

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The most common cause of failure in glaucoma filtering surgery is scarring of the filtering bleb, and the increased amount of collagen in the surgical site suggests that proliferation of fibroblasts with associated production of collagen and glycosaminoglycans is important (1).
Mitomycin C (MMC) has enhanced the surgical success rate of trabeculectomy through inhibition of Tenon capsule fibroblast proliferation since its introduction in 1983 (2). However, use of MMC was associated with conjunctival epithelial damage, and it is characterized by non-healing leaking blebs and the risk of an avascular bleb and bleb infection (3). Hypotony maculopathy is one of the serious complications. It involves prolonged intraocular pressure (IOP) reduction associated with disc edema, vascular tortuosity, and chorioretinal macular folds, potentially producing marked reduction in visual acuity (1). The suggested causes are excessive filtering blebs and aqueous hyposecretion, i.e., ciliary body changes (4). In addition to these serious complications, corneal problems are still common (5). Pastor et al. (6) examined corneal endothelial cell densities in 10 patients who underwent trabeculectomies with MMC and found a 4.7% to 20.0% decrease in cell density.
Therefore, many agents that can modulate wound healing and are safe for other ocular tissues simultaneously have been tried. In a previous study, matrix metalloproteinase (MMP), particularly MMP-2/MT1-MMP, was associated with degradation of the extracellular matrix in the wound healing process after glaucoma filtration surgery and it was suggested as an important target for therapeutic intervention after glaucoma filtration surgery (7). In an animal study, Wong et al. (8) reported that MMP inhibitor can effectively reduce subconjunctival scarring after experimental glaucoma filtration surgery. In another study, the sequential treatment group used the following: Bevacizumab (Avastin), a monoclonal, VEGF antibody; Saratin, a 12 kD polypeptide with anti-inflammatory and anti-thrombotic properties; and Ilomastat, an MMP inhibitor. The study demonstrated a significant prolongation of bleb survival compared to the controls, which was not significantly different from the MMC positive control group (9). In another study, the MMP inhibitor significantly improved surgical outcomes compared with controls and the length of bleb survival was similar to the MMC group (10).
However, a MMP inhibitor used in previous studies was a nonspecific target agent; i.e., producing general inhibition on MMP. Also, there has been no study on the influence on other ocular tissues. Therefore, we evaluated the safety of a MMP inhibitor on other ocular tissues in an animal model.
MATERIALS AND METHODS
Fifteen New Zealand white rabbits aged between 12 and 14 weeks and weighing 2.0 to 2.5 kg were used.
Procedures and examination
Glaucoma filtration surgery was performed only on the right eye similarly to a previous report (11). Animals were randomly divided into 3 groups according to the adjuvant agent used during the surgery: the control group (n = 5), no agent; ilomastat-treated group (n = 5), 0.1 mL of 100 μM ilomastat (Calbiochem-Novabiochem, Nottingham, UK) in a subconjunctival injection; and MMC-treated group (n = 5), a thin cellulose sponge soaked with MMC (0.2 mg/mL). The bleb, conjunctiva, cornea, and anterior chamber were evaluated with slit lamp biomicroscopy and Seidel test preoperatively and at 7 days, 14 days, and 28 days postoperatively. A pachymeter (Ultrasonic pachymeter; Nidek, Aichi, Japan) was used preoperatively and at postoperative 28 days to check the central corneal thickness (CCT). Specular microscopy (Robo-Specular Microscope; Konan Medical Corporation, Nishinomiya, Japan) was performed preoperatively and 28 days postoperatively. At the postoperative 28th day, the rabbits in each group were sacrificed in a CO2 chamber after isoflurane gas induced anesthesia. The right eye of each rabbit was enucleated to preserve the bleb. Tissues were preserved in 10% formaldehyde, embedded in paraffin, and sequential 3–4 µm sections of the operative wound site were prepared. Hematoxylin and eosin staining was evaluated to check the general cellularity and inflammatory cells. Based on previous reports, the conjunctiva and the ciliary body toxicity were evaluated and scored according to the grading systems by 2 pathologists (12). The scale used for conjunctival changes was: 0 = no histologic change: no inflammation; 1 = minimal histologic change/conjunctiva epithelium preserved, thickening of the conjunctiva; 2 = mild histologic change/conjunctiva epithelium preserved, thickening of the conjunctiva, and mild inflammatory cell infiltration; 3 = moderate histologic change/score 2 with loss of collagen fibril organization; and 4 = severe histologic change: loss of the conjunctival epithelium, total disorganization, and necrosis of the underlying scleral stroma. The scale used for ciliary body changes was: 0 = no histologic change; 1 = minimal histologic change/ciliary epithelium height normal, demonstrating minimal fibroblast proliferation, congestion, and edema, no fibrin; 2 = mild histologic change/ciliary epithelium height decreased, demonstrating moderate fibroblast proliferation with fibrin, moderate congestion, and edema; 3 = moderate histologic change/score 2 with inflammatory cell infiltration; 4 = severe histologic change/desquamation of the ciliary epithelium, total disorganization, and necrosis of the ciliary body. The toxicity of the cornea was also assessed with light modifications.
