

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The outcome of childhood acute lymphoblastic leukemia (ALL) has considerably improved during recent decades (1234). Nonetheless, approximately 20% of childhood ALL patients relapse during or after frontline treatment (5). In particular, the outcome of bone marrow (BM) relapse of pediatric ALL is very poor, and relapsed ALL is one of the major causes of childhood cancer death (56). Challenges in the treatment of marrow-relapsed ALL include failure to achieve second complete remission (CR2), risk of induction death, and short-sustained second remission during post-remission treatment (578). Thus, an initial step to improve the outcome of marrow-relapsed ALL is the development of a more effective and safe reinduction platform.
Reinduction therapy usually consists of a 4-week regimen of prednisone, vincristine, L-asparaginase, and an anthracycline. Idarubicin is a second-generation anthracycline that has been effectively used to treat acute myeloid leukemia and relapsed ALL (91011). The maximum tolerated dose of idarubicin is reported to be 12.5 mg/m2/dose (9). The Children's Cancer Group (CCG)-1884 study reported that a weekly dose of idarubicin at 12.5 mg/m2 for 3 weeks could be effectively incorporated into reinduction regimens, with a requirement for intensive supportive care for serious hematopoietic toxicity (10). However, a previous Korean pilot study showed that 12.5 mg/m2/week of idarubicin was unacceptably toxic and had an inferior CR2 rate to a modified dose of 10 mg/m2/week due to a higher toxic death rate (12).
Based on the previous pilot study, the Childhood Acute Lymphoblastic Leukemia (CALL)-0603 study sought to improve the CR2 rate by reducing toxic death during a reinduction attempt with a modified dose of idarubicin and to evaluate the long-term outcomes of Korean children with relapsed ALL, thereby providing baseline data for future trials.
MATERIALS AND METHODS
Patients
Between 2006 and 2009, the multicenter, prospective CALL-0603 study enrolled children and adolescents aged from 1 to 21 years with a first isolated or combined marrow-relapsed ALL. Patients with B-precursor and T-cell ALL were included, whereas those with mature B-cell ALL and Down syndrome were excluded. Patients who had undergone prior allogeneic hematopoietic stem cell transplantation (HSCT) were eligible.
Definitions
BM relapse was defined as BM showing greater than 25% blasts (M3) by microscopic morphological examination. Central nervous system (CNS) relapse was defined as a cerebrospinal fluid white blood cell (WBC) count greater than 5/μL with lymphoblasts present on cytology or clinical signs of CNS disease. Testicular relapse was confirmed by open-wedge biopsy. Involvement of any other extramedullary site was confirmed histologically. Early and late marrow relapses were defined as relapse less than 24 months and ≥ 24 months after initial diagnosis, respectively. The risk groups at initial diagnosis were stratified based on age and WBC count at diagnosis and cytogenetic aberrations: standard risk as age ≥ 1 year and < 10 years with an initial WBC count < 50,000/μL, high risk as age < 1 year or ≥ 10 years and/or an initial WBC count ≥ 50,000/μL, and the presence of t(9;22)(q34;q11), mixed lineage leukemia (MLL) rearrangements, or hypodiploidy (< 45 chromosomes) irrespective of age and WBC count. Cytogenetic findings were divided into 4 groups: favorable (high hyperdiploidy [> 50 chromosomes] and t(12;21)(q23;p13)), unfavorable (t(9;22)(q34;q11), MLL rearrangements, and hypodiploidy), others, and normal karyotype.
Treatment plan
The reinduction protocol consisted of oral prednisolone 60 mg/m2/day for 28 days, weekly intravenous vincristine 1.5 mg/m2, intramuscular L-asparaginase 6,000 IU/m2 3 times weekly with a total of nine doses, and weekly intravenous idarubicin 10 mg/m2 on days 0, 7, 14, and 21. If the absolute neutrophil count (ANC) was < 500/μL or the platelet count was < 50,000/μL on day 14 or 21, idarubicin administration was withdrawn. However, if BM examination on day 14 showed M3 marrow, idarubicin was administered regardless of the blood cell count. CNS-negative patients received intrathecal cytarabine and hydrocortisone on days 0, 7, and 28, whereas CNS-positive patients received intrathecal triple therapy containing cytarabine, hydrocortisone, and methotrexate on days 0, 7, 14, 21, and 28.
