

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The role of intensive care has rapidly expanded over the last 20 years, and critical care staff is involved in the care of critically ill patients within the intensive care unit (ICU) and in general wards, and following discharge from the ICU (1). To prevent unexpected deaths and patient deterioration due to clinical errors, the rapid response system (RRS) was proposed to detect acutely deteriorating hospitalized patients and to provide timely interventions for these patients (2).
Potential criticisms of RRS are that these systems are labor intensive, and some hospitals may feel that they do not have the manpower to staff an RRS (3). However, several studies have shown that that these systems are necessary to reduce inpatient morbidity and mortality (34567). Considering patient safety and the potential costs associated with unexpected legal problems, the use of an RRS will likely extend further in worldwide medical systems.
However, no optimal composition for an RRS has been identified (8). The RRS has a number of different formats and names, including rapid response team, medical emergency team, and critical care outreach team, depending on its design. The RRS is often considered to function as a “moving ICU” because it has the ability to manage complex airway issues, establish central access, and initiate ICU-level care at patients' bedside (910).
Usually ICUs are often separated into medical and surgical disciplines because patients admitted to medical versus surgical services are different (11). Typically, patients admitted to medical services are more likely to be older and in a more critical condition than those admitted to surgical services (12). Therefore, activated patients in the RRS may present with different clinical features and need somewhat different support between medical and surgical services.
Therefore, we aimed to compare differences in the triggers and causes for RRS activation, interventions performed, and outcomes of patients admitted to medical and surgical services. We hypothesized that the triggers, causes for RRS activation, and interventions performed following this activation differ based on the patient population.
MATERIALS AND METHODS
Study design
This study was conducted at the Seoul National University Bundang Hospital, a tertiary care academic hospital that admits approximately 17,000 patients per year. Originally, our hospital has 906 beds with 2 specific ICUs (medical and surgical), and since March 2013, it has been expanded to 1,270 beds. The wards were moved to the new building from March 2013 to February 2014. The ICU was also expanded to 4 specific ICUs (i.e. medical, surgical, neurologic, and emergency). Annual ICU admissions are approximately 6,000 per year.
The RRS at our hospital was launched in October 2010. It is based on the electronic medical record (EMR) screening system and has 10 activation criteria (Supplementary Table 1). Patients deteriorating in general wards detected by RRS monitoring between October 2012 and February 2014 were included in this study.
We reviewed EMRs for the following clinical variables: age, sex, ward of admission, the modified early warning score (MEWS), triggers and causes of RRS activation, interventions performed by the RRS, patient disposition after intervention, the Acute Physiology and Chronic Health Evaluation (APACHE)-II score, the Sequential Organ Failure Assessment (SOFA) score, the reason for ICU admission, survival rate, and the number of sudden cardiac arrests during the period.
RRS design
Initially, the RRS was performed in the wards of general surgery and hemato-oncology. It was gradually expanded and all hospital wards have been monitored through our RRS since April 2013. The EMR-based RRS described in this study is operated through a dashboard monitoring system termed the ‘Bundang Excellent SMART Touch Board system (BESTBOARD)’ (13). The system has 10 types of activation criteria, including direct call by a healthcare worker in emergency situations (Supplementary Table 1). If an abnormal value (based on predefined criteria) is recorded in the EMR, this value and patients' identification are displayed as an alert on the dashboard monitor (13). A primary check is performed by a charge RRS nurse with > 5 years of ICU experience. If it is thought that the patient will require further work up and specific interventions, nurses will notify physicians to ensure proper patient management. The monitoring system is operated from 7 a.m. to 10 p.m. on weekdays and from 7 a.m. to 12 p.m. on Saturdays. The RRS team is composed of 4 experienced nurses and 11 physicians. From 7 a.m. to 6 p.m. on weekdays, 2 pulmonologists (intensivists who are in charge of the medical ICU) or 2 anesthesiologists (intensivists who are in charge of the surgical ICU) participate on a rotating duty system, and from 6 p.m. to 10 p.m. on weekdays and from 7 a.m. to 12 p.m. on Saturdays, 9 staff members (3 emergency physicians, 2 pulmonologists, 2 cardiologists, 1 hemato-oncologist, and 1 anesthesiologist) are on duty.
