

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Preterm birth is a major cause of neonatal mortality and morbidity worldwide (123). Although the causes of preterm birth are multiple, short cervical length (CL), as measured via transvaginal ultrasonography between 20 and 24 weeks, has been implicated in the mechanisms that lead to preterm birth. Short CL has been found in approximately 0.5%–3.0% of asymptomatic singleton pregnant women (456789).
Previous studies have demonstrated that maternal characteristics such as an obstetric history, prior cervical excisional procedure, and maternal weight and height, confer a high risk of preterm birth (101112131415). However, the causality between these maternal characteristics and preterm birth remains unclear because most of the prior studies explained the relationship by using other confounders such as an obstetric history, weight, height, and a history of alcohol or substance abuse; but not included short CL. In fact, some studies reported the significant associations of obstetric history, prior cervical excisional procedure, maternal weight and height with short CL, indicating that the increased risk of preterm birth from abnormal maternal characteristics is mainly because a large proportion of women with abnormal maternal characteristics may have a short CL (8101617). However, even in these studies, whether such maternal characteristics can modify the effect of short CL on preterm birth has not been examined. Clarifying this issue has important clinical implications for patient counseling, appropriate screening, and developing preventive and treatment strategies for preterm birth. The purpose of this study is to determine the maternal characteristics (demographics, obstetric history, and prior cervical excisional procedure) that are associated with a short mid-trimester CL and whether having a short CL explains the association between these maternal characteristics and spontaneous preterm delivery (SPTD).
MATERIALS AND METHODS
This was a single-center retrospective cohort study conducted at Seoul National University Bundang Hospital (Seongnam, Korea), a tertiary-care teaching hospital, between July 2004 and April 2014. Women with singleton pregnancies who attended routine antenatal clinics to undergo anomaly scan and CL measurements between 20 and 24 weeks of gestation were consecutively enrolled. Since 2004, we have routinely measured CL by transvaginal ultrasonography in the mid-trimester in all asymptomatic pregnant women who attended an antenatal clinic and maintained a database that prospectively collected clinical data on these women. The asymptomatic women included in this study were identified retrospectively through the computerized database. The exclusion criteria were multiple gestation; a prophylactic cerclage earlier in the pregnancy; losses to follow-up after mid-trimester CL measurements; prior termination of pregnancy because of fetal anomalies at 16–23 weeks or intrauterine fetal demise; prior iatrogenic preterm birth; symptomatic preterm labor; preterm premature rupture of membranes (PPROM); major congenital anomalies; and dead fetus.
The following data were extracted from the database: maternal demographic characteristics (age, weight, height, and parity), obstetric history, sonographic CL, gestational age at the time of CL measurement, and pregnancy outcomes. Prior cervical excisional procedures (defined as either a loop electrosurgical excision procedure or cold knife cones) were obtained from a review of electronic medical charts. Obstetric history was classified into the following categories: nulliparity; a history of at least 1 SPTD; and at least 1 term birth and no preterm birth (low-risk history group). A nullipara was defined as women in their first pregnancy or where previous pregnancies did not progress after 15 weeks 6 days. Women with previous SPTD were defined as those with a history of preterm delivery (20–36 + 6 weeks) caused by preterm labor, PPROM, and cervical insufficiency.
Transvaginal ultrasonography to measure CL was performed by Maternal Fetal Medicine faculties or fellows by using either a Voluson 730 Expert (GE Healthcare, Milwaukee, WI, USA) or an Aloka SSD 5500 (Aloka Co. Ltd., Tokyo, Japan) ultrasound machine equipped with a 6.0-MHz transducer. The detailed description of CL measurements was published elsewhere (18). In brief, after voiding, women were placed in the dorsal lithotomy position and the probe was gently inserted in the anterior vaginal fornix to visualize the cervical canal. Minimum pressure was applied with the probe to obtain a sagittal view of the complete cervix, including the internal overall survival (OS), external OS, and endocervical canal. CL was measured by placing the electronic markers at the furthest points between the internal OS and external OS, measuring it as a straight line. The shortest of 3 measurements obtained was taken as the CL. Short CL was defined as a CL of ≤ 25 mm. SPTD was defined as a delivery before 34 weeks' gestation after spontaneous onset of preterm labor or PPROM. Decisions regarding the treatment for a short cervix, such as progesterone supplementation and cerclage placement, were left to the discretion of the attending obstetrician and not specified by the protocol during the study period.