If the day 29 BM was 5% to 25% blasts (M2) or M3, patients proceeded immediately to consolidation chemotherapy at the physician's discretion. The aim of this trial was to evaluate the efficacy and safety of reinduction treatment. Thus, post-induction consolidation regimens were based on institutional preferences, and the investigators decided between maintenance with chemotherapy or allogeneic HSCT to their discretion.
Assessment of treatment response and toxicities
BM examinations were done on days 7, 14 (if not less than 5% blasts [M1] at day 7), and 28 of reinduction treatment. Rapid early response (RER) was defined as an M1 marrow on day 7 (< 5% lymphoblasts) and CR on day 28 or an M2 marrow (5%–25% lymphoblasts) on day 7 and an M1 marrow on day 14 and CR on day 28. Slow early response (SER) was defined as an M2 or M3 (> 25% lymphoblasts) marrow on day 14 and CR on day 28 or an M3 marrow on day 7 and CR on day 28. CR2 was defined as an M1 marrow with no evidence of circulating blasts or extramedullary disease and with peripheral blood cell count recovery (ANC ≥ 750/μL and platelet count ≥ 75,000/μL).
Toxicities were graded based on the National Cancer Institute's Common Terminology Criteria for Adverse Events (CTCAE v4.0; National Cancer Institute, Bethesda, MD, USA).
Statistical methods
The primary objective of this study was to assess the efficacy and toxicity of a reinduction regimen, which were represented by CR2 rate and induction death rate. A CR2 rate of 75% (95% confidence interval, 60–90) was considered sufficient to warrant further study of this reinduction regimen. According to this design, it was necessary to recruit 36 patients. The secondary objective of this study is to assess the 5-year event-free survival (EFS) and overall survival (OS) of the enrolled patients.
A χ2 test was used to identify factors associated with CR. EFS was defined as the time between relapse and the first event (either relapse or death in CR). OS was defined as the time between relapse and death from any cause. The Kaplan-Meier method was used to estimate survival probabilities, and a log-rank test was used to test the prognostic significance of various risk factors. A P value < 0.05 was considered statistically significant. All statistical analyses were performed using SPSS version 21.0 (Statistical Package for the Social Sciences; IBM Corp., Armonk, NY, USA).
RESULTS
Patient characteristics
A total of 44 patients (31 males and 13 females) from 6 institutions (19 from Asan Medical Center Children's Hospital, 13 from Seoul National University Children's Hospital, 9 from Samsung Medical Center, 1 from National Cancer Center, 1 from Ajou University Hospital, 1 from Pusan National University Hospital) were enrolled in the trial. Demographic and clinical characteristics are summarized in Table 1. The median ages at initial diagnosis and relapse were 8.0 years (range, 1.1–15.8) and 11.5 years (range, 1.5–18.7), respectively. The median duration from initial diagnosis to relapse was 22.0 months (range, 2.0–107.0). Twenty-four patients relapsed less than 24 months after initial diagnosis (early relapsers) and 17 relapsed after more than 24 months (late relapsers). Thirty-four patients had isolated BM relapses, whereas 10 had combined BM and extramedullary relapses. At initial diagnosis, 17 patients had been allocated to the standard risk group, and 27 to the high-risk group. In addition, 35 patients had precursor B-cell leukemia and 9 had T-cell leukemia; 9 had favorable cytogenetic aberrations, 6 unfavorable, and 29 had normal karyotype or other aberrations. Six patients had received allogeneic HSCT in the first CR before relapse.
Table 1
Patient characteristics and treatments

CR = complete remission, EFS = event-free survival, OS = overall survival, BM = bone marrow, CNS = central nervous system, LNs = lymph nodes, CR1 = first complete remission, HSCT = hematopoietic stem cell transplantation, RER = rapid early response, SER = slow early response, NA = not available.
*NA indicates the patients whose BM data on day 7 and/or day 14 were not available.
