

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Otitis media (OM) is defined as inflammation of the middle ear and mastoid space, regardless of cause or pathogenesis (1). OM has the second highest incidence rate, after upper respiratory tract infection, in patients who visit otorhinolaryngology and pediatrics departments (2). Without appropriate treatment, OM may become chronic, resulting in various complications.
Acute otitis media (AOM) and otitis media with effusion (OME) are closely related clinical conditions. AOM represents an acute infective process, whereas OME is characterized by the presence of middle ear effusion in the absence of symptoms and signs of acute inflammation (3). In general, Eustachian tube dysfunction and bacterial infection have been found to be the most frequent causes of OM, making the selection of appropriate antibiotics important in its treatment. The recent overuse and misuse of antibiotics, however, has led to changes in the major pathogens causing OM and in their antibiotic sensitivity. Empirical antibiotic treatment of patients with antibiotic resistant bacteria may result in treatment failure or complications. Spontaneous otorrhea is a frequent complication of AOM and, when it occurs, the use of antibiotics is recommended. If OME persists after a 3-month period of watchful waiting, treatment with ventilation tubes may be considered (4).
The causes of inflammatory response in patients with OME have been difficult to identify, especially because OME is not characterized by symptoms and signs of acute inflammation expected during typical acute bacterial infections (5). Data on the microbiologic characteristics of patients with AOM presenting as spontaneous otorrhea are also limited.
Selecting appropriate antibiotics and preventing the development of antibiotic resistant bacteria are major goals in the primary treatment of patients with OME and AOM. Primary pathogens and their antibiotic sensitivities in patients diagnosed with AOM and OME may change over time. This multi-center study therefore evaluated changes over 5 years in principal pathogens and their antibiotic sensitivity in patients in Korea diagnosed with AOM or OME.
MATERIALS AND METHODS
Subjects
The study population consisted of 683 outpatients who visited 7 tertiary hospitals in Korea from January 2010 to May 2015 and were diagnosed with OM, based on the results of medical history taking and physical examination, including otoscopy, tympanometry, and pure tone audiometry. Patients were classified as having AOM or OME based on diagnostic results and clinical findings.
AOM was defined as inflammation of the middle ear, in which fluid in the middle ear was accompanied by acute onset of signs or symptoms of ear infection, including a bulging eardrum, usually accompanied by otalgia or a perforated eardrum and often with drainage of purulent otorrhea. OME was defined as fluid in the middle ear without acute signs or symptoms of ear infection. Otoscopy may reveal a translucent eardrum, but more frequently the eardrum is opaque. A translucent eardrum may be accompanied by a fluid-air level. Alternatively, the eardrum may be immobile, either retracted or bulging.
The 683 patients diagnosed with OM consisted of 379 males and 304 females, of mean age 30.3 ± 26.9 years. Of these patients, 122 (53 males and 69 females, mean age 30.1 ± 26.7 years) were diagnosed with AOM, and 561 (326 males and 235 females, mean age 30.5 ± 27.3 years) with OME (Table 1).
Table 1
Baseline demographic characteristics of OM patients and organisms isolated from middle ear effusion and otorrhea samples
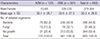
Values are presented as number (%).
OM = otitis media, AOM = acute otitis media, OME = otitis media with effusion, SD = standard deviation.
![]()
Sample collection, bacterial culture tests and antibiotic sensitivity tests
An otorrhea sample was collected from each patient with AOM on the first day of their hospital visit. Middle ear fluid was obtained after the bulk of the otorrhea fluid had been removed and the ear canal had been cleansed with a dry cotton swab. Under direct otoscopic visualization, the remaining discharge was collected, using an extra-thin flexible wire swab, from an area near the tympanic membrane or the perforation site of the tympanic membrane. Discharge or middle ear fluid samples were collected from patients with OME during middle ear surgery procedures, including ventilation tube insertion.
Each collected sample was added to Stuart transport medium and inoculated into blood agar and thioglycollate liquid medium. All cultures were incubated for at least 24 hours at 35ºC, and resultant bacteria were identified by Gram staining and biochemical tests. Antibiotic sensitivity tests were performed after bacterial identification, following the guidelines of the National Committee for Clinical Laboratory Standards (NCCLS) (6).
