

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The prevalence of obesity has been continuously increasing worldwide over the last several decades, which raises concerns about the disease burden associated with obesity such as that of cardiovascular diseases (CVD) and cancers. Socioeconomic status (SES) has been suggested to be associated with obesity at an individual level as well as at a population level (1). However, the relationship between SES and obesity varied according to the developmental level of the society (12). The study conducted in countries with a high level of development showed that obesity was more prevalent in people with low SES, whereas obesity prevalence was higher in people with high SES in countries with medium to low levels of development (13). In low-income countries or in countries with low human development index (HDI), the association between SES and obesity appears to be positive for both men and women: the more affluent persons or those with higher educational attainment are more likely to be obese. Meanwhile, in middle-income countries or in countries with medium HDI, the association becomes largely mixed for men and mainly negative for women (4), and even inverse association is observed between SES and obesity prevalence in developed countries, especially for women (5).
Socioeconomic differential in obesity prevalence is an important issue of public health, in the aspect that it may cause a socioeconomic differential in the burden of obesity-related diseases. There have been studies on socioeconomic inequality in individual specific diseases that are associated with obesity (67). However, socioeconomic inequality in the overall disease burden associated with obesity has not been extensively evaluated. In addition, the trend of inequality in obesity-related disease burden along with the change in national-level socioeconomic development has been rarely evaluated.
The Korean population would be an appropriate study sample to address the issue because Korea has experienced rapid socioeconomic growth and increasing obesity prevalence over the last several decades (8). The HDI of Korea has increased from 0.64 in 1980 to 0.80 in 1995 and to 0.91 in 2010 (9). HDI is one of the widely used national-level indices of socioeconomic development calculated as a composite statistic of life expectancy, education, and income indices. A HDI of 0.8 or more represents “high development” and a HDI below 0.5 represents “low development” (10). In addition, obesity prevalence among Korean adult population has increased from 26.7% to 31.5% between 1998 and 2005 (8).
In this regard, this study aimed to evaluate the time trend in socioeconomic differentials in overall and specific obesity-related mortality over the last decade in Korean population.
MATERIALS AND METHODS
Death certificate data from the Statistics Korea and Korean Population and Housing Census (KPHC) data were used for this study. Individual information about sex, age at death, cause of death, and education level was obtained from death certificate data of the Statistics Korea for Koreans who died of obesity-related diseases at an age of 25–74 years in 2001, 2006, and 2011.
We defined obesity-related mortality as death from CVD, diabetes, or obesity-related cancers (111213) and identified them by International Classification of Disease-10 codes for causes of death: CVD as hypertensive or ischemic heart disease (I11, I13, I20–I25), heart failure (I50), cerebrovascular disease or stroke (I60–I69), atherosclerosis or peripheral vascular disease (I70), and aortic aneurysm (I71), diabetes mellitus as diabetes (E10–E14); and obesity-related cancers as colon and rectal cancer (C18–20), esophageal cancer (C15), kidney cancer (C64, C65), pancreatic cancer (C25), gallbladder cancer (C23), thyroid cancer (C73), endometrial cancer (C541), and female breast cancer (C50).
The KPHC is a nationwide survey conducted at 5-year interval since 1926 to understand the size, distribution, and structure, and the housing of all Koreans and foreigners residing in Korea. The size of population by age and education level in 2000, 2005, and 2010 extracted from the KPHC data were used as population denominators for calculating mortality rates in 2001, 2006, and 2011, respectively.
We selected education level as an individual SES indicator for the present study because information on income, social class, or wealth was not available in the death certificate data and less than 50% of Korean women were involved in economic activity. Education level was grouped into 4 categories: elementary school or less (≤ 6 years), middle school (7–9 years), high school (10–12 years), and college or higher (> 12 years).
We calculated direct age standardized mortality in 2001, 2006, and 2011, using the population in 2005 as the standard population. We assessed time trends in the age-standardized mortality rates by the Spearman rank correlation test.
We assessed the degree of socioeconomic inequality by estimating the relative index of inequality (RII) by education level using Poisson regression model. RII is the rate ratio of the mortality rates of those at the lowest education level compared with those at the highest education level and thus, often used to estimate socioeconomic inequality. A RII higher than 1 indicates that the mortality rate is higher in the group with lower education level, and thus, socioeconomic inequality exists. A larger RII indicates a more severe inequality (14). All the analyses were conducted with SAS version 9.3 (SAS Institute, Inc., Cary, NC, USA).