For transmission electron microscopic observations, the cornea was obtained from the treated eyes immediately postmortem, and fixed in 2.5% glutaraldehyde in 0.1 M phosphate buffer for transmission electron microscopic examination. Afterwards, the specimens were postfixed in 1% osmium tetroxide solution, dehydrated and embedded in epoxy resin using the usual procedure. Ultrathin sections of approximately 60–70 nm thickness were made using an Ultracut-E Microtome (Reichert-Jung, Buffalo, NY, USA) and were stained with heavy metals, uranylacetate and lead citrate. Stained sections were assessed and photographed under transmission electron microscopy (TEM; H-7650; Hitachi, Tokyo, Japan).
Statistical analysis
Statistical analyses were conducted using IBM SPSS stastics version 24.0 (IBM Corp., Armonk, NY, USA). The means and standard errors were calculated using descriptive statistics. The Mann-Whitney U test and the Kruskal-Wallis test were used to compare the clinical findings of the groups. Significance was considered at P values < 0.05.
Ethics statement
This study was approved by the Institutional Animal Care and Use Committee of Ewha Medical Center(ESM15-0291). All animal procedures and methods used for securing the animal tissue complied with the Association for Research in Vision and Ophthalmology (ARVO) Statement for the Use of Animals in Ophthalmic and Vision Research and our institutional guidelines.
RESULTS
On postoperative day 7, 14, and 28, fluorescein slit lamp microscopic examination revealed no abnormalities in the bleb conjunctiva such as bleb leakage and blebitis in the ilomastat treated group, whereas one MMC treated eye showed one avascular cystic bleb. In the ilomastat-treated group, cornea problems such as keratitis and corneal ulcer were not noticed vis slit lamp examination. Any other adverse events, such as cataract, anterior chamber cell reaction, and endophthalmitis, were not found during the study.
The CCTs in each group are shown in Table 1. CCT was measured before surgery as follows: 377.0 ± 18.9 in controls, 382.00 ± 22.69 in the ilomastat-treated group and 372.40 ± 21.17 in the MMC-treated group. There was no significant difference among the groups (P = 0.756). On postoperative days, CCTs were 361.5 ± 10.6 in the control group, 384.0 ± 8.28 in the ilomastat-treated group, and 368.33 ± 21.12 in the MMC treated group and also showed no statistically significant changes among the 3 groups (P = 0.253). In the ilomastat-treated groups, there were no statistically significant changes in CCT between preoperative and postoperative 28 days (P = 0.655) and the MMC-treated groups also showed no significant change between preoperative and postoperative 28 days (P = 0.285; Table 1).
Table 1
Pachymetric result (µm)
![]()
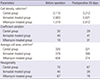
Specular microscopy findings, such as cell density, coefficient of variation, average cell area, and hexagonality for the 3 groups are shown in Fig. 1 and Table 2. In the ilomastat-treated group, the parameters on preoperative and postoperative 28 days were the following: cell density 2,683 and 2,621, coefficient of variation 40 and 41, average cell area 379 and 398, hexagonality 40 and 28, respectively (Table 2). In the ilomastat-treated group, there was no statistically significant difference in all parameters preoperatively and at postoperative 28 days (all P > 0.05). In the MMC-treated group, the coefficient of variation was changed from 19 preoperatively to 31 at postoperative 28 days. The average cell area also decreased from 659 to 374, and hexagonality changed from 67 to 78 in the MMC-treated group. However, when parameters were compared among the 3 groups preoperatively and at postoperative 28 days, there were no statistically significant differences in all parameters (all P > 0.05).
 | Fig. 1Specular microscopy of corneal endothelial cells of the rabbits on postoperative 28 days.
