

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Multidrug-resistant tuberculosis (MDR-TB), defined as TB that is resistant to at least isoniazid (INH) and rifampicin (RFP), is difficult to treat. The global treatment success rate of MDR-TB remains at approximately 50% (1). Appropriate regimen design based on drug resistance patterns is crucial for improving treatment outcomes (2). Detailed information on additional drug resistance is essential to build an effective MDR-TB treatment regimen; however, such data are scarce in Korea.
Recently there has been much progress in the field of MDR-TB (3), such as the introduction of rapid molecular drug susceptibility tests (DST) and the availability of new anti-TB drugs (bedaquiline and delamanid) and effective repurposed drugs (linezolid and clofazimine). In addition, a shorter MDR-TB treatment regimen has been proven effective in several cohorts (4-6), which has shown a high reproducibility.
Reflecting on these advances, the World Health Organization (WHO) has recently released updated guidelines for the treatment of MDR-TB (7), which include the introduction of a shorter MDR-TB treatment regimen, and new recommendations on the existing conventional regimen. One of these 2 treatment strategies needs to be selected for the treatment of MDR-TB among patients in Korea. In this context, we asked several questions as follows: 1) Is the shorter treatment regimen feasible in Korea?, 2) Is the conventional regimen likely effective in Korea?, and 3) How many patients would benefit from including these new drugs at treatment initiation? To find an optimized strategy for MDR-TB treatment in Korea, we conducted a retrospective, multicenter study for the analysis of additional drug resistance patterns among MDR-TB patients.
MATERIALS AND METHODS
Study design and data collection
We included patients who were diagnosed with MDR-TB, on the basis of the results from phenotypic DST between January 2010 and December 2014, at 7 university-affiliated tertiary care hospitals in Busan, Ulsan, and Gyeongsangnam-do in Korea. We retrospectively reviewed the medical records of these patients, and the following data were collected: age, sex, history of previous TB treatment, type of specimen, and results of phenotypic DST.
We excluded duplicated patients in-hospital or inter-hospital, by checking each patient's name, gender, and birth date. If a patient had more than 1 DST result, we selected the earlier result. If the patient had DST results for both pulmonary and extra-pulmonary specimens, we selected the results for the pulmonary specimen.
DST
For the DST, 6 hospitals sent Mycobacterium tuberculosis isolates to the Korean Institute of Tuberculosis, and 1 hospital sent them to the Green Cross Reference Laboratory. Workflows used and references of critical concentrations for resistance were the same in both the laboratories. The drug susceptibility of the M. tuberculosis isolates was determined by the absolute concentration method with Lowenstein-Jensen medium. The drugs and their critical concentrations for resistance were as follows: INH 0.2 μg/mL, RFP 40 μg/mL, ethambutol (EMB) 2.0 μg/mL, rifabutin (RFB) 20 μg/mL, streptomycin (SM) 10 μg/mL, amikacin (AMK) 40 μg/mL, kanamycin (KM) 40 μg/mL, capreomycin (CM) 40 μg/mL, ofloxacin (OFX) 2.0 μg/mL, levofloxacin (LFX) 2.0 μg/mL, moxifloxacin (MFX) 2.0 μg/mL, prothionamide (PTH) 40 μg/mL, cycloserine (CS) 30 μg/mL, and para-aminosalicylic acid (PAS) 1.0 μg/mL. Pyrazinamide (PZA) susceptibility was determined by a pyrazinamidase test.
Definitions
MDR-TB was defined as resistance to at least both INH and RFP; Extensively drug resistant TB (XDR-TB) was defined as resistance to any fluoroquinolone (FQ) and at least one of three second-line injectable drugs (SLID) (CM, KM, or AMK), in addition to MDR; Pre-XDR-TB was defined as resistance to either a FQ or any SLID but not both, in addition to MDR. Patients were classified into the following groups according to their TB treatment history: 1) New patients with no history of TB treatment, 2) Patients previously treated with first-line drugs only, or 3) Patients previously treated with second-line drugs. Treatment history was defined as treatment with anti-TB drugs for ≥ 30 days.
Statistical analysis
Data are presented as mean ± standard deviation for continuous variables, and as numbers (with percentages) for categorical variables. Continuous variables were compared using the independent samples t-test, and categorical variables were compared using the Pearson's χ2 test or Fisher's exact test. To evaluate the trends in annual drug resistance, the χ2 test for trend was performed. All tests were 2-tailed, and P < 0.05 indicated statistical significance. Statistical analysis was performed using SPSS Statistics, Version 17.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Patients' characteristics
A total of 5,599 culture-confirmed TB patients were included, of which 378 (6.8%) showed M. tuberculosis isolates with MDR. Baseline characteristics of the 378 MDR-TB patients are shown in Table 1. Their mean age was 47.8 years and 242 (64.0%) of them were men. Of 378 MDR-TB patients, 216 (57.1%) were new patients, 125 (33.1%) had been treated previously with first-line drugs only, and 37 (9.8%) had been treated previously with second-line drugs (Table 2). The proportion of new patients did not show any significant change in trend during our study period (Table 3).