The definition of RRS activation in this study means that physicians intervened for alert-listed patients. Admission to the ICU via the RRS is primarily mediated by intensivists. Interventions performed by the RRS are triaged according to the A/B/C triage categories used by critical care response teams in Ontario (14). This system categorizes patients into the following 3 categories: A (Admit to ICU) includes patients admitted to the ICU; B (Borderline) includes patients who require further assessment (typically investigations or monitoring of their response to therapy); and C (Consultation only) includes patients who require assessment and recommendations that can be performed while remaining in their current location. We added category D (Do not resuscitate [DNR]), which includes patients whose DNR orders are initiated by the RRS team on the ward (13).
Statistical analysis
Categorical and continuous variables are expressed as numbers and percentages, and medians and interquartile ranges, respectively. Differences between medical and surgical services were tested by independent sample t-test and χ2 tests for continuous and categorical variables, respectively. Clinically significant variables were subject to multiple logistic regression analysis to determine the risk factors for mortality. All statistical analyses were performed using SPSS, version 17.0 (IBM SPSS Statistics, Armonk, NY, USA). A 2-tailed P value < 0.05 was considered significant.
Ethics statement
The present study protocol was reviewed and approved by the Institutional Review Board of Seoul National University Bundang Hospital (IRB No. L-2013-1232), which waived the requirement for informed consent because of the retrospective study design. The study was performed in accordance with the Declaration of Helsinki.
RESULTS
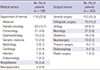
RRS was activated in 460 patients over the study period. Among 460 patients, 138 (30.0%) and 322 (70.0%) were admitted to the medical surgical services, respectively. The most common wards of RRS activation were general surgery for surgical services and the hemato-oncology unit for medical services (Table 1).
Table 1
Specific wards of RRS activation
![]()
The majority of RRS activations were triggered by abnormal screening values (blood pressure, heart rate, respiratory rate, body temperature, oxygenation, lactic acid levels, and blood gas analysis) or pain and neurological symptoms (72.6%, Table 2). Only 26.7% were triggered by direct calls. The number of direct calls from medical services was especially low (n = 20). The median response time was 5 minutes (Table 2).
Table 2
Clinical characteristic of patients with RRS activation

Values are presented as number of patients (%) or median (IQR).
RRS = rapid response system, IQR = interquartile range, MEWS = modified early warning score, BP = blood pressure, HR = heart rate, RR = respiratory rate, BT = body temperature, SaO2 = arterial oxygen saturation, PaCO2 = partial pressure of carbon dioxide.
*Systolic BP < 90 mmHg; †HR are < 50/min or > 140/min; ‡RR < 10/min, > 30/min, or stridor/accessary muscle use; §BT > 39°C or < 36°C; ∥SaO2 < 90% in room air or facial mask > O2 8 L/min; ¶PaCO2 > 50 mmHg, pH < 7.3, or PaO2 < 60 mmHg; **Lactic acid > 2.5 mM/L or TCO2 < 15 mM/L; ††any serious concern about deterioration.
![]()
Triggers for RRS activation significantly differed between the medical and surgical services (P = 0.001). They included an abnormal respiratory rate (23.2%), abnormal results on blood gas analysis (20.3%), and low blood pressure (18.8%) among patients in the medical services group; and low blood pressure (32.0%), low oxygen saturation (20.8%), and an abnormal heart rate (17.7%) among patients in the surgical services group (Table 2).
We found significant differences in the main causes for RRS activation between patient groups (Supplementary Table 2). More patients in the medical services group than in the surgical services group were distressed by respiratory problems (61.6% vs. 38.0%, P < 0.001), and patients in the surgical services group were more likely to experience cardiac problems and bleeding (16.4% vs. 8.5%, P = 0.035 and 8.8% vs. 2.5%, P = 0.024, respectively) than those in the medical services group.