(A) Control group. (B) Ilomastat treated group. (C) Mitomycin-treated group. In the ilomastat-treated group, there was no statistically significant differences in all parameters preoperatively and at postoperative 28 days.
|
Table 2
Specular microscopic results
![]()
When conjunctival toxicity was evaluated, the average score was 1 in the control group, 1.5 in the ilomastat-treated group and 2 in the MMC-treated group. When assessing the ciliary body toxicity score, the ilomastat-treated group was 0.5 and the MMC-treated group was 1.5.
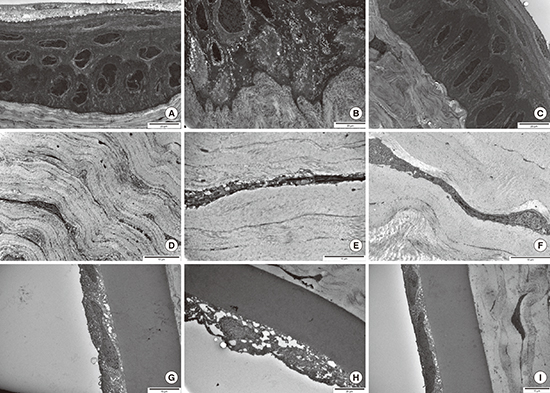
Electron micrographs of corneal structures are shown in Fig. 2. In MMC-treated eyes, variable-sized vacuoles were observed in the cytoplasm of epithelial cells and loss of junctional complexes were observed in basal cells. Multiple vacuoles were also observed in the cytoplasm of keratocyte corneal endothelial cells. In ilomastat-treated eyes, stratified squamous non-keratinized epithelial cells in the tear film were observed and normal long spindle shaped keratocytes were scattered among the lamellae of the stroma. A thick homogenous noncellular Descemet's membrane lined by a single endothelial cell layer was also noticed. In addition, any other adverse event, such as cataract formation, anterior chamber cell reaction, or endophthalmitis via slit lamp examination, were not found in the ilomastat treated group during the study.
 | Fig. 2Transmission electron microscopic view of cornea. (A, D, G) Control group. (B, E, H) Ilomastat-treated group. (C, F, I) Mitomycin-treated group. (A) The stratified squamous nonkeratinized epithelium resting on Bowman's membrane was noticed. Wing cells and basal low columnar cells with oval nuclei were observed. Interdigitation and junctional complexes at the lateral surface of basal epithelial cells were noticed. (B) Variable-sized vacuoles were observed in cytosplsm and loss of junctional complexes at lateral side was observed in basal cells. (C) Cellular integrity was maintained and surface damage or cellular desquamation resulting from toxicity was not observed. Microvilli on superficial cells were well preserved. (D) Normal long spindle shaped keratocyte are scattered among the lamellae of the stroma and the structures in the cytoplsam were well preserved. (E) Multiple vacuoles were observed in the cytoplasm of keratocyte. (F) A normal-looking spindle-shaped keratocyte was observed. Numerous well-preserved rough endoplasmic reticulum was noticed. (G) A thick homogenous noncellular Descemet's membrane lined by a single endothelial cell layer with a moderate electron-dense oval nucleus. (H) Intracytoplasimc multiple vacuoles are observed in corneal endothelial cell in MMC-treated group.
MMC = Mitomycin C.
|
DISCUSSION
Glaucoma is a progressive optic neuropathy that may cause blindness if not properly treated. Many glaucoma patients need glaucoma surgery during the treatment period and glaucoma filtration surgery is usually first attempted to control IOP (1314). However, the success rate of trabeculectomy is not perfect and many adjunctive antifibrotic agents to modulate the wound healing process of glaucoma filtration surgery have been tried (15). In addition, MMC is one of the most commonly used agents, but it is an antibiotic derived from Streptomyces caespitosus with alkylating properties that exert their most profound cellular toxicity in the late G1 and early S cellular phases (16). MMC can lead to the development of hypotony with a shallow chamber, hypotonic maculopathy, extended choroidal detachment, or a decrease in visual acuity related to progressive cataracts (17). During the many trials to find a more physiologic, alternative agent, a previous study reported that the healing response after surgery could be modulated by inhibiting the effects of MMPs in animal studies. However, a MMP inhibitor is a nonspecific target agent and we did not know the exact mechanism of modulating the wound healing process in filtration blebs. In addition, keratocytes are known to be quiescent in the normal cornea but are readily activated and transformed into myofibroblasts that express a-smooth muscle actin in response to various insults (18). Then myofibroblasts produce ECM, collagen-degrading enzymes, MMPs, and cytokines to compensate for the insults (18). If the MMP inhibitor could influence the cornea as with 5-fluorouracil or MMC, it could further disturb the physiologic compensation process of keratocytes. Therefore, we assessed the safety of the MMP inhibitor in glaucoma filtration surgery, especially the conjunctiva, cornea and ciliary body.
