

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Attention deficit hyperactivity disorder (ADHD) is a neurobehavioral disorder characterized by core symptoms of inattentiveness, hyperactivity, and impulsivity. According to predominant symptoms, the Diagnostic and Statistical Manual of the American Psychiatric Association (Diagnostic and Statistical Manual of Mental Disorders 4th edition [DSM-IV]) recognizes 3 subtypes of ADHD: predominantly inattentive, predominantly hyperactive-impulsive, and combined subtype (1).
ADHD is 1 of the most common mental disorders in children between the ages of 5 and 15 years and affects approximately 8%–12% of children worldwide (2). Its impact on society is enormous in terms of financial cost, stress to families, interference with academic and vocational activities, as well as negative effects on self-esteem (3). Due to the substantial burden of this disease, an accurate estimate of ADHD prevalence is essential. In Korea, some studies have reported ADHD in association to environmental exposure to chemicals, genetic components, and co-morbidity of other psychiatric disorders (4,5). The prevalence of ADHD among the adults have been studied in a small scale (6-8), which did not provide information on the prevalence in children. The prevalence of ADHD in children was reported with a wide range such as 5.9% and 9.0% in Korea, even though they were confined to Seoul (9,10).
The present study was conducted to estimate the prevalence of ADHD and its comorbidity among Korean children in a community by a screening questionnaire with a rating scale and diagnostic clinical assessment.
MATERIALS AND METHODS
Study population
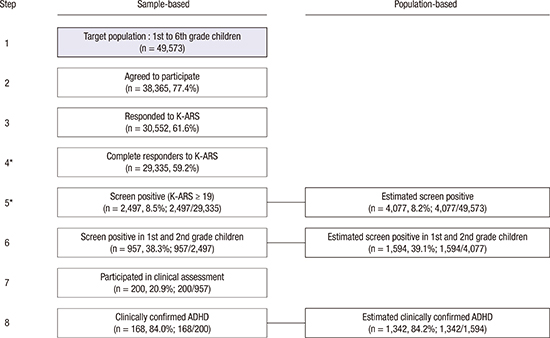
This study was conducted between 2007 and 2010 in Cheonan, which is a medium sized city with a mix of urban, rural, and industrial areas (Korea). The number of school-aged children in Cheonan is 49,273, which was the target population and included all students in 65 elementary schools (1st to 6th grade) from between September 2007 and August 2008. Of the 65 schools, 49 schools agreed to participate (n = 38,365 children) (Fig. 1). A total of 30,552 children, with respective parents, agreed to participate and responded to the Korean version of ADHD Rating Scale (K-ARS). Between 2009 and 2010, a pediatric psychiatrist clinically assessed selected children who showed positive result in screening on K-ARS and were in either 1st or 2nd grade at the time of screening (n = 200). Written informed consent was obtained from the parents or guardians and also from children, prior to study participation.
ADHD diagnosis
We used a 2-stage design for case identification (Fig. 1). In the first stage, a systematic screening was performed using the K-ARS, an 18-item questionnaire assessing inattentiveness and hyperactivity (11). The score of K-ARS can be between 0 and 54. Screen positive were defined the score of K-ARS was greater than 18. All parents or guardians were asked to complete the K-ARS. Children were considered to be screen-positive for the K-ARS scores greater than 18. In the second stage, the screen-positive children were evaluated by a standardized clinical assessment. Among the 1st and 2nd grade students, 957 children showed screen-positive, and extensive efforts were made to contact parents of these children. Among these parents, 20.9% (n = 200) provided consent for diagnostic evaluations. Children whose parents could not be contacted or did not agree to participate were classified as nonparticipants.
All diagnostic interviews were performed by a pediatric psychiatrist using the standard procedures for diagnosing ADHD, including the Attention-deficit Diagnosis System (ADS) and the Korean version of the modified computerized test of variables of attention (TOVA) (12). The children with standard score greater than 70 with ADS as like TOVA and if they met the DSM-IV criteria for attention-deficit hyperactivity disorder, they were diagnosed as having ADHD. The pediatric psychiatrist identified the dominant ADHD symptom domain (inattentive, hyperactive, or combined subtype) for each case based on all the results: the K-ARS score (≥ 9 for each symptom domain), or ADS score (≥ 60 for each symptom domain), and DSM-IV criteria.
