

 PDF
PDF ePub
ePub Citation
Citation Print
Print




INTRODUCTION
Although there are many causes of acute renal infarction, the most common cause is cardiogenic thromboembolism associated with underlying disease, such as atrial fibrillation, intracardiac thrombus, infective endocarditis, and valvular heart disease. Rare causes include trauma or angiographic-procedure-related arterial injury (1).
Spontaneous renal artery dissection (SRAD), defined as a dissection of the renal artery with no underlying vascular disease, renal artery intervention, or trauma, has been known as a very uncommon event and its incidence and clinical characteristics are not well established (234). Several rare conditions can now be more easily detected using the high resolution images provided by multidetector computed tomography (MDCT) scanning. For example, the number of reports of the isolated dissection of the celiac or superior mesenteric artery has increased recently because of the widespread use of MDCT (56). Likewise, SRAD has been identified more frequently in literature due to the recent advances in MDCT technology (7).
The purpose of this retrospective study was to assess the incidence of SRAD as a cause of acute renal infarction, and to compare the clinical and MDCT findings from patients with renal infarction caused by SRAD with those from patients with renal infarction caused by an embolism.
MATERIALS AND METHODS
Patients
This was a single-center retrospective study. The hospital picture archiving and communication system reports of abdomen computed tomography (CT) scans completed between November 2011 and January 2014 were searched for the text ‘renal infarct’ or ‘renal infarction.’ When relevant text was identified the MDCT data sets and medical records were examined retrospectively. The clinical and imaging data collected at the time of admission and during follow-up included patient demographics, history of underlying disease (hypertension, diabetes mellitus, atrial fibrillation, cardiomyopathy, heart valve disease, coronary artery disease, and malignancy), blood pressure (systolic, diastolic, and mean), and laboratory results, including white blood cell (WBC), C-reactive protein (CRP), lactate dehydrogenase (LDH), creatinine, blood urea nitrogen (BUN), the BUN/creatinine ratio (BCR), and the estimated glomerular filtration rate (eGFR). Coagulation study (prothrombin time and activated partial thromboplastin time) and urinanalysis data (proteinuria, pyuria, and hematuria) were also collected. Patient exclusion criteria were chronic renal infarction, acute pyelonephritis, and lack of clinical data. Hypertension was defined as an arterial systolic pressure higher than 140 mmHg, or a diastolic pressure greater than 90 mmHg, or both, while the patient remained in a seated position for 2 minutes (8). New-onset hypertension was defined as a newly diagnosed hypertension in a patient who was normotensive or had no history of hypertension before visiting our institute. Proteinuria was defined as a positive dipstick test of the urine (9). Pyuria was defined as 5 or more WBCs per high-power field on microscopy of the urine (10). Hematuria was defined as any number of red blood cells per high power field on microscopy of the urine (11).
CT technique
MDCT images of the abdomen were acquired using either a 16-detector CT scanner (Sensation 16; Siemens Medical System, Erlangen, Germany) or a 64-detector CT scanner (Brilliance 64; Philips Medical System, Eindhoven, the Netherlands). The 16-detector MDCT images were obtained with a tube voltage of 120 kVp, a tube current of 200 mAs, a collimation of 16.0 × 1.5, a pitch of 0.75, and a rotation time of 500 ms; the images were reconstructed with a thickness of 2 mm at 1- or 2-mm intervals. The 64-MDCT images were obtained with a tube voltage of 120 kVp, a tube current of 300 mAs, a collimation of 64.00 × 0.67, a pitch of 0.891, and a rotation time of 750 ms; the images were reconstructed with a thickness of 1 or 2 mm at 1- or 1.5-mm intervals. All patients were placed in a supine position on the CT table. The acquisition volume included the whole abdomen from the dome of the diaphragm to the lower margin of the symphysis pubis.
An 18-gauge intravenous cannula was inserted into a vein in the antecubital fossa, forearm, or wrist, and scanning of the abdomen was performed after an intravenous injection of 100–120 mL iopromide (Ultravist 370; Bayer HealthCare, Berlin, Germany) or iohexol (Bonorex 350; CMS, Seoul, Korea) with a flow rate of 2.5–3.5 mL/sec using an automatic power injector (Stellant; Medrad, Indianola, PA, USA). The scan delay time was determined by the automatic bolus tracking method. The region of interest was the descending aorta, at the level of the diaphragm. The CT scan for hepatic arterial-phase images was started 10 seconds after the CT attenuation value of the aorta reached 100 HU for 16-MDCT, or 7 seconds after the CT attenuation value of the aorta reached 150 HU for 64-MDCT. An additional CT scan for portal-phase images was started 25 seconds (for 16-MDCT) or 40 seconds (for 64-MDCT) after the start of the contrast injection. The CT scan was carried out while the patient held their breath at the end of inspiration.