RESULTS
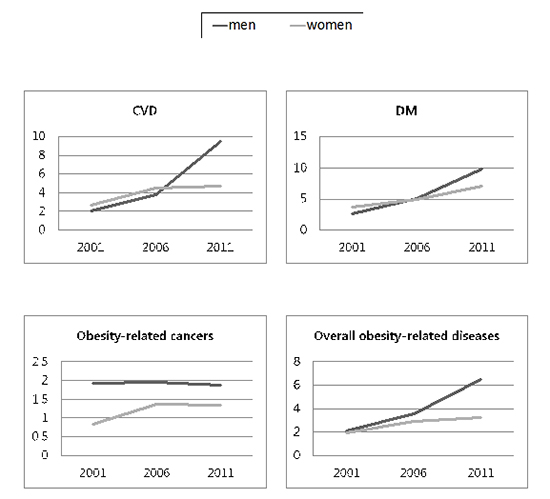
Table 1 shows the mortality rates for obesity-related diseases in overall and by education level. The mortality rates for overall and specific obesity-related diseases were persistently higher in men than in women, and tended to gradually decrease between 2001 and 2011 in both sexes, except for the obesity-related cancer mortality in women.
Table 1
Age-standardized obesity-related mortality per 100,000 persons* by education level in 2001, 2006, and 2011 in Koreans of 25–74 years of age

CVD = cardiovascular diseases.
*Direct age standardization was done, using the population in 2005 as the standard population. †CVD includes hypertensive or ischemic heart disease, heart failure, cerebrovascular disease or stroke, atherosclerosis or peripheral vascular disease, and aortic aneurysm; Obesity-related cancers include cancers at colon and rectum, esophagus, kidney, pancreas, gallbladder, and thyroid. For women, cancers at endometrium and breast were additionally included; Overall obesity-related mortality includes mortality from CVD, stroke, diabetes mellitus, and obesity-related cancers. ‡Percentage of mortality rate in 2011 compared to the mortality rate in 2001. §
P value for trend < 0.05, assessed by the Spearman rank correlation test.
The mortality rates for obesity-related diseases were higher in people with lower education level in all 3 years, except for obesity-related cancer mortality in women. Mortality rates for CVD and diabetes have gradually decreased between 2001 and 2011 in both sexes with all 4 education levels, except for men with the lowest education level. The mortality from obesity-related cancers in men tended to decrease over time in people with most education levels except for middle school education level, whereas the mortality from obesity-related cancers in women showed no consistent time trend by education level.
Table 2 shows the time trend in RII of obesity-related mortality by education level. The RIIs for mortality from CVD and diabetes in men and women were higher than 1 in 2001, which have gradually increased over time. The RII of mortality from obesity-related cancers in men was higher than 1 in 2001; however, it did not change significantly over time. On the other hand, the RII of mortality from obesity-related cancers in women was lower than 1 in 2001. However, it has turned to be higher than 1 in the year 2006, which persisted until 2011.
Table 2
Time trend between 2001 and 2011 in RII* (95% CIs) for obesity-related mortality by education level, in Koreans 25–74 years of age
RII = relative index of inequality, CIs = confidence intervals, CVD = cardiovascular diseases.
*Rate ratio of the mortality rates of those at the lowest education level compared with those at the highest education level. A RII higher than 1 indicates that the mortality rate is higher in the group with lower education level. †CVD includes hypertensive or ischemic heart disease, heart failure, cerebrovascular disease or stroke, atherosclerosis or peripheral vascular disease, and aortic aneurysm; Obesity-related cancers include cancers at colon and rectum, esophagus, kidney, pancreas, gallbladder, and thyroid. For women, cancers at endometrium and breast were additionally included; Obesity-related mortality includes mortality from CVD, diabetes mellitus, and obesity-related cancers. ‡Assessed by the Poisson regression test.
We estimated the time trend of RII between 2001 and 2011 of obesity-related mortality by education level in each 10-year age stratum (Table 3). The RII of mortality tended to be higher in younger people than those in older people, for all specific obesity-related diseases, in both men and women. The time trend of gradual increase in RII over time was evidently found for CVD mortality, consistently in both men and women across all age strata. However, for mortality from obesity-related cancers in men, the time trend in RII was not observed across all age strata. For mortality from diabetes, the RII has gradually increased in older people aged 45 years or more, while no time trend was found in younger people, in both men and women.