All statistical analyses were performed by using SPSS version 22.0 for Windows (IBM SPSS Statistics, Chicago, IL, USA). The Shapiro-Wilk test was used to assess for a normal data distribution. Univariate analysis was conducted with the Student's t-test, Mann-Whitney U test, or χ2 test. A multivariate logistic regression analysis was then performed to identify, among various maternal characteristics at mid-trimester, the factors that were significantly and independently associated with the risk of short CL. In this logistic regression model, only variables with P values of < 0.1 in the univariate analysis were included. In addition, by using the likelihood of SPTD as an outcome variable, logistic regression was used to determine whether any maternal characteristics related to short CL were associated with SPTD independent of short CL. All maternal factors were entered in the multivariable logistic regression analysis. In the initial regression, all maternal factors, excluding the variables “short CL” and the interaction term, were entered in the regression equation to identify the maternal factors that were significantly associated with SPTD. Next, short CL was added to the regression model to assess whether maternal factors remained associated with SPTD independent of short CL. Potential interactions between various maternal characteristics related to SPTD and short CL were evaluated as well. We assessed for multicollinearity among the variables by using a χ2 test and the Pearson or Spearman rank correlation test. Variables with a high correlation were summarized in the analysis. Obstetric history alone was included instead of both obstetric history and parity, and weight alone was included instead of both body mass index (BMI) and weight. All reported P values are 2-sided, with a significance level of 0.05.
RESULTS
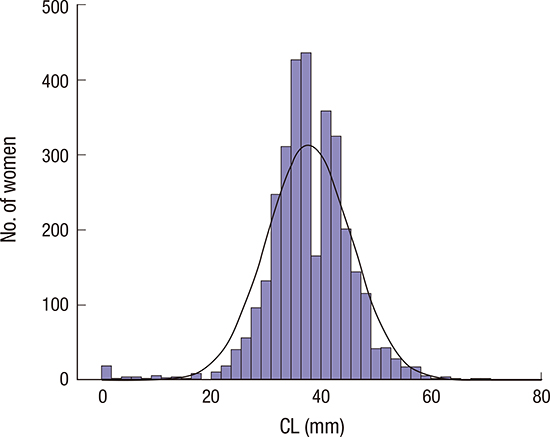
During the study period, 4,171 consecutive singleton pregnant women were screened at 20–24 weeks of gestation. Of these women, 4 refused to undergo transvaginal ultrasonographic assessment of CL and 6 had huge cervical myomas. The exclusion criteria were met in 857 of the remaining 4,161 (history-indicated cervical cerclage [n = 84], losses to follow-up after CL measurements [n = 595], prior termination of pregnancy due to fetal anomalies [n = 77], prior preterm vaginal delivery for an intrauterine fetal demise [n = 33], prior iatrogenic preterm birth due to preeclampsia and fetal growth restriction [n = 33], and incomplete data sets [n = 35]). Eight women with current iatrogenic preterm birth at < 34 weeks of gestation were further excluded from the analysis (preeclampsia [n = 6], fetal growth restriction [n = 1], and placental abruption [n = 1]). Thus, 3,296 women were suitable for the final analysis. CL was approximately normally distributed with some skewness at the lower end (Fig. 1). The mean (standard deviation [SD]) CL was 37.7 (7.7) mm at a mean gestational age of 21.3 (1.0) weeks, which was specifically 37.7 (7.5) mm for nulliparas and 37.8 (7.9) mm for multiparas (P = 0.460). The mean (SD) CLs were 37.7 (7.5), 34.7 (9.3), and 38.0 (7.8) mm for the nulliparous women, those with a previous SPTD, and those with a low-risk obstetric history, respectively. The differences were significant (P = 0.005), with the women with a previous SPTD having the shortest mean CL (Fig. 2A). The mean CL was significantly shorter in the women with than in those without prior cervical excisional surgery (P < 0.001; Fig. 2B). The CL was ≤ 25 mm in 124 women (3.8%). Among the women with short CLs, 42 underwent emergency cervical cerclage and 13 received vaginal progesterone therapy. The overall incidence rate of SPTD before 34 weeks of gestation was 2.6% (85/3,296).
 | Fig. 1Distribution of CL at 20–24 weeks of gestation in 3,296 asymptomatic singleton pregnancies. A normal distribution is displayed as a solid line.