Table 1
Baseline characteristics of 378 patients with MDR-TB
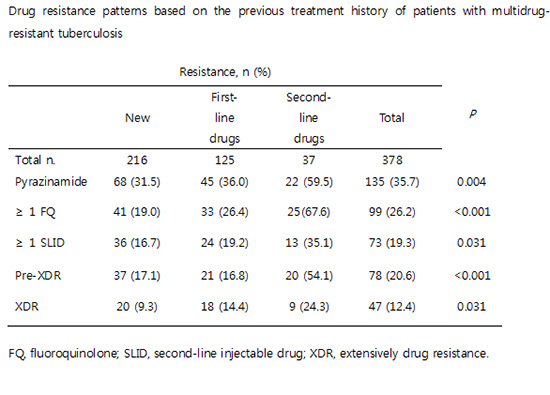
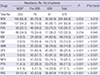
Table 2
Drug resistance patterns based on the previous treatment history of patients with MDR-TB
MDR-TB = multidrug-resistant tuberculosis, RFB = rifabutin, EMB = ethambutol, PZA = pyrazinamide, SM = streptomycin, KM = kanamycin, CM = capreomycin, AMK = amikacin, OFX = ofloxacin, LFX = levofloxacin, MFX = moxifloxacin, PTH = prothionamide, CS = cycloserine, PAS = para-aminosalicylic acid, FQ = fluoroquinolone, SLID = second-line injectable drug, XDR = extensively drug resistance.
Table 3
Trends in the rates of additional drug resistance in patients with MDR-TB
MDR-TB = multidrug-resistant tuberculosis, RFB = rifabutin, EMB = ethambutol, PZA = pyrazinamide, SM = streptomycin, KM = kanamycin, CM = capreomycin, AMK = amikacin, OFX = ofloxacin, LFX = levofloxacin, MFX = moxifloxacin, PTH = prothionamide, CS = cycloserine, PAS = para-aminosalicylic acid, FQ = fluoroquinolone, SLID = second-line injectable drug, XDR = extensively drug resistance.
Drug resistance pattern and trends
The rates of additional drug resistance among MDR-TB patients are shown in Table 2. Strains isolated from MDR-TB patients showed additional resistance to PZA (35.7%), EMB (63.8%), ≥ 1 SLID (19.3%), and ≥ 1 FQ (26.2%). The drug resistance rate for oral second-line bacteriostatic drugs showed the following sequence: PAS (31.5%), PTH (17.5%), and CS (7.1%). Proportions of pre-XDR-TB and XDR-TB were 20.6% and 12.4% respectively.
Drug resistance rates for PZA, FQs, KM, PTH, and CS were significantly higher in previously treated patients than in new patients. During the study period, there were no significant changes in the trends in resistance to all drugs except SM (Table 3).
When patients were categorized based on the level of drug resistance, resistance rates for all drugs, except SM, increased stepwise in the following sequence: uncomplicated MDR-TB, pre-XDR-TB, and XDR-TB (Table 4). Strains from XDR-TB patients showed additional resistance to PZA (70.2%), SM (36.2%), and MFX (74.5%).
Table 4
Drug resistance patterns based on the levels of drug resistance among patients with MDR-TB
MDR-TB = multidrug-resistant tuberculosis, MDR = multidrug resistance, XDR = extensive drug resistance, RFB = rifabutin, EMB = ethambutol, PZA = pyrazinamide, SM = streptomycin, KM = kanamycin, CM = capreomycin, AMK = amikacin, OFX = ofloxacin, LFX = levofloxacin, MFX = moxifloxacin, PTH = prothionamide, CS = cycloserine, PAS = para-aminosalicylic acid, FQ = fluoroquinolone, SLID = second-line injectable drug.
*MDR-TB without additional resistance to FQ and SLID.
We estimated how many patients were eligible for the shorter MDR-TB regimen recommended by WHO. A total of 190 (50.3%) MDR-TB patients had strains susceptible to at least PZA, any FQ, and any SLID and no history of second-line drug treatment. Among them, 95 (25.1%) were fully susceptible to the all drugs comprising the shorter MDR-TB regimen (KM, MFX, PTH, PZA, and EMB). In contrast, 189 (50.0%) patients were fully susceptible to the 5 drugs comprising the standard conventional regimen (PZA, KM, OFX, PTH, and CS).
DISCUSSION
Our study identified 2 major concerns regarding MDR-TB in Korea. First, the proportion of new patients was as high as 57.1% of the total MDR-TB patients, which indicates a high rate of primary transmission in Korea. Second, the rate of additional drug resistance was high, especially to core drugs such as PZA, any FQ, and any SLID. In our study cohort, approximately one-third of the MDR-TB strains were also resistant to PZA, one-fourth of the strains to a FQ, and one-fifth of the strains to any SLID. XDR-TB comprised 12.4% of MDR-TB patients. Such a high level of additional drug resistance poses a challenge to building of an effective treatment regimen and comparable with findings from several countries (8-10).
