

 PDF
PDF ePub
ePub Citation
Citation Print
Print




INTRODUCTION
Vitamin D plays an important role in calcium and phosphate homeostasis and normal mineralization of bone (1). In addition, recent data have demonstrated that vitamin D is related to many urological diseases, such as male lower urinary tract symptoms and benign prostatic hyperplasia (2), erectile dysfunction (3), and urological cancer (4). There is also evidence that pelvic floor diseases such as urinary incontinence (UI) are related to low vitamin D levels (56). However, data from other study groups are still scarce. Therefore, we evaluated the relationship between UI and vitamin D using nationally representative data from Korea.
MATERIALS AND METHODS
Study subjects
Data from the Korea National Health and Nutrition Examination Survey (KNHANES) IV were used in this study. The KNHANES has been performed by the Korea Centers for Disease Control and Prevention to examine the general health and nutritional status of Koreans. A stratified 3-stage clustered probability design (local district → enumeration district → household) was used so that representative data for Koreans could be obtained. Four surveys have been completed: KNHANES I (1998), KNHANES II (2001), KNHANES III (2005), KNHANES IV (2007–2009), KNHANES V (2010–2012), and KNHANES VI (2013–2014). KNHANES IV enrolled 31,705 individuals, of whom 24,871 participated in the survey (response rate: 78.4%). Among those who participated in the survey between February 2008 and December 2009, serum 25-hydroxyvitamin D (25[OH]D) levels were obtained so that the vitamin D status of the general population in South Korea could be determined. To elucidate the relationship between UI and serum 25(OH)D levels, we excluded KNHANES IV participants whose serum 25(OH)D levels were not evaluated (n = 5,329; i.e., those who participated in the survey between January 2007 and January 2008). Data from males (n = 9,213) and subjects less than 20 years old (n = 2,577) were also excluded. In addition, subjects with missing data regarding UI (n = 355), menopause (n = 646), pregnancy history (n = 22), body mass index (BMI) (n = 18), hypertension (n = 11), and diabetes mellitus (n = 204) were excluded. Women who were currently pregnant (n = 45) were also excluded. Ultimately, 6,451 women were included in this study.
Evaluation of UI
The condition of current UI was established if a woman answered ‘yes’ to the following question. “Do you have current UI?”
Potential confounders
Age, obesity, lung disease (chronic cough), gravidity, hypertension, and menopause are known to be risk factors for stress UI in women (7891011). The KNHANES IV did not include data about gravidity, so we replaced gravidity with the number of pregnancies. The number of pregnancies was also a risk factor for UI in our data (see Table 1). Additionally, diabetes mellitus (12) and stroke (13) are risk factors for UI resulting from neurogenic bladder. Therefore, we used these factors for propensity score matching.
Table 1
Characteristics of participants before and after propensity score matching
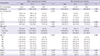
Values are presented as number (%).
UI = urinary incontinence, HTN = hypertension, DM = diabetes mellitus, BMI = body mass index, COPD = chronic obstructive pulmonary disease.
![]()
Obesity was determined based on the BMI (weight/height2, kg/m2), and subjects were categorized as underweight (BMI < 18.5), normal weight (BMI 18.5–22.9), or overweight (BMI > 22.9) according to World Health Organization Western Pacific Region suggested revised Asia-Pacific criteria. Lung disease (chronic cough) was defined as the presence of current asthma or chronic obstructive pulmonary disease (COPD). Hypertension was defined as systolic blood pressure ≥ 140 mmHg, diastolic pressure ≥ 90 mmHg, or use of antihypertensive medication. Diabetes mellitus was defined as fasting blood glucose ≥ 126 mg/dL, or use of antidiabetic medication, or insulin. Stroke was defined as a history of stroke or current presence of stroke.
Vitamin D measurement
Serum 25(OH)D levels were measured with a gamma counter (1470 Wizard, PerkinElmer, Finland) with an RIA (Dia-Sorin, Still Water, MN, USA). The intra- and inter-assay coefficients of variation were 2.9%–5.5% and 6.3%–12.9%, respectively. Vitamin D insufficiency was categorized as < 20 ng/mL, 20–30 ng/mL, and > 30 ng/mL according to previous data (14).
Statistical analysis
Demographic data were analyzed with descriptive statistics. The significance of differences in these estimates was analyzed with a χ2 test for categorical variables.
