

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Central precocious puberty (CPP) in girls is related to multiple problems, including inappropriate behavior, teenage pregnancy, and compromised final height due to early epiphyseal fusion (12). The gonadotropin-releasing hormone (GnRH) agonist is the treatment of choice for CPP, and it constantly binds to the GnRH receptor of the pituitary gland.
With the downward secular trend in pubertal timing, the number of girls diagnosed with CPP increases yearly (3). There have also been rising concerns about the potential long-term complications from treatment. A number of studies have investigated the final outcomes of GnRH agonist treatment on factors, such as the final adult height and the age of menarche (456). However, few studies have investigated the possible effects of GnRH agonist treatment on the reproductive function of CPP girls during the treatment period. Ovarian reserve is measured by conventional tests, such as estradiol (E2), basal luteinizing hormone (LH), follicle-stimulating hormone (FSH), and ultrasonography. Serum anti-Müllerian hormone (AMH) is an emerging marker for follicle reserve because of its low fluctuation and high availability (7).
Therefore, we aimed to assess the ovarian function by analyzing the serum AMH levels of CPP girls according to the GnRH agonist treatment stage cross-sectionally. We also compared the serum AMH levels in CPP girls with those of normal controls at the treatment initiation point and at follow-up after discontinuation.
MATERIALS AND METHODS
Subjects
We reviewed the records of 505 CPP girls who visited the Pediatric Endocrinology Clinic of Korea University Hospital between May 2012 and September 2015 for the evaluation of early pubertal signs. CPP was diagnosed based on the appearance of breast budding before the age of 8 years and bone age advancement, together with a pubertal peak LH level ≥ 5 IU/L before the age of 9 years. The girls were treated with a long-acting GnRH agonist (3.75 mg of leuprolide acetate) every 4 weeks. We subdivided the CPP girls into 5 groups based on the GnRH agonist treatment stage: group A (before treatment, n = 98), group B (3 months after initiation, n = 103), group C (12 months after initiation, n = 101), group D (24 months after initiation, n = 101), and group E (6 months after discontinuation, n = 102).
To assess whether the AMH levels were affected by the GnRH agonist treatment, we included 100 healthy girls as control subjects. The bone age-matched healthy girls were subdivided into 2 groups: control group 1 (before treatment, n = 55) and control group 2 (after discontinuation, n = 45).
Methods
We retrospectively reviewed the chronological age, bone age, height, weight, and body mass index (BMI, kg/m2) at the initial GnRH stimulation test, as well as the laboratory profiles. The height, body weight, and BMI were expressed as standard deviation scores (SDSs) from those of Korean girls of the same chronological age.
The serum concentrations of the basal LH and FSH were measured with an immunofluorimetric assay kit (DIAsource immunoassay, Louvain-la-Neuve, Belgium). The E2 level was measured using a radioimmunoassay kit (Siemens, Camberley, UK) and the insulin-like growth factor-I (IGF-I) level was measured with a double antibody immunoradiometric assay kit (Immunotech, Marseille, France).
For the AMH assay, the blood samples were centrifuged (2,330 × g for 7 minutes) within 30 minutes, and the serum was stored at 2°C–8°C within 24 hours until analysis. The serum AMH levels were measured with the AMH Gen II enzyme-linked immunosorbent assay kit (Beckman Coulter Inc., Brea, CA, USA). The intra-assay and inter-assay variation coefficients were less than 3.7% and 4.4%, respectively, and the lower detection limit was 0.08 ng/mL. The normal reference range of AMH level is 2.2–6.8 ng/mL based on the data of young women aged 20–31 years (89).
Statistical analysis
The SPSS software version 20.0 (IBM Co., Armonk, NY, USA) was used for the statistical analyses. Independent t-test and Mann-Whitney test were performed for comparison of the 2 groups. One-way analysis of variance (ANOVA) and repeated measures ANOVA were conducted to compare the clinical and biochemical parameters of the groups. The χ2 test was used to assess the proportion of normal AMH levels. Pearson's correlation coefficients were calculated to evaluate the relationship between the AMH levels and other factors. All the data were expressed as mean ± standard deviation (SD), and a P value < 0.05 was considered statistically significant.
RESULTS
Clinical and biochemical characteristics of CPP girls according to stage of GnRH agonist treatment
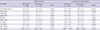
The mean chronological age of group A was 8.4 ± 0.7 years, and the mean bone age was 9.9 ± 0.6 years. The height SDS, body weight SDS, and mean BMI SDS were 1.0 ± 0.7, 0.8 ± 0.9, and 0.4 ± 0.9, respectively. The mean chronological age of group E was 11.8 ± 0.6 years, and the mean bone age was 12.7 ± 0.4 years. The height SDS significantly decreased to 0.7 ± 0.9 (P = 0.036 as compared with group B), while the body weight SDS and mean BMI SDS were 0.6 ± 0.9 and 0.4 ± 1.0, respectively (Table 1).