Co-morbidity diagnosis
Additional assessments were performed using the scales such as the Behavior Assessment System for Children II (BASC-II), Korean Child Behavior Checklist (K-CBCL), Kovacs' Children's Depression Inventory (CDI), State Anxiety Inventory for Children (SAIC), Trait Anxiety Inventory for Children (TAIC), Korean Wechsler Intelligence Scale for Children (K-WISC)-III, and an evaluation for Tic symptoms. These scales were administered to the parents or guardians when children came to visit the pediatric psychiatrist for the clinical assessment.
Socio-demographic factors
The screening questionnaire was used to obtain the following socio-demographic factors: gender, age (years), parental marital status (not married, cohabited, separated, divorced, bereaved, married, and unknown), educational level of father/mother (< 12 years, 12 years, > 12 years), and occupation of father/mother (yes, no).
Statistical analysis
The rate of positive results in ADHD screening was estimated from the scores of screening questionnaires and diagnostic assessments. Its point estimate was computed at the population level with proper survey weights. The weights were developed to compensate for both nonresponding schools and nonparticipating subjects (either students or parents). Since there was no sampling involved, the initial weights of both schools and students in the population were set to one. Then, each weight was inflated with the corresponding multiplicative adjustment factor to compensate for nonresponse. A basic assumption behind nonresponse adjustments is that nonresponse does not depend on either survey variables or other characteristics related to the survey unit, which is technically termed as “missing completely at random (MCAR).” The detailed method was provided as the supplementary material. Point prevalence was estimated by gender, age, parental marital status, educational level of parents, and any occupation of parents.
Simple logistic regression analysis was used to assess the association between ADHD risk (evaluated as screen positive) and socio-demographic covariates. The statistical significance of differences between estimates was assessed by using logistic regression; odds ratios (ORs) and 95% confidence intervals (CIs) are reported. Both precision measures (standard errors [SEs] and CIs) were computed by using the above weights, downscaled to make the sum equal to the total number of K-ARS responding students. Such an additional adjustment would reserve the proper compensation for the nonresponse and would also help avoid overstating the precision. Statistical analyses were conducted using proc logistic procedure in SAS (version 9.2; SAS Institute, Cary, NC, USA). P values of less than 0.05 were considered statistically significant.
RESULTS
Subjects characteristics
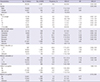
The mean age was 9.2 years with a standard deviation of 1.7. The majority of parents who responded was married (77.9%), employed (76.2%), and had graduated from high school (97.9%). Details regarding the distribution of socio-demographic variables are summarized in Table 1.
Table 1
Screen positive (%) of ADHD according to socio-demographic characteristics (n = 29,335)
![]()
Prevalence of ADHD
The median values (Q1–Q3) of K-ARS score of boys and girls were 8 (4–14) and 5 (2–10), respectively. The screen positive of ADHD among boys and girls were 11.7% and 5.2%, respectively (Table 1). The point prevalence of ADHD in the community was 85 per 1,000 children, as estimated from on the results of screening questionnaire and diagnostic assessment (Table 2). Boys were 2.4 fold more likely to have ADHD than girls, with prevalence of 117 per 1,000 boys and of 52 per 1,000 girls. Eight-year-old children showed the highest ADHD prevalence in this study. Children with separated parents were at 3.4 fold greater odds of having ADHD than those with married parents. Children whose father or mother was educated for less than 12 years had more than 3 fold higher risk of having ADHD than children whose parents were educated for 12 or more years. Children whose fathers did not have an occupation or whose mothers did have an occupation were at a greater risk of having ADHD.
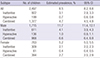
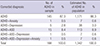
Table 2
Prevalence estimates of ADHD subtypes by gender (n = 29,335)
![]()
ADHD subtypes and co-morbidity
The combined subtype was most prevalent, and followed by the inattentive type and hyperactive type (Table 2). Table 3 illustrates psychiatric co-morbidities for the 200 children with clinically diagnosed ADHD. Among these, 23 subjects (12.7%) had at least 1 co-morbid disorder. Autism spectrum disorder (ASD) was the most common co-morbidity, followed by depression and anxiety.