Outcome of reinduction treatment
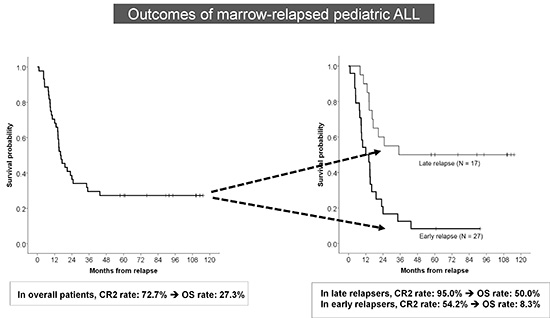
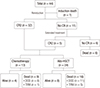
Overview of treatment and outcome regarding 44 patients with relapsed ALL is depicted in Fig. 1. Among 44 patients, 43 completed 4 weeks of reinduction treatment, and 1 died during reinduction therapy. The CR2 rate after 4 weeks of reinduction therapy was 72.7% (32 of 44 patients). Five patients achieved remission with extended treatment, resulting in a final CR2 rate of 84.1% (37/44). Among 43 patients who completed 4 weeks of reinduction treatment, 38 patients had available BM data on day 7 and/or day 14, thus could be designated according to their early morphological marrow responses to treatment as follows: 28.9% RER (11/38), 39.5% SER (15/38), and 31.6% induction failure (12/38).
Fig. 1
Overview of treatment and outcome regarding 44 patients with relapsed ALL.
ALL = acute lymphoblastic leukemia, CR = complete remission, CR2 = second complete remission, DOD = died of disease, TRM = treatment-related mortality, HSCT = hematopoietic stem cell transplantation.
Regarding dosage, 19 patients received 20 mg/m2 of idarubicin, 22 patients 30 mg/m2, and 3 patients 40 mg/m2. The median dose of idarubicin was 30 mg/m2. Patients who received 30 mg/m2 or more of idarubicin included significantly more patients with M3 marrow on day 14 than those who received 20 mg/m2 of idarubicin (27.8% vs. 0.0%, P = 0.038). Factors associated with successful CR2 induction are listed in Table 1. There was no significant difference in the CR2 rate between idarubicin doses of 20 mg/m2 and 30 mg/m2 or more (70.0% vs. 75.0%, P = 0.736). Time from initial diagnosis to relapse less than 24 months was a significant predictor of failure to achieve CR2 (P = 0.002). Site of relapse, age at relapse, risk group allocation at initial diagnosis, and cytogenetic aberrations were not significantly associated with the probability of achieving CR2.
Hematological toxicities were as follows: grade 3–4 neutropenia in 100.0%, anemia in 68.1% (30/44), and thrombocytopenia in 90.9% (40/44). Non-hematological toxicities were as follows: grade 3–4 transaminase elevation in 11.3% (5/44), hyperbilirubinemia in 4.5% (2/44), hyperglycemia in 13.6% (6/44), mucositis in 10.0% (4/44), and pancreatitis in 4.5% (2/44). Of the 44 patients, 33 (75.0%) developed neutropenic fever during reinduction treatment: 9 developed documented bacteremia, 8 had documented or presumed fungal infection, 4 had viral infection, and 12 had no identifiable source of infection. One patient died due to septic shock during reinduction treatment, resulting in an induction death rate of 2.3%.
Outcome of post-induction treatment
Among the 37 patients who achieved CR2, 13 (5 early relapsers and 8 late relapsers) continued consolidation and maintenance treatment with chemotherapy: 4 patients remained in remission, 8 subsequently relapsed and died of progressive disease, and 1 died in remission due to treatment-related complications. The remaining 24 patients (12 early relapsers and 12 late relapsers) proceeded to allogeneic HSCT in CR2: 8 remained in remission, 11 subsequently relapsed and died of disease, and 5 died of a transplant-related cause in remission. Of the 6 patients who did not achieve CR2, 5 patients continued chemotherapy and 1 patient received allogeneic HSCT in the refractory state; all died of progressive disease.
At a median follow-up duration of 99 months, the 5-year EFS and OS rates were 22.2% ± 6.4% and 27.3% ± 6.7% for all patients, 4.2% ± 4.1% and 8.3% ± 5.6% for early relapsers, and 43.8% ± 11.4% and 50.0% ± 11.2% for late relapsers, respectively (P = 0.001) (Fig. 2). Early time point of relapse and SER to reinduction chemotherapy were significantly related to poor EFS rates (Table 1). Notably, early response during reinduction treatment was a significant prognostic factor for late relapsers (RER vs. SER vs. induction failure = 100.0% vs. 33.3% ± 15.7% vs. 0.0%, P < 0.001), but it was not significant for early relapsers (RER vs. SER vs. induction failure = 20.0% ± 17.9% vs. 0.0% vs. 0.0%, P = 0.113) (Fig. 3).