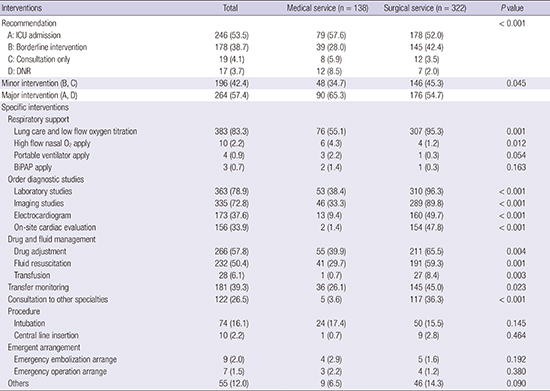
Then we evaluated interventions performed following RRS activation (Table 3). Overall, patients were more likely to be classified as DNR or required ICU admission in the medical group than those in the surgical group (65.3% vs. 54.7%, P = 0.045). Moreover, the time from RRS activation to DNR conversion was longer in the surgical group than that in the medical group (median 14 days vs. 4 days, P = 0.035; Table 4). Our analysis of individual interventions also yielded significant differences. Patients admitted to surgical services were more likely to undergo lung care with low-flow oxygen titration, various diagnostic studies, drug and fluid adjustment, consultation with other specialties, and transfer monitoring than patients admitted to medical services. In contrast, patients admitted to medical services were more frequently undergoing a trial of high-flow oxygen therapy and ventilation with a portable or non-invasive positive pressure device (Table 3).
Table 3
Interventions of RRS activation

Values are presented as number (%).
RRS = rapid response system, ICU = intensive care unit, DNR = do not resuscitate, BiPAP = Bi-level positive airway pressure.
![]()
Table 4
Outcomes of interventions performed after RRS activation
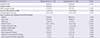
Values are presented as number of patients (%) or median (IQR).
DNR = Do Not Resuscitate, RRS = rapid response system, ICU = intensive care unit, SOFA = Sequential Organ Failure Assessment, APACHE-II = Acute Physiology and Chronic Health Evaluation-II, MV = mechanical ventilation.
![]()
Although the majority of patients were alive at hospital discharge in both groups, a higher number of patients were alive at discharge in the surgical group compared to those in the medical group (86.6% vs. 64.5%, P < 0.001). Among the outcomes of interventions performed after RRS activation, we observed similar rates of ICU admission between groups. However, significant differences in the SOFA and APACHE-II scores, intubation rate, and frequency of renal replacement therapy were found between groups (Table 4).
In multivariate analysis (logistic regression) for hospital mortality in RRS activated patients, whether the patient was admitted to medical services was found to be an independent risk of mortality in this patient group after adjusting for the MEWS, Charlson comorbidity index weighted for age, and intervention performed by the RRS team (Table 5).
Table 5
Prognostic factors for mortality in RRS activated patients
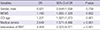
MEWS = modified early warning score, CCI-age = age adjusted Charlson comorbidity index, OR = odds ratio, CI = confidence interval.
*Major intervention (A, D) vs. minor intervention (B, C).
![]()
DISCUSSION
We observed significant differences between the medical and surgical patient groups in terms of the triggers and causes of RRS activation, interventions performed, and patients' outcomes following RRS activation. Common diagnoses resulting in RRS activation in our study were respiratory distress, sepsis, and cardiac problems; these findings are similar to those of previous studies (8151617). However, the 2 patient groups had significantly different clinical characteristics and intervention requirements. In contrast to patients admitted to medical services, in which RRS activation was triggered by respiratory problems in 60% of cases, sepsis and cardiac and bleeding problems were common triggers for RRS activation among patients admitted to surgical services.
These different causes of RRS activation are reflected in the differences in activation criteria and interventions performed in the 2 groups. We found that interventions performed in patients admitted to medical services were mainly support for high-grade respiratory care (e.g. high-flow oxygen therapy, portable ventilator and bi-level positive airway pressure use). In contrast, interventions performed in patients admitted to surgical services included diagnostic tests, drug adjustment, fluid management, and transfusions. In 2011, Sarani et al. (16) reported that triggers for RRS activation and interventions were similar between the medical and surgical patient groups. However, their study focused on the incidence of cardiac arrest and hospital mortality, whereas we assessed detailed differences in triggers, interventions, and causes for RRS activation between 2 patient groups. Therefore, our study suggests that an RRS structure tailored for specific patient groups may be needed.