Gram-positive bacteria were tested for sensitivity to trimethoprim/sulfamethoxazole (TMP/SMX; SPT; co-trimoxazole), clindamycin (CL), penicillin (PC), erythromycin (EM), vancomycin (VAN), teicoplanin (TCP), tetracycline (TC), ciprofloxacin (CIP), linezolid (LZ), cefoxitin (CFT), rifampin (RFP), oxacillin (OX), and imipenem (IMP). Gram-negative bacteria were tested for sensitivity to TMP/SMX; SPT, CL, PC, EM, VAN, TCP, cefotaxime (CTX), piperacillin/tazobactam (PITA), cefepime (CFP), CIP, LZ, CFT, RFP, IMP, amikacin (AK), gentamicin (GM), aztreonam (AZM), ceftazidime (CAZ), piperacillin (PIP), tobramycin (TOB), and levofloxacin (LFX).
RESULTS
Bacterial detection rate and major isolated strains
Culture of ear fluid samples collected from the 683 patients showed the presence of bacteria in samples from 306 patients (44.8%) and fungi in samples from 33 patients (4.8%). In contrast, neither bacteria nor fungi were isolated from the samples of the remaining 344 patients (50.4%) (Table 1).
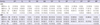
The most frequently isolated bacterial species was coagulase negative Staphylococcus aureus (CNS), present in 72 patients (23.5%), followed by methicillin-susceptible S. aureus (MSSA) from 50 (16.3%), methicillin-resistant S. aureus (MRSA) from 41 (13.4%), and Streptococcus pneumonia (SP) from 26 (8.49%). Of the 122 patients diagnosed with AOM, 76 (62.3%) were positive for bacteria and 15 (12.3%) for fungi, and 31 (25.4%) were negative for both (Table 1). CNS was isolated from 18 patients (23.7%), followed by MSSA from 13 (17.1%), MSSA from 13 (17.1%), SP from 12 (15.8%), and Pseudomonas aeruginosa (PA) from 6 (7.9%). Of the 561 patients diagnosed with OME, 230 (40.9%) had samples positive for bacteria and 18 (3.2%) for fungi, and 313 (55.8%) were negative for both (Table 1). CNS was isolated from 54 of these patients (23.5%), followed by MRSA from 38 (16.5%), MSSA from 37 (16.1%), and PA from 18 (7.82%) (Table 2).
Table 2
Bacteriological results of cultured and identified organisms

Values are presented as number (%).
AOM = acute otitis media, OME = otitis media with effusion, MRSA = methicillin-resistant Staphylococcus aureus, MSSA = methicillin-sensitive Staphylococcus aureus, CNS = coagulase negative Staphylococcus aureus,
![]()
Antibiotic sensitivity tests
Antibiotic sensitivity of Gram-positive bacteria
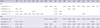
Most of the isolated staphylococci were classified as S. aureus (SA), including CNS, MSSA, and MRSA. All MRSA strains isolated from 41 patients were sensitive to VAN and TCP, whereas 90.2% were sensitive to co-trimoxazole. These strains, however, showed low sensitivity to other antibiotics, with 100% being resistant to PC, TC, CFT, and EM. Bacteria isolated from patients with AOM showed particularly low sensitivity to EM, CIP, and RFP.
More than 80% of the MSSA strains isolated from 48 patients were sensitive to TCP, VAN, and co-trimoxazole, CIP, LZ, and CFT.
About 85%–100% of the CNS strains isolated from 71 patients were sensitive to TCP, VAN, LZ, and co-trimoxazole, similar to findings for MSSA, with about 75% being sensitive to CL. In contrast 25%–60% of the isolated CNS strains were sensitive to other antibiotics, whereas ≥ 80% were resistant to PC and TC. Analysis of CNS strains according to OM subtype showed that sensitivity to most antibiotics was higher in strains isolated from patients with OME than with AOM. All SP strains isolated from 26 patients were sensitive to VAN and TCP, but showed low sensitivity to other antibiotics, in particular being resistant to SPT, CL, PC, and EM (Table3).
Table 3
Antibiotic susceptibility patterns of major gram-positive bacteria in OM
Values are presented as number (%).
OM = otitis media, SPT = trimethoprim/sulfamethoxazole (TMP/SMX, co-trimoxazole), CL = clindamycin, PC = penicillin, EM = erythromycin, VAN = vancomycin, TCP = teicoplanin, TC = tetracycline, CIP = ciprofloxacin, LZ = linezolid, CFT = cefoxitin, RFP = rifampin, IMP = imipenem, AOM = acute otitis media, OME = otitis media with effusion, MRSA = methicillin-resistant Staphylococcus aureus, MSSA = methicillin-sensitive Staphylococcus aureus, CNS = coagulase negative Staphylococcus aureus, SP = Streptococcus pneumoniae.