CL = cervical length.
|
 | Fig. 2Box plots for CLs at 20–24 weeks of gestation. (A) For 3,296 asymptomatic singleton women with nulliparous status, a previous spontaneous preterm delivery (SPTD), and prior term births only. The women with a previous SPTD have significantly lower mid-trimester CLs than the women with nulliparous status or prior term births only (P = 0.001 and P < 0.001, respectively, by analysis of variance with Bonferroni correction). (B) In women with or without a history of cervical surgery. The mean CL is significantly shorter in the women who had undergone a prior cervical excisional procedure than in those who had not undergone a prior cervical surgery (P < 0.001).
CL = cervical length.
|
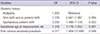
Table 1 describes the maternal and clinical characteristics of the study population according to the presence or absence of short CL (≤ 25 mm). Women with short CLs were more likely to have had undergone prior cervical excisional procedures and had CL measured at a significantly later gestational age. Moreover, based on the univariate analysis, obstetric history was significantly associated with short CL. However, no differences in maternal age, height, weight, and parity were observed. Preterm birth at < 34 weeks' gestation occurred in 32 (26%) of the 124 women with short CL and 53 (2%) of the 3,172 women with a normal cervix (P < 0.001). The result of the multivariate logistic regression analysis demonstrated that an obstetric history, gestational age at measurement, and prior cervical excisional procedure had significant independent contributions to the prediction of short CL (Table 2).
Table 1
Maternal and clinical characteristics of the study population according to the presence or absence of short CL
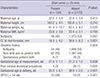
Data are mean ± SD or number (%).
BMI = body mass index, CL = cervical length, SPTD = spontaneous preterm delivery, SD = standard deviation.
![]()
Table 2
Results of the multivariate logistic regression analysis of independent variables for predicting short CL (≤ 25 mm)
![]()
In the initial regression, after adjusting for potential confounders (i.e., gestational age at measurement, emergency cerclage placement, progesterone therapy, maternal age, weight, and height), a history of SPTD, but not prior cervical excisional procedure, was significantly associated with SPTD (Table 3). This association remained significant after adjustment for the presence of short CL. After including the interaction term between a history of SPTD and short CL in the regression, the associations of short CL and history of SPTD with SPTD became stronger. In addition, an interaction between obstetric history and short CL in relation to SPTD risk was observed, suggesting that effect modification was present.
Table 3
Results of the multivariate logistic regression analyses for the outcome of spontaneous preterm birth before 34 weeks' gestation

![]()
DISCUSSION
The principal findings of this study are as follows: 1) history of SPTD and prior cervical excisional procedure were associated with an increased risk of having a short mid-trimester CL; 2) history of SPTD, but not prior cervical excisional procedure, was associated with an increased risk of SPTD, independent of a short CL; and 3) evidence of an interaction between obstetric history and short CL in association with SPTD.
Our finding that prior cervical excisional procedure was independently associated with short mid-trimester CL is consistent with the results of many previous studies (111719). These findings are expected because cervical excision seems to directly shorten the CL. However, with respect to the association between prior cervical excisional procedure and preterm delivery, the results of previous studies have been somewhat conflicting. Some studies reported no associations (2021), whereas other studies reported an association even after the addition of CL to the prediction model (111719). Our result is concurrent with the findings of the former study but differed from the findings of a recent meta-analysis conducted by Jin et al. (19). This discrepancy between studies may be related to the differences in the gestational age cutoffs used to define SPTD as a primary outcome measure; sample size; standard care for asymptomatic pregnant women at high risk of preterm delivery; inclusion and exclusion criteria; and whether known risk factors were uniformly adjusted for in the analyses (e.g., short CL).
In agreement with previously published data (102223), we found that the women with a prior SPTD had a shorter mid-trimester CL and were more likely to have short CL than the women with no history of preterm delivery (e.g., nulliparas or women at low risk), suggesting that the association between a prior SPTD and the risk of subsequent SPTD may be mediated by the shortening itself of the cervix. However, in addition, our findings from the multivariate regression models, which indicated that the observed association between prior SPTD and the risk of subsequent SPTD was independent of short CL and that a synergistic effect exists between prior SPTD and short CL in relation to subsequent SPTD, suggest that an unexplained factor poses a higher risk of subsequent SPTD to women with prior SPTD than that associated with short CL alone. This risk may include genetic background, dietary and lifestyle variables, uterine anomaly, and inherent susceptibility to infection. Further studies that use “omics” approaches are needed to elucidate underlying mechanisms by which a prior SPTD may independently contribute to a short mid-trimester CL and subsequent SPTD, with the goal of target identification for its prevention and therapy.