The propensity score was built by means of a multivariable logistic regression model considering the following variables: menopause, number of pregnancies, hypertension, diabetes, BMI, age group, stroke, asthma, and COPD. Propensity score matching was considered for 558 UI patients and 5,893 control patients, but ultimately, propensity scores were matched at a 2:1 ratio of controls to UI patients (n = 1,116 controls and 558 UI patients). We performed propensity score matching with the MatchIt package in the R statistical package, and implemented the suggestions of Ho and colleagues for improving parametric statistical models by preprocessing data with nonparametric matching methods.
All tests were 2-sided, with statistical significance set at P < 0.05. Analyses were conducted with the R statistical package v.2.13.1 (R Foundation for Statistical Computing, Vienna, Austria).
Ethics statement
The study was carried out in agreement with the applicable laws and regulations, good clinical practices, and ethical principles as described in the Declaration of Helsinki. The Institutional Review Board of National Police Hospital reviewed and approved this study protocol (approval number: 11100176-201611-HR-010). Informed consent was waived by the board.
RESULTS
Table 1 displays the demographic data before and after propensity score matching for the UI cases and normal controls. Overall, the study included 558 UI cases and 5,938 normal controls, but following propensity score matching, there were 558 UI cases and 1,116 normal controls. Before propensity score matching, the rates of menopause, hypertension, diabetes mellitus, and asthma were significantly greater in the UI group. Additionally, participants in the UI group were significantly more likely to be older and obese and to have a higher number of pregnancies. After propensity score matching, age, menopause status, number of pregnancies, hypertension, diabetes mellitus, BMI grade, stroke, asthma, and COPD were evenly dispersed and did not differ significantly between the groups, therefore validating the propensity score matching model.
Table 2 displays vitamin D levels according to the presence of UI, before and after propensity score matching. Before matching, vitamin D levels were significantly higher in the UI case group. However, there was no significant difference in the mean vitamin D levels after matching. Additionally, there was no difference in the distribution of vitamin D levels (> 30, 20–30, < 20 ng/mL) between the groups after matching.
Table 2
Vitamin D level according to the presence of UI, before and after propensity score matching

Values are presented as number (%) of participants.
UI = urinary incontinence.
*Mean (standard deviation).
![]()
DISCUSSION
The aim of this study was to evaluate the relationship between vitamin D levels and female UI. In this study, vitamin D levels were higher in women with UI in univariate analysis. However, there was no significant relationship between vitamin D levels and UI after propensity score matching. When other stratification methods for vitamin D levels were used, such as 20 ng/mL, 30 ng/mL, or quartile ranges of the population, there was no relation between UI and vitamin D levels in a preliminary study (data not shown). The adjustment factors we used in matching (menopause, number of pregnancies, hypertension, diabetes, BMI, age group, stroke, asthma, and COPD) would have been confounders in determining the relationship between UI and vitamin D levels. Therefore, failure to account for these confounders would have altered the results before and after matching. Ultimately, our data revealed that low vitamin D levels were not significantly and independently related to female UI in this study. Our results differed from the results of previous clinical studies.
Nationally representative data from the United States (including 1,881 women) showed that those with UI were significantly more likely to have vitamin D levels less than 30 ng/mL (17.2% vs. 9.8%) (5). However, the adjusted odds ratio for UI was not associated with vitamin D levels in that cohort (adjusted odds ratio (aOR), 0.70; 95% confidence interval (CI), 0.45–1.08; P = 0.098) (5). Nevertheless, sub-group analysis revealed that the odds ratio for UI was significantly lower in women 50 years old and older with vitamin D levels of 30 ng/mL or higher (aOR, 0.55; 95% CI, 0.34–0.91; P = 0.022) (5). Another retrospective study from the United States (including 394 women) demonstrated that women with a pelvic floor disorder (defined as having at least one of the following diagnoses: stress UI, urge UI, fecal incontinence, or pelvic organ prolapse) had significantly lower levels of vitamin D than women in the normal healthy control group (vitamin D: 29.3 ± 11.5 vs. 35.0 ± 14.1 ng/mL, P < 0.001) (6). Additionally, Incontinence Impact Questionnaire-7 scores were higher among women with vitamin D insufficiency (questionnaire score 28.8 ± 26.8 vs. 42.4 ± 30.2, P = 0.001), and higher Incontinence Impact Questionnaire-7 scores were independently associated with vitamin D insufficiency (P < 0.001) (6).
