

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Between March and July of 2009, an emerging infectious disease characterized by acute severe fever and thrombocytopenia of unknown etiology was reported in the rural areas of Central China (1). The cause of this illness was identified in 2010, and defined as the severe fever with thrombocytopenia syndrome virus (SFTSV) by the China Center for Disease Control and Prevention (2). Outside of China, severe fever with thrombocytopenia syndrome (SFTS) cases were reported in Japan (3), South Korea (4), and the United States in 2012 (5). Recent surveillance data has shown an increasing incidence of SFTS, with widespread distribution of the SFTSV in Korea (6). This disease usually presents with fever, thrombocytopenia (platelet count < 100,000 per cubic millimeter of blood), and leukopenia, which often progress to multiple organ failure. SFTS has an average mortality rate of 7.3% to 16.0% (27), and up to 46.0% in a 2013 Korean study (8). The major risk group consists of those living in rural areas working as farmers, particularly elderly patients (median age of 58 years) (2). Thus, most previous studies have been based on adult data, with little pediatric data available. Through 2014, SFTS was diagnosed in 91 individuals in South Korea (9), but pediatric patients have not been reported and no clinical study on children has been performed. Here, we describe a pediatric case of SFTS, and the clinical characteristics and disease progression in children.
CASE DESCRIPTION
In mid-August, 2015, a 10-year old girl from Chonnam Province visited the hospital with myalgia and a history of fever over the previous 8 days. She spent time with the animals on her family farm (in a rural area), and her father noticed a tick on her head before the fever developed. Because the abrupt onset high fever and myalgia were not improved with medical care, her father consulted the community health center. The patient's blood and the tick were evaluated to determine if she suffered from a tick borne disease. In both the tick (Haemaphysalis longicornis) and the patient's blood sample, medium and small segment of the SFTS viral RNA was detected by reverse transcriptase-polymerase chain reaction. In addition, SFTSV was isolated from the tick. Based on these results, SFTSV infection was confirmed and patient was referred to a tertiary hospital. Her physical examination upon admission revealed a temperature of 36.1°C, pulse of 88 beats/min, respiration rate of 20/min, and blood pressure of 90/60 mmHg. Additionally, painless small lymph nodes were palpable in the neck. Although, she complained of severe myalgia, general weakness, and the inability to walk, no gastrointestinal or hemorrhagic symptoms were observed in the patient.
The laboratory tests revealed a white blood cell (WBC) count of 1.7 × 103/mm3, platelet count of 60 × 103/mm3, aspartate aminotransferase level of 224 U/L, lactate dehydrogenase level of 1,183 U/L, and creatine kinase level of 905 U/L. The coagulation profile, kidney function test, and urinalysis were non-specific. She was treated with a broad spectrum antibiotic, intravenous immunoglobulin (IVIG, 0.5 mg/kg/day for 2 days), dexamethasone (10 mg/m2/day), and ribavirin (400 mg/day).
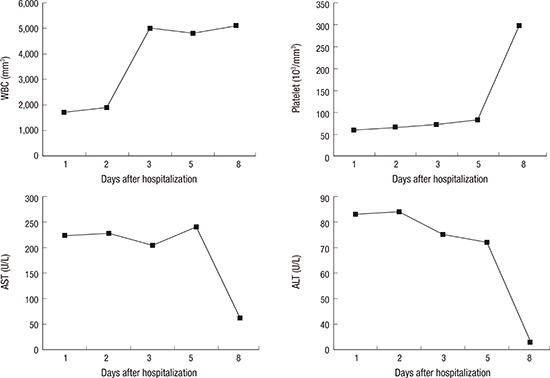
The general weakness and myalgia were relieved and her body temperature was normalized after the initiation of the treatment, and remained normal. After treatment, the patient was drowsy, but fully oriented and responsive. Because drowsiness could be a possible side effect of ribavirin, it was discontinued on the 6th day. Since then her mental state improved with no other neurological symptoms. Restoration of the WBC and platelet counts was observed 3 days and 8 days after hospitalization, respectively. The normalization of the other abnormal laboratory findings occurred over 5 to 8 days (Fig. 1). On the 9th day, patient was discharged with no medical problems, and she needed no further medication. At the 2-month follow-up, she remained healthy without sequelae.

DISCUSSION
In this article, we have described the first pediatric case of SFTS in Korea. Overall, the clinical manifestation appeared to be milder than in an adult case, and the patient was successfully treated with a combination of steroids, IVIG, and ribavirin. Results from several epidemiological investigations have indicated that SFTS patients are most often elderly individuals living in rural areas (81011). Most data are based on adult populations, and a very few pediatric SFTS cases have been documented (1213). Available data on pediatric patients indicate common symptoms of fever, leukopenia, throbocytopenia, and gastrointestinal symptoms. They did not exhibit any symptoms of dyspnea, consciousness disorder, dizziness, or hemorrhage (12). However, adult patients more frequently present with hemorrhage, central nervous system symptoms, or multiple organ dysfunction syndrome (81014). Among the pediatric cases, no death occurred and clinical course seemed to be milder than that in adults. For this reason, recognition of pediatric SFTS is more difficult than in adults solely based on clinical symptoms.
In order to diagnose SFTS, clinical suspicion based on symptoms and hematological abnormalities is critical along with history and inspection of the tick bite. A tick bite is not always evident, and a history of outdoor activity or contact with animals should be investigated. In the present case, the patient was bitten by a tick while she was playing with the animals on the farm. Hematologically, SFTS patients present with both thrombocytopenia and leukopenia. Previous studies on pediatric patients showed delayed onset and early recovery of thrombocytopenia compared to adult patients (1213). Of the 4 pediatric patients, 3 patients presented with delayed onset of thrombocytopenia (5 to 6 days after disease onset compared to 1 to 2 days for adults). In addition, thrombocytopenia reverted to normal earlier for pediatric patients than in adults (5 to 9 days vs. 10 days, respectively) (12). However, our patient's thrombocytopenia lasted more than 10 days. A study with a larger sample size should be conducted to determine if there are significant differences in onset and recovery of thrombocytopenia between pediatric and adult cases with SFTS.
As mentioned above, pediatric patients present vague symptoms and less aggressive clinical course (1213). The disease severity depends on multiple factors, including viral replication, access to the healthcare system, and the host's immune response, as well as other unknown reasons. Ding et al. (11) suggested that age was a critical risk factor for SFTS, because most hospitalized SFTS patients were elderly. Shin et al. (8) also found an association between age and prognosis, and those patients who died were older than the survivors (73.5 years vs. 61.0 years, respectively). The incomplete maturation of the immune system in children could pose a possible mechanism for milder disease manifestation (12). This mechanism has been previously reported to explain a milder clinical course for Crimean-Congo hemorrhagic fever in children than in adults (15). Difference in pro-inflammatory and anti-inflammatory cytokine networks in adults and children may be due to variation in host-dependent factors including genetic diversity or immunological response (15). Additionally, children often have easier access to the healthcare system.
Here, to the best of our knowledge, we report the first pediatric case of SFTS in Korea. Since SFTSV is endemic in Korea, close attention must be paid to the screening of children with mild symptoms consisting of SFTS.
 XML Download
XML Download