Table 3
Time trend between 2001 and 2011 in RII* for obesity-related mortality by education level in each 10-year of age strata, in Koreans 25–74 years of age

RII = relative index of inequality, CVD = cardiovascular diseases.
*Rate ratio of the mortality rates of those at the lowest education level compared with those at the highest education level. A RII higher than 1 indicates that the mortality rate is higher in the group with lower education level. †Cardiovascular disease includes hypertensive or ischemic heart disease, heart failure, cerebrovascular disease or stroke, atherosclerosis or peripheral vascular disease, and aortic aneurysm; Obesity-related cancers include cancers at colon and rectum, esophagus, kidney, pancreas, gallbladder, and thyroid. For women, cancers at endometrium and breast were additionally included; Obesity-related mortality includes mortality from cardiovascular disease, diabetes mellitus, and obesity-related cancers. ‡Assessed by the Poisson regression test.
DISCUSSION
In this Korean study, we found that a significant socioeconomic inequality has existed for obesity-related mortality in both men and women, especially in younger Koreans in spite that the mortality from these diseases has markedly decreased over the same time period. In addition, our study revealed that the socioeconomic inequality in some specific obesity-related mortality (CVD and diabetes) has gradually increased over the last decade in Korea.
In our study, the RII, which reflects socioeconomic disparity, was greater than 1 for all obesity-related diseases in both sexes throughout the whole study period. Even the RII of obesity-related cancer mortality in women that was once less than 1 in 2001 has increased to greater than 1.
Several studies in countries in various developmental stages have also found an inverse association between SES and mortality from specific obesity-related causes. For cardiovascular mortality, studies in low and middle income Asian countries (15), African country (16), and Latin America (17) have consistently found an inverse association with SES. An inverse association between SES and diabetes was also reported (618). The consistency in the findings of socioeconomic inequality in obesity-related mortality and morbidity between studies including our study strongly suggests that the obesity burden falls disproportionately on people with low SES and persons with lower SES were found to be at higher risk of death from CVD, diabetes, and obesity-related cancers compared to persons with higher SES.
Obesity results from an energy imbalance where caloric intake exceeds the energy expenditure by physical activity and metabolic processes in a body, which is influenced by complex interactions between genetic, metabolic, behavioral, cultural, and environmental factors including social networks and community ties (1920). Socioeconomic disparity in obesity and obesity-related diseases may stem from difference in calorie intake and physical activity across different SES (212223).
Interestingly, the direction of socioeconomic inequality in obesity-related mortality in the present study tends to be inconsistent with the direction of socioeconomic disparity in obesity prevalence. Although a Korean study conducted in a rural area in 2007 showed that the prevalence of obesity was higher in subjects with lower education level for both sexes (24), most studies in Korea reported that the direction of socioeconomic differential in obesity prevalence differed by sex (252627). A study using the data from Korean National Health and Nutrition Examination Survey (KNHANES) in 2010 reported that obesity prevalence was positively associated with both education level and family income for men, whereas an inverse association was found for women (26).
Time trend in socioeconomic disparity in obesity was scarcely studied with inconsistent findings. A study using KNHANES data between 1998 and 2007 also found different directions of time trend in socioeconomic inequality in obesity prevalence by sex: the RII of obesity prevalence by income level was lower than 1 until 2005 for men, while it was higher than 1 in women until 2007 (27). However, in the same study, the RII of obesity prevalence by education level did not show any significant trend from 1998 to 2007 (27). Another Korean study has evaluated a time trend in socioeconomic differentials by household income in obesity prevalence level between 1998 and 2010 and found that a positive association in men and an inverse association in women between obesity prevalence and SES have persisted or deepened over time (28). Therefore, there is a discrepancy in the time trend in socioeconomic inequality between obesity prevalence and obesity-related mortality.