![]()
Antibiotic sensitivity of Gram-negative bacteria
PA strains isolated from 24 patients showed high sensitivity to PITA, IMP, and CAZ as well as relatively high sensitivity to CFP and PIP. These strains, however, showed low sensitivity to quinolone antibiotics, including CIP and LFX, and to aminoglycoside antibiotics. Haemophilus strains from 19 patients showed high sensitivity to CIP (80%) and TOB (80%), but low sensitivity to SPT (53.3%) and CL (33.3%) (Table 4).
Table 4
Antibiotic susceptibility patterns of major Gram-negative bacteria in OM
OM = otitis media, SPT = trimethoprim/sulfamethoxazole (TMP/SMX, co-trimoxazole), CL = clindamycin, PC = penicillin, EM = erythromycin, VAN = vancomycin, TCP = teicoplanin, CTX = cefotaxime, PITA = piperacillin/tazobactam, CFP = cefepime, CIP = ciprofloxacin, CFT = cefoxitin, IMP = imipenem, AK = amikacin, GM = gentamicin, AZM = aztreonam, CAZ = ceftazidime, PIP = piperacillin, TOB = tobramycin, LFX = levofloxascin, AOM = acute otitis media, OME = otitis media with effusion.
![]()
DISCUSSION
AOM is defined as all acute inflammatory states occurring in the middle ear cavity within 3 weeks of symptom onset. AOM that becomes chronic without drum perforation is described as progressing to OME, with ear fullness and hearing loss caused by drum retraction without erythema or otalgia. In most patients, however, inflammatory fluid remains inside the middle ear. The mechanism by which acute infection progresses to chronic inflammation remains unclear (6). As the primary causes of OM are Eustachian tube dysfunction and bacterial infection, many studies have investigated the primary pathogens in and the use of antibiotics to treat patients with OM. Due to the overuse and misuse of antibiotics in the treatment of various infectious diseases and the increasing frequency of antibiotic resistant bacteria, empirical antibiotic therapy may delay appropriate treatment regimens, causing secondary complications. Thus, If OM patients also have concurrent symptoms, particularly otorrhea, the otorrhea samples should be cultured to identify causative bacteria, with appropriate antibiotic therapy based on the results of antibiotic sensitivity testing.
Standard bacterial culture and sensitive molecular detection techniques have shown that the healthy middle ear is typically a sterile site (7). Bacterial isolation rates from patients with AOM have been found to range from 50% to 90%, but to be lower (21% to 70%) in patients with OME (8). Overall, we were able to isolate bacteria from 44.8% of the patients with OM. In addition to pathogenic bacteria, the normal flora always present in the external auditory canal (EAC) include Staphylococcus epidermidis, S. auricularis, S. capitis, and Corynebacterium (910). We found that the isolation rate of normal flora was low, whereas the isolation rates of pathogenic bacteria, including MSSA, MRSA, and PA, were high.
In this study, 18 (23.7%) patients with AOM and 54 (23.5%) with OME were positive for CNS. Contamination by bacteria present in the EAC may explain the high rate of detection of CNS in these middle ear effusion samples, but likely had no effect on the results for other strains. Differences in bacterial strains from previous studies may reflect a shift in the bacterial population toward more resistant isolates under antibiotic pressure, induced by the use of antibiotics prescribed at primary and secondary medical institutions (1112). These changes may also be caused by nosocomial infection by healthcare workers or medical instruments used during surgery and treatment.
CNS, Veillonella spp., and SA were found to be the 3 pathogens most frequently isolated from effusion fluid of patients with OME (5). Although long regarded as non-pathogenic commensals, CNS strains were shown to form biofilms, making them the leading cause of biomaterial-related infections (13). CNS have also been implicated in OM, with a recent study finding that they account for 60% of bacteria isolated from OME (14). Children with spontaneous otorrhea differ from those with uncomplicated AOM, in that the former is associated with S. pyogenes, which has shown greater local aggressiveness than other pathogens (15). Culture of middle ear fluid of children with otorrhea showed that 18% were positive for SA, with the presence of this bacterium regarded as the most significant microbiological characteristic of children with otorrhea (16).
