comparison of the CKD probability after PN or RN surgery

Recurrence-free survival was poorer in patients with an NS ≥ 9 compared to NS ≤ 8 (P = 0.047; Fig. 2). However, overall survival (P = 0.697) and cancer-specific survival (P = 0.272) were comparable between these 2 groups. There were no differences in recurrence-free survival, cancer specific survival, or overall survival in patients with an NS ≤ 8 vs. ≥ 9 according to the operative methods, respectively.
Fig. 2
Oncological outcomes according to the RENAL NS. Solid line, RENAL NS ≥ 9; dotted line, RENAL NS ≤ 8. (A) Recurrence-free survival (P = 0.047); (B) Overall survival (P = 0.697); (C) Cancer-specific survival (P = 0.272). Each line has a different meaning (solid line, RENAL NS ≥ 9; dotted line, RENAL NS ≤ 8).
NS = nephrometry score.

DISCUSSION
For elective cases of T1b renal tumors, the recommendation of PN over RN is derived from the benefits obtained by preserving renal function without compromising oncological outcomes (21). However, we often observe that despite nephron-sparing surgery, some patients still progress to CKD. On the other hand, not all patients progress to CKD following RN. Although current treatment guidelines suggest PN whenever it is technically feasible (322), we found that not all spared nephrons remain functional and that further differentiation in the selection criteria was necessary. The usefulness of the tools for preoperatively describing tumor complexity, such as the NS, has been investigated and consistently shown to be applicable for selecting operative methods and patient counseling (10). In our present study, we showed that NS can be used to identify a subgroup of patients who can benefit from PN. Reduction of risk for CKD progression by nephron-sparing surgery was observed only in tumors with NS ≤ 8, but not in tumors with NS ≥ 9. Similar progression to CKD was observed following PN or RN for tumors with NS ≥ 9.
The NS numerically represents tumor anatomical detail in relation to renal structures. This score can generally be divided into 3 categories (low, 4–6; intermediate, 7–9; and high, 10–12). In our present study, the proportion of patients undergoing PN markedly reduced with advancing NS, and that less than 5% of renal masses with high NS underwent PN, which is similar to the findings of a previous study (11). Similar to our present study, all previous studies that reported benefits of PN for T1b tumors were based on non-randomized retrospective series. Therefore, patients in the previous studies may have been heavily selected, resulting in a consistent detection of an advantageous role for PN over RN. Based on our results, we suggest that a NS of 9 may be a clinically useful cut-off. For a T1b tumor to be assigned a NS ≥ 9, it should be entirely endophytic, renal hilum-invasive, and/or cross the midline of the kidney. Such lesions appear to be more hilar and centrally located for moderately sized tumors. Compared to tumors at more polar locations, excision of these central tumors involves severing vascular structures and suture-hemostasis at a more proximal level. This can lead to loss of function due to devascularization, even if the parenchymal volume is spared. Our findings of similar percent volume reductions after similar ischemia times for NS ≤ 8 and ≥ 9 patients, but significantly greater progression to CKD in patients with an NS ≥ 9 supports this hypothesis.
The decision to conduct PN is generally made based on various tumor and patient characteristics, as well as the preferences of the surgeon. Compared to RN, PN inherently involves a higher risk of perioperative complications (23). Although minimally invasive PN approaches are becoming more popular, they are associated with a higher rate of complications, even for the most experienced hands (24). Furthermore, methods to achieve cold ischemia during minimally invasive PN are not yet available. T1b tumors are frequently complex, as was indicated by the NS distribution in our present patient cohort, so the conventional open method with cold ischemia over a minimally invasive approach may be preferred when nephron-sparing options are considered. However, if the nephron-sparing approach cannot preserve as much function as expected, the merits and limitations of open PN and minimally invasive RN should be compared before operative modalities are selected. While cancer control and renal function preservation are the primary goals of surgery for these patients, quality of life also needs to be considered if these primary objectives can be equally achieved (21). Considering the similar functional outcomes after RN and PN found in our current study in patients with NS ≥ 9, we propose that minimally invasive RN could be a better choice for these patients. Open PN requires longer convalescence and poorer cosmesis than minimally invasive surgeries. Moreover, such patients could be spared the risk of developing potential complications of PN or undergoing the hardships of open surgery and instead be offered minimally invasive RN. However, the selection of operative methods should remain highly individualized after consideration of the overall status of the patient.
PN has been recommended for T1b tumors based on evidence of equivalent oncological outcomes compared with RN (5). However, we previously reported that hilar-located tumors are associated with poorer recurrence-free survival (25). In this present study, patients with a NS ≥ 9 had more aggressive tumors and showed a lower recurrence-free survival rate, consistent with the findings of previous studies (1626). For patients with a NS ≥ 9 tumor and a normal contralateral kidney, minimally invasive RN can be expected to achieve better oncological outcome and similar functional outcome compared to PN. In patients with an NS ≤ 8, oncological outcomes were similar between RN and PN. Although these results need to be validated, our present findings support the use of RN rather than PN for complex, centrally located tumors.
Our present study was limited by the small number of patients who underwent PN. Because of compensatory changes in renal function, a relatively long follow-up period is thought to be essential for assessing the probability of CKD development. Therefore, patients who had been recently operated on could not be included in our cohort. Another limitation was that the probability of pathological upstaging was ignored because patients were selected based on pathological staging, rather than clinical staging, to compare oncological outcomes. PN might neglect microvascular infiltration, although RN allows for examinations of the microvasculature. However, the probability of pathological upstaging in clinical T1b RCC was equivalent between our patients who underwent RN and PN in our RCC registry (7.3% vs. 3.9%; P = 0.289). Our present study is of value because we could minimize the differences between the RN and PN groups and arrive at some reliable conclusions using propensity score-matched analysis. Moreover, to the best of our knowledge, our current study is the first to suggest a cut-off NS for RN in T1b RCC without increasing the probability of developing CKD over PN. Clinicians could therefore be assisted by our findings in the future when selecting optimal operative methods for patients with T1b RCC. Although there may be real benefits to elective PN for T1b renal tumors, it would be prudent to proceed with caution after considering tumor complexity. Additional studies of the roles of PN in complex T1b renal masses with a normal contralateral kidney are needed to consider the results of our present study and those of similar previous reports (27).
In conclusion, among patients with T1b renal tumors, the NS can effectively identify cases who could benefit from nephron-sparing surgery. Compared to RN, the risk of progression to surgery-induced CKD is not reduced following PN in renal tumors with a NS ≥ 9. Considering the potential complications of PN, minimally invasive RN could be considered as a viable alternative approach for this subgroup of patients.
 XML Download
XML Download