Table 1
Clinical and biochemical characteristics of CPP girls according to stage of GnRH agonist treatment

Data are presented as mean ± SD.
CPP = central precocious puberty, GnRH = gonadotropin-releasing hormone, SDS = standard deviation score, BMI = body mass index, AMH = anti-Müllerian hormone, E2 = estradiol, LH = luteinizing hormone, FSH = follicle-stimulating hormone, IGF-I = insulin-like growth factor-I, SD = standard deviation, ANOVA = analysis of variance.
Each marks means significant differences between groups as determined by Tukey's multiple comparison test; *P < 0.05 compared with group A; †P < 0.05 compared with group B; ‡P < 0.05 compared with group C; §P < 0.05 compared with group D; ‖P < 0.05 by one-way ANOVA.
![]()
The mean AMH level of group A was 5.9 ± 3.6 ng/mL. The mean AMH level of group B was lower (4.7 ± 3.2 ng/mL, P = 0.047 as compared with group A), and this reduction in the AMH level diminished after 12 months and 24 months of treatment (4.9 ± 3.1 ng/mL, P = 0.176 and 5.5 ± 3.0 ng/mL, P = 0.937 as compared with group A, respectively). Six months after discontinuation of the GnRH agonist treatment, the AMH levels were similar to those at pre-treatment (5.1 ± 3.3 ng/mL, P = 0.075). The mean AMH levels were all within the normal reference range (2.2–6.8 ng/mL). The E2, LH, FSH, and IGF-I levels were also significantly higher in group E (P < 0.001 as compared with group A, group B, group C, and group D) (Table 1).
Comparison with normal controls before treatment and after discontinuation of GnRH agonist treatment
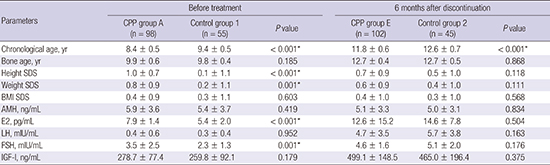
Before initiation of the GnRH agonist treatment, the chronological age of the CPP group A was lower (8.4 ± 0.5 years vs. 9.4 ± 0.5 years, P < 0.001), and both their height SDS and weight SDS were higher (1.0 ± 0.7 years vs. 0.1 ± 1.1 years, P < 0.001 and 0.8 ± 0.9 years vs. 0.2 ± 1.1 years, P = 0.001, respectively). However, their bone age and BMI SDS were similar to those of the girls in normal control group 1. Six months after discontinuation of the GnRH agonist treatment, the chronological age of the CPP group E was lower (11.8 ± 0.6 years vs. 12.6 ± 0.7 years, P < 0.001), but their bone age, height SDS, weight SDS, and BMI SDS were similar to those of the girls in normal control group 2 (Table 2).
Table 2
Comparison with normal controls before GnRH agonist treatment and after discontinuation of treatment
Data are presented as mean ± SD.
GnRH = gonadotropin-releasing hormone, CPP = central precocious puberty, SDS = standard deviation score, BMI = body mass index, AMH = anti-Müllerian hormone, E2 = estradiol, LH = luteinizing hormone, FSH = follicle-stimulating hormone, IGF-I = insulin-like growth factor-I, SD = standard deviation.
*P < 0.05.
![]()
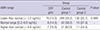
The AMH levels of the CPP group A and CPP group E were similar to those of the bone age-matched controls (5.9 ± 3.6 ng/mL vs. 5.4 ± 3.7 ng/mL, P = 0.419 and 5.1 ± 3.3 ng/mL vs. 5.0 ± 3.1 ng/mL, P = 0.834, respectively). The E2, LH, FSH, and IGF-I levels 6 months after discontinuation were also similar to those of the girls in control group 2 (Table 2). No difference in the proportion of AMH range (lower than normal, normal, and higher than normal) was observed among CPP girls, control group 1, and control group 2 (P = 0.999) (Table 3).
Table 3
Comparison in proportion of AMH range among CPP girls, control group 1, and control group 2
Data are presented as number (%); P value was obtained by χ2 test.
AMH = anti-Müllerian hormone, CPP = central precocious puberty.
![]()
Correlation between AMH level and other factors
A univariate analysis was performed using a simple linear regression to examine the correlation between the AMH level and other factors. At baseline, the AMH level was negatively correlated with the FSH level (r = −0.264, P = 0.009). No correlation was found during the treatment or at 6 months after discontinuation of the GnRH agonist treatment (3 months: r = 0.016, P = 0.873; 12 months: r = −0.018, P = 0.857; 24 months: r = −0.102, P = 0.321; 6 months after discontinuation: r = −0.157, P = 0.110). The AMH level did not correlate with the chronological age, bone age, height SDS, weight SDS, BMI SDS, E2 level, LH level, or IGF-I level (data not shown).