Our results confirm the previous works, showing that CL, as measured by using transvaginal scan at mid-trimester, is inversely associated with the frequency of preterm birth, even in women with a reassuring obstetric history, such as prior term births only and no prior cervical excisional procedure (10172425). Furthermore, we demonstrated an interaction between obstetric history and short CL in association with SPTD, suggesting a synergistic detrimental effect of these 2 variables on SPTD. This finding also agrees with those of a previous report in which unlike low-risk women with short CL, high-risk women with prior SPTD and short CL benefit from cerclage, and this benefit increases as the CL decrease (26). Taken together, these data could help in the successful identification of women at high risk of preterm delivery by increasing patients' acceptability of universal screening for CL and in the design of current and potential future strategies for prevention and treatment of preterm delivery.
Several previous studies have reported the associations between higher maternal weight and short mid-trimester CL after adjusting for baseline variables (822), although these are not consistent findings (2327). However, we did not confirm these observations. In contrast to short mid-trimester CL, our finding that higher maternal weight was independently associated with SPTD is consistent with those of previous studies (1415). Consequently, our data collectively suggest that the mechanisms underlying the risk of SPTD associated with higher maternal weight (especially obesity) might be mediated by factors involved in obesity, such as metabolic and hormonal alterations, chronic low-grade inflammation, and associated comorbidities, rather than short CL. We also found a lack of association of maternal height with a short mid-trimester CL, which is consistent with the previous findings (827), but differs from findings of another study (16). The reasons for the discrepancy regarding the association between demographic variables and the risk of short CL among studies may be related to the difference in sample size, ethnicity of the study population, the inclusion criteria related to risk status for preterm delivery, and whether confounding factors were controlled for.
The overall incidence of SPTD at < 34 weeks in our study population was 2.6%, which is similar to the data (2.1%) of other cohorts of women provided by Fonseca et al. (28). In comparison with the incidence in the general population, our incidence of short CL was lower than that (7.2% had CLs of ≤ 25 mm) reported by Moroz and Simhan (29), but was higher than that (2% had CLs of ≤ 25 mm) reported by Temming et al. (30). However, the differences in rates between our study and their studies can be explained by the gestational age to assess CL. CL assessment in the study of Moroz and Simhan (29) was conducted at a slightly later gestational age (21–28 weeks' gestation) than the 20–24 weeks in our study. CL in the study of Temming et al. (30) was measured at a slightly earlier gestational age (17–23 weeks' gestation). Our finding that incidences of a CL of ≤ 25 mm and SPTD at < 34 weeks in women with prior term deliveries only were not significantly different from those in nulliparous women is in agreement with previous works (2324).
The present study has several limitations. First, it was of a retrospective nature and was performed at a single center, which leads to a lack of generalizability of results. Second, the participants were recruited over a period of 10 years to collect a larger number of samples despite improvements in the management of women at high risk of SPTD during this period. This might lead to bias in the effect of certain risk factors on SPTD. However, it is unlikely that this bias would change our main findings because we corrected for potentially important confounders related to the medical care of women at high risk of preterm birth, such as the use of progesterone therapy and placement of a cervical cerclage. Indeed, the current data of singleton pregnancies suggest that progesterone therapy and cervical cerclage in women with a short cervix, a previous spontaneous preterm birth, or both may be effective in preventing preterm birth, as recommended by the American College of Obstetricians and Gynecologists (3132). Then, at present we follow this treatment recommendation for a short cervix. Third, we excluded a large number of women with an obstetric history for termination of pregnancy in the second trimester because this factor masks underlying characteristics of other important obstetric histories such as previous SPTD and prior term births only in cases having these factors simultaneously in obstetric history. Accordingly, we did not evaluate the effect of obstetric history for termination of pregnancy in the second trimester on short CL and SPTD. Fourth, an association between prior cervical excisional procedure and risk of SPTD could not be precisely evaluated because only few women underwent prior cervical excisional procedures (30/3,304; 0.9%), which led to a lack of statistical power to detect a difference in SPTD between the groups. This study has some strengths over other studies. First, we adjusted for many known confounding factors simultaneously and investigated more-complex effect modifications. Second, the ethnicity of our population is uniform, in which 99.5% of our participants were of Korean ethnicity, which led to less racial bias on outcome measures.
In conclusion, a history of SPTD is associated with an increased risk of short mid-trimester CL and strongly associated with subsequent SPTD, independent of short CL. The associations between a history of SPTD and subsequent SPTD were more pronounced among the women with short CL than among those with normal CL. These findings warrant confirmation by further studies and offer direction for further studies to elucidate the potential mechanisms for better understanding of the biology of women with a previous SPTD.
 XML Download
XML Download