Table 3
Co-morbidity between ADHD and other psychiatric disorders in a sample of 200 children
![]()
DISCUSSION
Epidemiological studies have reported highly variable rates of childhood ADHD prevalence worldwide, ranging from 2.2% to 17.8% (13-21). This wide discrepancy between studies could be due to methodological differences, use of different systems of classification, and variations in ADHD definition. In this study, the prevalence of ADHD among Korean children in a community was 8.5% (95% CI, 8.2–8.8), which is slightly higher compared to the pooled worldwide ADHD prevalence of 6.8% in a meta-analysis (20), and is in between those reported as children's ADHD prevalence in Seoul, 5.9% (9) and 9.0% (10). To our knowledge, our study is the first large-scale epidemiological survey on ADHD among Korean in a community.
ADHD is diagnosed approximately 3 times more often in boys than in girls (22-24). The gender ratio in this study was similar with the previous reports. It is reported that this difference between genders may reflect either a difference in susceptibility or that females with ADHD are less likely to be diagnosed than males (25). However, the underlying physiological mechanism that causes ADHD is still not thoroughly understood and remains under investigation.
A significantly higher prevalence of ADHD was found among children whose parents were separated or divorced and/or less educated. This can be interpreted by the fact that children whose parents are separated or divorced do not receive proper attention and care from parents, and this leads to a greater incidence of ADHD symptoms. This was not the case in children being raised by a single parent in bereavement. Interestingly, children with unemployed fathers showed a higher prevalence of ADHD, while those with unemployed mother showed lower prevalence. This might be attributed to the traditional roles of each parent, i.e., father as the head of household, and mother as the homemaker. Even though the percentage of working mothers in Korea had spiked to 43.6% in 2011, only 9.2% of wives conceded that the division of household labor is equally assigned in a study (26).
Currently, there are 2 diagnostic criteria used to diagnose ADHD in children, DMS-IV and International Classification of Diseases 10th edition (ICD-10). Both classifications utilize lists of behaviors to consider in the process of diagnosing hyperactive conditions. The main differences between DSM-IV and ICD-10 pertain to the concomitance of the 3 domains (inattention, hyperactivity, and impulsivity), the exclusion of co-morbidity, and the degree of pervasiveness. The ICD-10 criteria require a full set of symptoms in all 3 domains, whereas the DSM-IV recognizes 3 subtypes of the disorder – the predominantly inattentive type, the predominantly hyperactive-impulsive type, and the combined type. The results reported in our study are in line with that of another study, in terms of prevalence of ADHD subtype (combined more frequent, and inattentive followed by hyperactive less frequent) (18).
During the past decade, accumulated evidence has indicated that symptoms of ADHD persist into adulthood for 30% to 50% of children diagnosed with this disorder (27). ADHD is a chronic, debilitating disorder that may affect many aspects of an individual's life, including academic difficulties, social skills problems, and disturbances in parent-child relationship. Childhood psychiatric disorders can prevent a young person from reaching full potential by disrupting normal development. Prevention, detection, and treatment of ADHD are important not only to relieve current distress but also to improve adult functioning and to prevent the perpetuation of this disadvantage to subsequent generations of individuals. The management of ADHD typically involves psychotherapy or medications, and the evidence is strong for the effectiveness of behavioral treatments and pharmacotherapy. However, in the absence of adequate recognition of the disorder by the medical community, the teaching profession, and the public in general, children with ADHD are unlikely to receive the assistance they require to achieve full developmental potential at school, at home, and into adulthood. The main result purpose of this study was the identification of the epidemiological information for providing an estimation of the overall prevalence of disorder in a community.
Our findings have to be interpreted in the light of certain limitations. First, we did not analyze the negative predictive value of the screening test used, which could have been evaluated by including the children with negative result on K-RAS scale. Hence, the prevalence rate reported in our study may have been underestimated. Second, the study was carried out in elementary schools and did not include schools for children with special needs. As such, the results cannot be generalized to the whole childhood population of the country. Third, children from only 1 region of the country were included. Fourth, people of low socioeconomic status and those living in rural environments are both less likely to participate in research and to have higher rates of psychiatric illnesses. Even though we weighed the estimates for nonresponse, the effect of nonresponse might not be fully considered.
Despite the limitations, our study has added a new insight into the existing knowledge on ADHD prevalence. These results underline the importance of applying a screening methodology in schools, which could easily be applied to other mental disorders of childhood. Understanding the impact of ADHD in the general population may help clinicians to develop an adequate service, in terms of both psychological screening and treatments, and possibly to prevent the onset of other disorders in co-morbidity during a patient's lifespan.
 XML Download
XML Download