Fig. 2
Survival of children with ALL. (A) OS and EFS in children with first BM relapse. Thick solid line = OS; dashed line = EFS. (B) EFS according to timing of relapse. Thick solid line = early relapse (< 24 months from initial diagnosis); thin solid line = late relapse (≥ 24 months from initial diagnosis).
ALL = acute lymphoblastic leukemia, OS = overall survival, EFS = event-free survival, BM = bone marrow.

Fig. 3
EFS based on timing of relapse and post-remission treatment. (A) EFS of all patients who achieved CR2 according to post-remission treatment. EFS of patients with (B) early relapse and (C) late relapse who achieved CR2 according to post-remission treatment. Thick solid line = chemotherapy; thin solid line = allogeneic HSCT.
EFS = event-free survival, CR2 = second complete remission, HSCT = hematopoietic stem cell transplantation.

EFS rates were not different between patients who received chemotherapy or allogeneic HSCT as a consolidative treatment (20.5% ± 12.0% vs. 29.2% ± 9.3%, P = 0.354). For early relapsers (n = 17) who achieved CR2, the EFS rates of patients who received chemotherapy or allogeneic HSCT were significantly different (0.0% vs. 8.3% ± 8.0%, P = 0.003), while those for late relapsers (n = 20) were not (50.0% ± 17.7% vs. 50.0% ± 14.4%, P = 0.649) (Fig. 4).
Fig. 4
EFS based on timing of relapse and early response to reinduction chemotherapy. (A) EFS of all patients with available data according to early response to reinduction chemotherapy. EFS of patients with (B) early relapse and (C) late relapse with available data according to early response to reinduction chemotherapy. Thick solid line = RER; thin solid line =SER; dashed line = induction failure.
EFS = event-free survival, RER = rapid early response, SER = slow early response.

DISCUSSION
The aim of our present study was to evaluate the efficacy and safety of reinduction chemotherapy with a modified dose of idarubicin. This regimen showed a 72.7% CR2 rate, which were within expected range to warrant further study. Especially, the CR2 rate was favorable for late relapsers, while suboptimal for early relapsers. From a toxicity standpoint, this regimen was tolerable to most patients with 2.3% of induction death rate. Toxicities were mostly hematological, and infections during neutropenia were treatable in most patients. The results suggest that a reinduction regimen with modified-dose idarubicin can be a safe and effective strategy to achieve CR2 in Korean children and adolescents with late marrow-relapsed ALL. However, the long-term survival outcomes were still poor, especially for early relapsers, emphasizing the need for a more effective reinduction regimen and post-remission treatment.
The CR2 rates of children with marrow-relapsed ALL reportedly range from 50% to > 90%, depending on the time point of relapse. Previous studies reported that the CR2 rate was < 50% in very early relapse, 70%–85% in early relapse, and > 90% in late relapse (810131415161718). One of the major obstacles to CR2 is toxic death during remission induction therapy; its reported incidence ranges from 4% to 10% (10141519).
Anthracycline is a key component of the reinduction regimen for relapsed ALL. However, the optimal anthracycline and its dose remain controversial and have been evaluated in previous studies (91012). The CCG-1884 trial reported that the reinduction rate was similar for idarubicin and daunorubicin groups and that a higher dose of idarubicin (12.5 mg/m2/week for 3 weeks) resulted in better early EFS than daunorubicin and lower-dose idarubicin (10 mg/m2/week for 3 weeks) (10). However, a previous Korean study showed that high-dose idarubicin (12.5 mg/m2/week) led to a high toxic death rate of 44% and poor CR2 rate of 22%, suggesting that high-dose idarubicin might be unacceptably toxic for Korean children with relapsed ALL (12). Thus, the present trial chose the lower dose of idarubicin (10 mg/m2/week), which was adjusted based on myelosuppression during reinduction treatment and ranged from a total idarubicin dose of 20 mg/m2 to 40 mg/m2. Of the 44 patients, 20 (45.4%) received a total idarubicin dose of 20 mg/m2; these patients showed a comparable CR2 rate to higher-dose idarubicin with a low toxic death rate. The overall CR2 rate of the present study is comparable to those of previous studies (1014152021). Notably, most of the late relapsers achieved CR2. However, the CR2 rate of early relapsers was unsatisfactory. Moreover, the long-term outcomes of the patients who achieved CR2 were poor, especially early relapsers. Thus, the reinduction regimen can be stratified based on the time point of relapse, such as a less toxic regimen for late relapsers to decrease toxic death during reinduction treatment and a more effective regimen for early relapsers to improve the CR2 rate.