The aforementioned nationally representative studies from the United States (5) included relatively small cohorts and did not adjust for menopause, which is known to be a key risk factor in stress UI (1516). Vitamin D deficiency is a risk factor for premature ovarian failure (early menopause) (17), and menopause is a risk factor for UI (1516). Therefore, not adjusting for menopause was a major limitation of the previous study. Additionally, the previous data were not adjusted for common risk factors for UI, such as hypertension, diabetes, stroke, asthma, and COPD (18). The second set of evidence from a retrospective study in the United States (6) also had limitations, such as a small number of participants, retrospective chart review, data from one clinic (not nationally representative data), and lack of specific data regarding UI (i.e., general data regarding pelvic floor disorders including UI, fecal incontinence, or pelvic organ prolapse). Therefore, we think that there is a lack of evidence to support the relationship between low vitamin D levels and UI from a clinical perspective.
From a pathophysiologic perspective, vitamin D is thought to affect UI in females by various pathways. An immunohistological study indicated that the 1,25-dihydroxy vitamin D3 receptor was expressed in human skeletal muscle (data from intraoperative periarticular muscle biopsies taken from 20 female patients who had undergone hip or back surgery) (19). Additionally, a double-blind randomized control study of 122 elderly women (mean age, 85.3 years; range, 63–99 years) in long-stay geriatric care demonstrated that musculoskeletal function improved significantly in the group that received 1,200 mg calcium plus 800 IU cholecalciferol (vitamin D) relative to the group that only received calcium (20). Therefore, it has been hypothesized that a low vitamin D level might promote the development of UI by causing pelvic floor muscle weakness. Specifically, pelvic floor muscle weakness may prevent incontinent women from efficiently closing the urethra during times of increased intraabdominal pressure, resulting in stress UI (6).
However, the expression of the 1,25-dihydroxy vitamin D3 receptor differs according to the muscle site (biopsies of hip patients had significantly fewer receptor-positive nuclei than those of back surgery patients (Mann-Whitney U-test: P = 0.0025) (19). In fact, another report indicated that the vitamin D receptor was undetectable in human skeletal, cardiac, and smooth muscle (21). Additionally, there is no data to identity vitamin D receptor in pelvic floor muscle. These factors suggest that the expression of the 1,25-dihydroxy vitamin D3 receptor may be very small or absent in pelvic floor muscle. Furthermore, the study showing that musculoskeletal function improved following the administration of vitamin D did not include pelvic floor muscle. Therefore, the hypothesis that vitamin D is related pelvic floor muscle function remains to be confirmed.
A second possible pathophysiologic explanation for a relationship between vitamin D and UI is that vitamin D insufficiency may affect the detrusor wall and thus contribute to symptoms of overactive bladder and urge UI (6). In data from human and rat bladders, receptors for vitamin D were identified in both the urothelium and the smooth muscle of the detrusor wall (22). In addition, 2 cases of resolution of urge UI with high-dose vitamin D supplementation were reported (23). However, there have been no experimental data showing the relationship between low vitamin D levels and bladder instability in urodynamic studies, which is the core evidence needed to confirm the relationship between urge UI and vitamin D; rather, studies have merely reported the presence of receptors for vitamin D. Additionally, there have been many limitations to the clinical data demonstrating that vitamin D supplementation improved urge UI, such as study design flaws (no placebo group, small number of cases, and no double-blinding), lack of follow-up studies, and failure to use the standardized clinical measurement of urge UI for outcome measurements. Therefore, we think that there is lack of evidence to support the relationship between low vitamin D levels and UI from a pathophysiologic perspective.
The present study had several limitations. First, the nature of our dataset makes causal inferences problematic. Second, we could not study the subtypes of UI, as this information was not available. Nevertheless, we think that our study provided meaningful results, as the dataset was the largest one used so far, and we used propensity score matching analysis to evaluate the relationship between vitamin D levels and UI.
In conclusion, low serum vitamin D is not significantly and independently related to female UI after propensity score matching in representative Korean data. Further studies will be needed to confirm our results.
 XML Download
XML Download