The reason why these differences were observed is as follows. If an RRS alarm is alerted, our RRS nurse performs a check first and if the problem has not already been properly handled by the primary care physician who resides in the ward, our RRS is activated. In surgical service, most problems that occur during the perioperative periods need medical management such as infection (18), drug adjustment (1920), lung care (2122), etc. Generally, residents in the surgical ward resolve these problems after consulting with staff from medical departments (mainly infection, cardiology, and pulmonology). In this situation, the RRS team can provide rapid and proper interventions prior to receiving a response from the consultant. Therefore, minor interventions (B, C) are common in surgical services as shown in our results. Meanwhile, these kinds of problems have been commonly encountered by residents in medical wards, and most are solved by the primary care physician. Therefore, if the RRS is activated in the medical services, most cases are typically urgent and require major interventions such as high-grade respiratory support, ICU admission, or DNR discussion, according to our results.
It is necessary to re-establish specific thresholds for trigger criteria for specific patient groups to be able to apply these results to the clinical field. Our hospital uses constant trigger criteria for RRS activation and it has not been validated if the current criteria are appropriate. We determined the threshold levels of the trigger criteria based on our clinical practice and widely accepted values reported in previous studies (3152324). However, as shown in this study, different patient groups require more elaborate and specific trigger criteria and thresholds, as different patient groups are managed by different types of physicians. The capacities of these physicians in dealing with emergency situations differ greatly according to their department and experience. Therefore, optimal criteria and thresholds for RRS activation should be re-determined.
The RRS described in this study had 2 arms and was based on the admission of patients to either a medical or surgical service. The main concept of our RRS is a moving ICU. In addition, the lack of manpower devoted to full-time RRS is 1 of the main reasons for designing this system. We could not hire a new employee for the RRS due to poor administrative support, thus we made use of existing manpower. Physician notification following RRS activation differs depending on whether patients have been admitted to medical or surgical services. For patients admitted to medical services, 2 pulmonologists (intensivists who are in charge of the medical ICU) are the primary contact, whereas 2 anesthesiologists (intensivists who are in charge of the surgical ICU) are the primary contact for patients admitted to surgical services. Therefore, the potential benefits of this 2-arm system include greater physician familiarity with the primary care team, familiarity with patient problems and the anticipated clinical course, and the integration of common causes for patient deterioration in the system (16). Furthermore, rapid arrangement of ICU beds is possible and the continuity of treatment is preserved when patients are admitted to the ICU.
Our study has several limitations. First, it was a single center observational study. Since our findings reflect the experience of a single tertiary referral teaching hospital, they may not be generalizable to non-teaching or low-acuity hospitals. The 2-arm system of our hospital is advantageous as aforementioned, but there are no data to compare 2-arm systems with a single-arm system. A prospective study to compare the efficacy of these systems is needed. Second, the RRS in the study hospital was a part-time system. We do not conduct the screening system during the evening (10 p.m. to 7 a.m. on weekdays) and most of the time on weekends because resources are limited. However, instead of a screening system, we do conduct the RRS only via direct call during screening off time during the study period, and doctors on duty are intensivists and clinical fellows in the critical care division. Therefore, technically, there is an on-going RRS (direct call without screening and RRS nurses during the evening and weekends). Further analysis about the effect of this part-time system is needed. Third, the classification of the medical and surgical ward was somewhat irrelevant. Neurology was classified as the surgical ward in this study because of its proximity, as the neurologic ward and neurologic ICU are both located in the same building with the surgical ICU. Fourth, we did not analyze mortality data related to pre- and post-RRS implementation because this study focused on the different characteristics of RRS between the medical and surgical patient group.
In this study, we found that RRS triggers, patient outcomes, and interventions associated with RRS activation greatly differed between patients admitted to medical and surgical services. We suggest that future research evaluate the efficacy of an RRS approach that is tailored to specific patient groups.
 XML Download
XML Download