A recent trial showed that mitoxantrone (10 mg/m2 on days 1, 2), an anthracenedione agent, had a significant benefit in reducing disease-related events, compared to idarubicin (10 mg/m2 on days 1, 2) in marrow-relapsed ALL (17) and CNS-relapsed ALL (22). Thus, the incorporation of mitoxantrone into reinduction regimens could be considered in a future trial. In addition, recent immunotherapeutic approaches such as a bispecific T-cell engager or a chimeric antigen receptor T-cell therapy has been reported to be promising for relapsed/refractory ALL (2324).
Because post-remission chemotherapy has been unsatisfactory in enabling sustainable second remission, allogeneic HSCT has been used as an intensive consolidation element for post-remission treatment (212526). However, the beneficial role and indications of allogeneic HSCT for relapsed ALL remain unclear. Previous studies suggested that patients with early BM relapse or those with BM relapse at any time of T-ALL can be considered to be indicated for allogeneic HSCT (25262728). However, its indication remains controversial for those with late BM relapse (252627). This study was to evaluate a reinduction regimen, and not intended to prospectively evaluate the role of post-remission therapy. The choice of post-remission therapy was to physician's discretion in this study. The differences in post-remission therapy in the present study do not always reflect the investigator's intention-to-treat. The patients who proceeded to allogeneic HSCT would have more durable remission, whereas those with short-lived second remission would not be eligible for allogeneic HSCT. Thus, the impact of allogeneic HSCT on the outcomes in this study was simply observational, with limited implications.
Another important prognostic factor in the present study was early response to reinduction chemotherapy. Notably, all late relapsers who showed a RER remained in remission with or without allogeneic HSCT, whereas the outcome was universally poor regardless of the early response in early relapsers. This suggests that the treatment response can be a guideline to consolidative treatment. Our study did not incorporate more sensitive method to detect minimal residual disease (MRD) into the protocol. MRD has been reported to be a significant prognostic factor for both newly diagnosed and relapsed ALL (293031). A recent study showed that a faster acquisition of MRD negativity was associated with a better outcome in relapsed ALL (32). Thus, future trials should evaluate the treatment response with measurements of MRD, which can predict the outcome more precisely.
Interestingly, our present study showed that a higher dose of idarubicin trended to be associated with poor outcomes. This could be because idarubicin was designed to be administered to patients who showed M3 marrow on day 14, regardless of the blood cell count. Thus, poor responders were likely to receive a higher dose of idarubicin. Actually, all the patients with M3 marrow on day 14 received 30 mg/m2 or more of idarubicin. This suggests that dose intensification during reinduction treatment cannot improve the long-term outcome of poor responders.
The aim of our present study was to evaluate the reinduction chemotherapy. Thus, our study had a limited ability to evaluate the role of post-remission therapy, and the impact of post-remission treatment might have suffered from a selection bias. In addition, because patients were subdivided into late and early relapsers, the assessment of prognostic factors in each subgroup was limited by a small number of patients.
In conclusion, this study showed a favorable CR2 rate due to reduced toxicity during reinduction treatment of marrow-relapsed pediatric ALL. The CR2 rate of late relapsers was excellent, whereas that of early relapsers was unsatisfactory. Thus, a more effective induction treatment involving new agents should be considered for early relapsers. In addition, CR2 achievement was not translated into sustained remission in most patients. Thus, future trials are required to optimize the post-induction treatment and improve the long-term outcomes.
 XML Download
XML Download