DISCUSSION
This cross-sectional study evaluated the possible effects of GnRH agonist treatment on the ovarian function by examining the serum AMH levels of CPP girls. The results showed that the mean AMH level after 3 months of GnRH agonist treatment was lower than that at baseline. This reduction in the AMH level diminished after 12 months of treatment. Six months after discontinuation of the GnRH agonist treatment, the AMH levels were similar to those at pre-treatment. Before and after treatment, the AMH levels of the CPP girls were similar to those of their bone age-matched controls.
Besides compromised final adult height, CPP causes inconsistencies between physical and psychological development. According to the “8th Korea Youth Risk Behavior” web-based survey, early menarche is strongly associated with early sexual intercourse and teenage pregnancies (10).
The GnRH agonist is the treatment of choice for CPP. Although it is considered effective and well-tolerated, the potential long-term complications of GnRH agonist treatment remain controversial (11). For example, it is unclear whether polycystic ovarian syndrome is caused by the premature adrenarche that presents at the onset of CPP, or whether it is a side effect of GnRH agonist treatment (1213). Several studies have reported that the ages of menarche in treated CPP girls were similar to those of normal healthy girls, and that GnRH agonist-treated patients experienced regular menstrual cycles (4141516).
With the increasing number of girls diagnosed with CPP, concerns about the potential long-term complications at the time of diagnosis and during the subsequent period of GnRH agonist treatment have also increased. However, few studies have investigated the presence and use of markers that may indicate the possible effects of the treatment on the reproductive function. This study assessed the ovarian function by analyzing the AMH levels before, during, and after GnRH agonist treatment.
As the ovarian function cannot be measured directly, several serum markers or ultrasound parameters have been used instead (17). The AMH was discovered by Alfred Jost in the 1940s and has been serving as a biomarker of the ovarian reserve since 2002 (1819). AMH is only produced in the granulosa cells; thus, its level is likely to present a high specificity and sensitivity in reflecting the presence of ovaries (20).
The AMH levels increase temporarily immediately after birth up to 3 months of age. Further increases are then detected at 4 years of age and around puberty. After puberty, the AMH levels remain relatively stable until early adulthood (21). The serum AMH levels decrease with older age, increasing BMI, and gonadotropin administration (172223). In a recent study of 13 CPP girls and 2 early puberty girls, the partial reduction of the AMH level by a GnRH agonist treatment suggested a partial gonadotropin dependence of the AMH (24).
While other studies only included a comparison of the results with those of normal controls at baseline, we also included a comparison with normal controls after discontinuation of the treatment. In this study, the AMH levels returned to pre-treatment levels after discontinuation of the GnRH agonist treatment, and the mean AMH levels during the treatment were all within the normal reference range. We did not find a significant difference between the AMH levels of the CPP girls and those of the bone age-matched healthy girls at baseline or after discontinuation of the treatment.
Although the AMH levels remain stable throughout childhood and adolescence, cross-sectional analyses and longitudinal data have shown modest late pre-pubertal peaks and a slight decline in the first 2 years after the pubertal onset in healthy girls (252627). The mechanism underlying this decline has not been identified. However, it may be explained by the progression of the preantral and small antral follicles to the antral follicles, which do not produce AMH at the onset of puberty (23). The slight decrease in AMH levels observed in this study could be explained by the coincidence of the pubertal onset rather than by the suppressive effects of the GnRH agonist treatment.
FSH plays a role in AMH regulation. Several studies have found an inverse association between the AMH and FSH levels (2528). In this study, the AMH level was only negatively correlated with the FSH level before the GnRH agonist treatment. The changes in the AMH levels did not correlate with the changes in the gonadotropin or E2 levels during or after treatment. One explanation for this result may be that the AMH levels decrease at the time of hypothalamus-pituitary-ovarian axis activation.
The application of AMH has some limitations in clinical practice. While AMH is a good predictor of the ovum supply, it may not predict the ovum quality. Nevertheless, our study was significant in demonstrating that no differences were found in the AMH levels of CPP girls and normal controls after discontinuation of the GnRH agonist treatment. As this was a cross-sectional study, inter-individual variations may have been possible. Therefore, further longitudinal studies are needed.
In conclusion, the AMH levels of CPP girls were partially reduced at the early stage of the GnRH agonist treatment, but returned to pre-treatment levels after discontinuation of the treatment. All of the AMH levels according to the GnRH agonist treatment stages were within the reference range. There was no evidence to suggest any adverse effects of GnRH agonist treatment on the reproductive function.
 XML Download
XML Download