Primary drug resistance is defined as drug resistance in a patient who has never been treated for TB. It is an indicator of the extent of transmission of resistant bacteria, as well as the effectiveness of TB control programs in the community. In a Korean nationwide drug resistance survey among TB patients registered at the Health Insurance Review and Assessment Service in 2008, the proportion of new patients was 45.0% of the total MDR-TB patients (11), which is comparable to 57.1% of the patients in our study. Primary transmission of MDR-TB strains is a global problem. In a study analyzing drug surveillance data in 30 countries, new patients comprised a median of 54.0% of the MDR-TB cases (12). The high proportion of primary MDR-TB patients suggests the need for a comprehensive TB control program, including contact investigation and infection control, as well as early detection and prompt and effective treatment.
The WHO has recently recommended 2 therapeutic strategies for the treatment of MDR-TB. Drug resistance patterns of individual patients or countries could provide key information on choosing an appropriate strategy (7). The WHO suggests certain criteria to estimate a patient's eligibility for the shorter MDR-TB regimen: the patient should have no history of second-line drug treatment, and should have an M. tuberculosis isolate susceptible to at least PZA, any FQ, and any SLID (13). In our study cohort, only 50.3% of MDR-TB patients could fulfill these eligibility criteria. In Korea, high levels of drug resistance have already been reported in several retrospective MDR-TB cohort studies (11,14-17); additional resistance to PZA, OFX, and KM was 26.2%–59.0%, 16.6%–47.5%, and 13.3%–25.0% respectively. Considering high levels of additional drug resistance, it may not be appropriate to adopt the shorter MDR-TB regimen as a general strategy for MDR-TB treatment in Korea. The effectiveness of the shorter MDR-TB regimen is not proven in countries with high levels of drug resistance.
The risk of treatment failure is inevitably attributable to high levels of additional drug resistance. Treatment outcomes among MDR-TB patients are closely related to the level of baseline drug resistance. In a meta-analysis, the treatment success rate was found to decrease steadily with increase in additional drug resistance (18). The treatment success rates for uncomplicated MDR-TB, pre-XDR-TB with SLID resistance, pre-XDR-TB with FQ resistance, and XDR-TB were 64%, 56%, 48%, and 40% respectively (18). In addition, the Global Preserving Effective TB Treatment Study demonstrated that patients have an increased risk of acquiring resistance to second-line drugs during treatment that corresponds to increase in baseline drug resistance (19). The WHO recommends a standard conventional regimen composed of 4 likely effective second-line drugs as well as PZA, when RFP resistance is detected by rapid molecular DST (7). In our study cohort, we demonstrated that all of the 5 drugs composing a conventional regimen would be effective for only 50% of the MDR-TB patients. In other words, 50% of MDR-TB patients have a risk for treatment failure or acquisition of additional resistance during treatment using the conventional regimen.
In a country with high levels of drug resistance and high-resource settings, individually tailored regimens based on the resistance patterns may be more effective than standardized regimens such as the shorter MDR-TB regimen. A single-center study conducted in Austria demonstrated the achievement of high treatment success rates using 88 different regimens for the treatment of 90 MDR-TB patients (20). For design of such effective and individually tailored regimens, rapid and reliable molecular DST was warranted. However, rapid detection of RFP resistance using currently available molecular DST is a necessary but not a sufficient condition in a country with high levels of drug resistance. In this cohort, one-third of MDR-TB patients were also resistant to FQ or SLID, which means such patients may have a risk for treatment failure or acquisition of additional resistance with the empirical, conventional regimen. Recently, the WHO recommended MTBDRsl assay for early detection of resistance to FQ and SLID (21). If this assay is available, about one-third of the MDR-TB patients could benefit from including bedaquiline, delamanid, or linezolid at treatment initiation.
Our study has a major limitation because our results do not represent the overall situation in Korea. Our results are from regional data derived from 7 university hospitals in the private sector. Drug resistance rates may show differences between public and private institutions as well as between regions. A previous multicenter drug resistance survey showed a higher drug resistance rate in Busan, the region of our study sites, compared to that of other regions (22). One of the reasons for the higher drug resistance rate in our region might be the inclusion of drug resistant TB patients transferred from the National Masan Hospital, which was the largest TB hospital responsible for management of MDR-TB patients in Korea. Therefore, the drug resistance rate in this study might be higher than that of other regions in Korea.
In 2014, the proportion of notified TB cases in Busan, Ulsan, and Gyeongsangnam-do was 16.3% of all notified TB cases in Korea (23). Presently, approximately 90% of TB patients are treated in private hospitals, and the majority of drug resistant TB patients are treated at university hospitals in Korea. Therefore, despite the major limitation, our results may contribute to understanding the current state of MDR-TB in Korea. Further nationwide routine surveillance of drug resistance is needed to improve treatment strategies for MDR-TB patients in Korea.
In conclusion, the proportion of new patients and levels of additional drug resistance to core drugs were high in MDR-TB patients in Korea. Considering the high levels of drug resistance, the shorter MDR-TB treatment regimen may not be feasible; instead, an individually tailored regimen based on the results of molecular and phenotypic DST may be more appropriate in MDR-TB patients in Korea.
 XML Download
XML Download