When assessing the corneal endothelium with specular microscopy, in MMC-treated group, the coefficient of variation was changed from 19 preoperatively to 31 at postoperative 28 days, the average cell area also decreased from 659 to 374, and hexagonality changed from 67 to 78. Electron micrograph of cornea microstructures showed intracytoplasmic multiple vacuoles in epithelial cells, keratocytes, and endothelial cells in the MMC-treated group. Loss of junctional complexes in epithelial layers was observed in the MMC-treated group. In previous human studies, Pastor et al. (6) reported a 4.7% to 20.0% decrease in corneal endothelial cells in 10 patients who underwent trabeculectomies with MMC. In other studies, the mean corneal endothelial cell loss following MMC augmented trabeculectomy was reported to be about 4% to 14% (19). Fukuchi et al. (20) published a report on 2 patients with moderate to severe guttata who underwent trabeculectomy with MMC. It is difficult to compare the exact results because of variation in the study subjects and methods. We used a relatively low dose (0.2 mg/mL) of MMC in a soaking irrigation method that may result in fewer microstructural changes than in previous studies. However, these results showed again that special caution is needed in MMC use regarding corneal microstructures, although there was no definite clinical corneal problem.
There were no adverse corneal problems in the ilomastat treated group via slit lamp microscopy. In the pachymetric results, there was no statistically significant change in the CCT between preoperative and postoperative 28 day measurements in the ilomastat-treated group (P = 0.655). In specular microscopic assessments, there were no significant changes in the endothelial cell density, coefficient of variation, average cell area, and hexagonality between preoperative and postoperative 28 day measurements. Through transmission electron micrographs, in the ilomastat-treated group, cellular integrity was maintained and surface damage or cellular desquamation resulting from toxicity was not observed in the epithelial layers and there was no evident abnormal change in keratocytes and endothelial cells.
In assessing conjunctival toxicity, the conjunctiva epithelium was preserved and minimal histologic changes were found in the ilomastat-treated group compared to the conjunctival changes of the MMC-treated group. Slit lamp microscopic examination revealed no abnormalities in bleb conjunctiva such as bleb leakage and blebitis in the ilomastat treated group, whereas one MMC treated eye showed one avascular cystic bleb. An in vivo study showed MMP inhibition significantly reduced matrix contraction and production without Tenon's capsule fibroblast toxicity (21). Similar to our study, Martorana et al. (9) also reported that less thinning of tissues and avascularity were noted in the ilomastat-treated group compared to the MMC group.
Regarding the ciliary body toxicity scores, the ilomastat-treated group was 0.5 and the MMC-treated group was 1. Previous studies have shown that episcleral MMC damages the ciliary body, and another study reported that a 5-minute exposure of MMC (0.2 mg/mL, 0.1 mL) in rabbit eyes caused the nonpigmented epithelial cells of the ciliary body to become swollen, and the intracellular abundant mitochondria were swollen and vacuolized (22). Many studies have been conducted to adjust the concentration and application duration of the drug due to the toxic effects of MMC (23). We used MMC (0.2 mg/mL) soaking for 2 minutes in blebs and found mild histologic changes, congestion and edema in the ciliary body. However, the ilomastat-treated group showed less histologic changes compared with the MMC-treated group.
There were some limitations in this study. First, our study was performed in a rabbit model and it is hard to apply our results clinically considering the proliferative capacity of the rabbit endothelium. Second, the number of rabbit eyes used in our study was too low, so there are some limitations in statistical analysis. Therefore, larger scale cases will be needed to confirm the safety of the drug. Third, the authors did not demonstrate drug levels in the ocular tissues. However, the 0.2 mg/mL MMC injection procedure was reported to result in higher conjunctiva, sclera, and aqueous body concentrations and there has been no report on ilomastat intraocular concentrations (24). Forth, we applied a single injection of the MMP inhibitor, so the toxic effect of the drug may have been underestimated whereas previous studies used multiple injections (8910). Finally, we did not assess the long-term potential toxic effects of the drug.
In conclusion, a single subconjunctival injection of a MMP inhibitor in experimental trabeculectomy showed a less toxic effect on the rabbit corneas, conjunctiva and ciliary bodies compared to MMC. However, the toxicity in human use may be different and more detailed long term studies are needed to confirm the safety of the drug.
 XML Download
XML Download