We have considered several probable reasons for the discrepancy in socioeconomic differentials between obesity prevalence and obesity-related mortality. First, inequality in the control of related health risk factors could be considered. Kim et al. (25) reported that the positive association between body mass index and education level in men has attenuated, while the inverse association between body mass index and education level in women has become more evident, after adjusting for health-related behavioral factors such as smoking, alcohol use, and physical exercise. This finding suggests that socioeconomic differentials in lifestyle factors may intensify the socioeconomic differentials in obesity prevalence, and thus, result in greater socioeconomic differentials in obesity-related disease burden. Second, it has been suggested that quality of health care is worse in a person with lower education level (29). A study of Korean men found that the treatment rate for hypertension, 1 of the obesity-related diseases, was lower in men with lower education level compared to those with higher education level (30). Tamayo et al. (31) found that diabetic patients with higher SES are more likely to receive newer anti-hyperglycemic medication than those with lower SES in Germany. A Scottish study also reported that SES is associated with glycemic control, cardiovascular risk factors, and complication development in diabetes (18). Third, a discrepancy due to the time lag between the development of obesity and obesity related death may exist. For example, the data on the current obesity related death may reflect the obesity problem several years or several decades ago. A study in Cuba reported the finding compatible with this issue that the decrease in diabetes and cardiovascular mortality occurred about 5 years after the population-wide weight loss (32). However, our study could not address these issues due to the lack of individual information and lack of data over several decades.
In the present study, the educational inequality of obesity-related mortality was larger in younger people than in older people. We think this finding may reflect larger disparity across different educational groups in obesity prevalence, obesity-related disease, and the use of medical services, in younger people than in older people. Although we could not examine the hypothesis in the present study, several previous studies have reported supporting evidence. A study in Korean women found that the educational inequality in obesity prevalence was higher in younger people than that in middle agers (26). A similar pattern was observed in a study in Thailand (33) and United Sates (34). In addition, the association of obesity with diseases was found to decrease with aging (35), which might be explained by disease induced loss of weight in older people and higher premature death rate in low socioeconomic group. A study evaluated the trend in socioeconomic disparities of adolescent obesity in the USA found the disparity has gradually increased between 1998 and 2011, which may be reflected in greater disparity in obesity prevalence in younger people than in older people (36). Therefore, the findings of the present study may raise concerns regarding the possible aggravation of socioeconomic inequality in obesity-related mortality in the future, although more evidence over a longer period is needed. Although more evidence over a longer period is needed, the findings of the present study raise concerns regarding the possible aggravation of socioeconomic inequality in obesity related mortality in the future.
Interestingly, obesity-related cancer mortality rate in women has not materially decreased over the last decade. For women with the lowest education level, the obesity-related cancer mortality rate has rather increased. Increased mortality from breast cancer and endometrial cancer over the last decade in Korean women may explain the increase in obesity-related cancer mortality in women because breast cancer and endometrial cancer account for a substantial proportion of obesity related cancers (3738). In our previous study in Korean women, we found that mortality from breast cancer has increased between 2001 and 2011, especially in the women with lower education level with a gradual increase in the RII of breast cancer (37), which is consistent with the findings of the present study. When we considered the RII of each cancer that is known to be associated with obesity such as cancers of the esophagus, gallbladder, colon, and pancreas (Supplementary Table 1), no specific trend was found over time. Meanwhile, the obesity-related cancer mortality in men has decreased over the last decade in our study, which is consistent with the report by Statistics Korea which suggests that the overall age-adjusted cancer mortality in Korean men has decreased (39). However, the change was not so significant compared to CVD and diabetes mellitus. The RII of obesity-related cancers in men was persistently greater than 1, but it did not show any significant trend for change over time. When we considered the RII for each cancer in men (Supplementary Table 1), we found that the RII of colon cancer has gradually increased over time. Based on this finding, introducing screening for colon polyp and colonoscopic polypectomy, which is an active preventive strategy against colon cancer (40), can be considered because the high cost of screening colonoscopy can cause socioeconomic differentials in accessibility to the procedure.
Our study has some limitations. First, education level used as a SES indicator in our study might not be the best SES indicator. Second, we could not directly prove that obesity in a person with lower SES can lead to higher risk of obesity-related mortality compared to a person with a similar level of obesity but higher SES. Third, we did not consider the contribution of social patterning of lifestyle factors and other factors that can also be associated with the risk of obesity-related diseases.
In conclusion, a significant socioeconomic inequality in obesity-related mortality such as CVD, diabetes mellitus, and obesity-related cancers exists in Korean population. Despite the decreasing trend in obesity-related mortality over the last decade, the socioeconomic inequality in obesity-related mortality has persisted or gradually increased over the last decade. Given the increasing obesity prevalence, an active effort to identify the cause and to eliminate the socioeconomic gap in obesity-related diseases is needed.
 XML Download
XML Download