Despite studies reporting that Moraxella catarrhalis, alone or in combination with other bacteria, was etiologic of AOM in a substantial number of children, this bacterium was cultured from only a small number of otorrhea samples, in agreement with previous findings (15). M. catarrhalis was reported to cause milder episodes of AOM than other etiologic agents, to be associated with significantly lower rates of spontaneous otorrhea at the time of diagnosis of AOM and to not cause severe complications such as mastoiditis. The low incidence in our patients of Moraxella strains may be related to the high sensitivity and decreased resistance of these organisms to most commonly used antibiotics.
Fungi are present in nature and are found as normal flora in the oral and nasal cavities. In a previous study the presence of fungal DNA in middle ear effusion was found to be associated with AOM and SOM in 34% of middle ear effusion samples. In our study, fungi were found in 12.3% of AOM patients and 32.1% of SOM patients, and may be thought to have an etiologic role. However, additional research is needed to clarify this issue (17).
Previous studies have shown that the major pathogens in patients with AOM and OME were SP, Haemophilus influenza, and M. catarrhalis, in that order. It is unclear why the percentages of samples in this study positive for these bacteria were lower. The prevalence of OME has been found to vary over time, and may be due to patterns of antibiotic use and/or vaccination, particularly following the introduction of vaccines against H. influenza type b and SP.
The organisms most frequently causing OM and bacterial resistance have been found to vary considerably over time and geographical region (Table 5). These differences among studies may be due, in part, to differences in inclusion criteria, sample sizes, microbiological methodology, climate, and geographical areas (5816192122).
Table 5
Studies of bacterial prevalence and antibiotic resistance in AOM and OME

| Study | Country | Mean age | Setting and inclusive years | No. of samples | Bacterial prevalence, % | Antibiotic resistance prevalence, % |
|---|---|---|---|---|---|---|
| AOM | ||||||
| Wasihun et al. (19) | Ethiopia | 21.9 ± 1.81 yr | Referral hospitals | 162 | SA (28.4) | SA (AMC 60.9, CIP 21) |
| Oct 2014–Jun 2015 | Proteus mirabilis (24.1) | Proteus mirabilis (CIP 0, CFO 35.9, AMC 88.9) | ||||
| Pseudomonas (16.7) | Pseudomonas (AMC 88.9, CFO 62.9, CIP 37) | |||||
| Marchisio et al. (20) | Italy | 28.3 ± 19.5 mon | Tertiary center | 705 | H. influezae (51.0) | H. influezae (AMP 11.8, CFO 0.9) |
| Jan 2001–Dec 2011 | SP (19.4) | SP (AMP 2.2, CFO 0 ) | ||||
| S. pyoienes (17.4) | S. pyogens (AMP 0, CFO 0) | |||||
| Brook et al. (16) | USA | 3.8 yr | Community outpatient clinics | 63 | SP (44.0) | - |
| Feb 2001–Mar 2006 | H. influezae (24.0) | |||||
| Moraxella (12.0) | ||||||
| MRSA (10.0) | ||||||
| Leibovitz et al. (15) | Israel | 15.8 ± 8.2 yr | Community clinics or pediatric emergency room | 822 | H. influezae (32.1) | - |
| 1996–2006 | SP (30.1) | |||||
| S. pyogenes (5.7) | ||||||
| OME | ||||||
| Daniel et al. (5) | UK | 4.5 yr | Tertiary center | 62 | CNS (12.9) | - |
| 2010–2011 | SA (9.7) | |||||
| SP (6.5) | ||||||
| Nasser et al. (21) | Lebanon | 4.2 ± 1.7 yr | Single University hospital | 107 | H. influezae (62.0) | H. influezae (AMC 81, cefalotin 61.9, CFT 19.0) |
| Jan 2009–April 2010 | SP (26.0) | SP (AMC 11.11, CFT 11.11) | ||||
| M. species (12.0) | ||||||
| Jung et al. (22) | Korea | 4.5 ± 2.2 yr | Tertiary center | 289 | CNS (11.4) | MRSA (CIP 41.7) |
| Mar 2004–Feb 2008 | MRSA (4.1) | MSSA (TC 45.5, CIP 45.5) | ||||
| Pseudomonas (4.1) | ||||||
| Poetker et al. (8) | USA | 23.9 mon | Referred center | 233 | Staphylococcus (16.3) | - |
| Feb 2002–Apr 2004 | H. influezae (10.3) | |||||
| Moraxella (6.4) |
AOM = acute otitis media, OME = otitis media with effusion, SA = Staphylococcus aureus, AMC = amoxicillin-clavulanate, CIP = ciprofloxacin, CFO = ceftriaxone, AMP = ampicillin, SP = S. pneumonia, MRSA = methicillin-resistant S. aureus, CNS = coagulase negative S. aureus, CFT = cefoxitin, MSSA = methicillin-susceptible S. aureus, TC = tetracycline.
![]()
The increased rates of inoculation with the conjugated heptavalent pneumococcal conjugate vaccine (PCV7) has reduced SP-associated morbidity in patients with AOM and OME, resulting in variations in bacteria causing OM (1618). We found that the isolation rate of SP was 6%–15%, significantly lower than that of MSSA, which was present in 17.1% of patients with AOM and 16.1% of patients with OME. In addition, the isolated MSSA strains showed ≥ 60% sensitivity to the antibiotics CL, LZ, CIP, TMP/SMX, VAN, and TCP. The isolation of SA and MRSA has recently increased in patients with spontaneously draining AOM (14), increases that may be due, at least in part, to the doubling since the 1990s of the amoxicillin dose administered to children (23).
Previous studies have recommended that patients with OM and concurrent otorrhea should be treated with empirical antibiotics, such as EM and amoxicillin, regardless of OM subtype (15), as these antibiotics were effective against SP, H. influenzae, M. catarrhalis, and PA, the main causes of OM. In addition, CIP and augmentin (amoxicillin-clavulanate) have been reported effective against various Gram-positive and Gram-negative bacteria that cause AOM (24). We found, however, that MSSA strains recently isolated from Korean patients with OM over the 5-year study period had different antibiotic sensitivity profiles. These findings indicate that the use of EM, amoxicillin, and CIP as primary empirical antibiotics in patients with OM should be reviewed.
The isolation rate of MRSA from patients with AOM over the 5-year study period was maintained at approximately 5%–7%. However, the detection rate of MRSA was higher in our patients with OME than in previous studies, suggesting that the chronic use of medications in patients with OME may increase the frequency of MRSA detection. These findings emphasize the importance of refraining from excess use of antibiotics in treating OME.
Treatment of ear infection caused by MRSA is challenging. As MRSA is resistant not only to methicillin but to other antibiotics, it cannot be effectively treated with conventional antibiotics alone (25). We found that, regardless of OM subtype, 100% of isolated MRSA strains were sensitive to VAN and TCP and 90% were sensitive to TMP/SMX, but < 10% were sensitive to other antibiotics. Antibiotics effective in treating MRSA give rise to more complications than antibiotics effective against MSSA, suggesting that the former may carry a higher risk of morbidities related to these complications (26). Thus, in treating patients with OM, it is important to select antibiotics with sufficient anti-microbial effect. The use of topical anti-infective agents in the treatment of purulent OM is of potential benefit, delivering a high concentration of drug to the site of infection and having a higher safety profile than systemic treatment (2728)
PA is hard to treat, as this species does not require a particular environment or nutrition to grow and is highly resistant to conventional antibiotics (24). In addition, PA strains from different individuals have different antibiotic sensitivity profiles, emphasizing the importance of simultaneous bacterial identification and antibiotic sensitivity testing to identify appropriate antibiotics. We found that ≥ 70% of isolated PA strains were sensitive to CFT, AK, AZM, and CAZ, but that these strains were resistant to GM, TOB, and quinolone antibiotics such as CIP and LFX. Thus, empirical antibiotics conventionally used to treat otorrhea are unlikely to achieve appropriate treatment outcomes in patients thought to have PA-caused otorrhea.
One limitation of this study was its reliance only on culture generated data. More specific techniques, such as PCR, may have resulted in a much higher identification rate of the bacteria associated with middle ear effusion, and provided a more accurate representation of the development of OM.
In conclusion, assessments of patients with AOM and OME showed that the most frequently isolated Gram-positive bacteria were CNS, MSSA and MRSA, whereas the most frequently isolated Gram-negative bacterium was PA. Analysis of changes in bacterial isolation rate by OM subtype and antibiotic sensitivity over the 5-year study period showed little change in the bacteria responsible for each OM subtype compared with earlier years. However, we found that the detection rate of MRSA in OME had increased. Alternative treatments, including topical procedures, should be applied before antibiotic use. The use of systemic antibiotics should be guided by culture and sensitivity tests.
 XML Download
XML Download