Image analysis and measurement
Two experienced radiologists (S.Y.S. and B.K.K.), who were blinded to the results, interpreted the reconstructed arterial-phased data set independently by consensus using PC-based 3-dimensional software (Rapidia 2.8; Infinitt, Seoul, Korea). The cause of acute renal infarction was first determined by the comprehensive analysis of images and medical records, and then the laterality and extent of acute renal infarction were evaluated. When SRAD was identified as a cause of acute renal infarction, the level and extent of arterial involvement were investigated.
CT diagnosis of renal infarction was based on the presence of a parenchymal perfusion defect in the kidney, either wedge-shaped or otherwise, and either with or without a cortical rim sign (which is a sign of capsular collateral flow in renal infarction), and an absence of major perirenal stranding or mass effect (1213).
Acute renal infarction caused by an embolism was defined by the presence of either one direct sign or one or more indirect signs (Fig. 1). The single direct sign was the presence of intra-arterial filling defect identified by MDCT. The indirect signs included the presence of cardiac thrombi identified by echocardiographic evaluation, arrhythmia (such as atrial fibrillation) identified by electrocardiography (ECG), and co-existing infarction in other organs.
 | Fig. 1MDCT images in 85-year-old man with an atrial fibrillation. Axial image (A) shows multiple infarctions in the spleen (white arrows). Coronal image (B) shows multifocal wedge-shaped infarctions in bilateral kidneys (black arrows) and multiple infarctions in the spleen (white arrows). Renal infarction caused by an embolism was diagnosed.
MDCT = multidetector computed tomography.
|
The diagnosis of acute renal infarction caused by SRAD was based on the MDCT findings. The diagnostic criteria were an intimal flap in one of the renal arteries or eccentric mural low attenuation detected along the renal arteries, indicating a thrombosed false lumen (Fig. 2). Patients with an aortic dissection, history of trauma, arterial catheterization, or underlying vascular disease were excluded.
 | Fig. 2MDCT images in 49-year-old man with new-onset hypertension. (A) Initial. (B) One-month follow-up. (C) 26-month follow-up. Initial curved MPR image (A) shows that the true lumen of a segmental renal artery is compressed by a thrombosed false lumen (black arrow). Curved MPR image at 1-month follow-up (B) shows the aggravated narrowing of the true lumen (white arrow) and the aneurysmal change has developed (white arrow head). The previous infarction area has been atrophied in the cured MPR image at 26-month follow-up (C), even though the dissected renal vessels have been normalized (black arrow heads). Spontaneous renal artery dissection was diagnosed.
MDCT = multidetector computed tomography, MPR = multiplanar reconstruction.
|
Statistical analysis
Statistical analyses were performed with SPSS version 20.0 software for Windows (SPSS Inc., Chicago, IL, USA). Categorical variables were examined by Fisher's exact test and continuous variables by the Mann-Whitney test. All statistical tests were 2-sided tests. A P value less than 0.05 was considered to be statistically significant.
RESULTS
Among the 67 patients who were searched for the text ‘renal infarct’ or ‘renal infarction,’ 32 patients were excluded: chronic renal infarction (n = 26), acute pyelonephritis (n = 4), and lack of clinical data (n = 2). As a result, a total of 35 patients with renal infarction were included in this study; 25 male and 10 female patients. The median age of the patients at the initial clinical presentation was 56 years and the age range was 11–85 years. The baseline characteristics of study population are listed in Table 1. The most common cause was an embolism (n = 14, 40.0%). Among these patients, one had a direct sign (thrombi in the renal artery) and the remaining 13 had indirect signs, including concomitant infarction of the spleen in 8 patients (57.1%), and atrial fibrillation in 5 patients (35.7%). SRAD was the second most common cause of acute renal infarction (n = 6, 17.1%). Thirty-two patients (91.4%) showed segmental renal infarction. The remaining 3 patients (8.6%) showed total infarction of the affected kidney. Bilateral lesions were only present in patients with an embolism or vasculitis. The characteristics according to the causes of acute renal infarction are summarized in Table 2.
Table 1
Baseline characteristics of study population
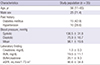
Values for categorical variables are given as a number (%); values for continuous variables, as mean ± standard deviation or median (range).
BUN = blood urea nitrogen, eGFR = estimated glomerular filtration rate.
![]()
Table 2
Proportion of laterality and extent of acute renal infarction by causes

![]()
The clinical, imaging, and laboratory characteristics of patients with renal infarction caused by either SRAD or an embolism are summarized in Table 3. One of 6 (16.7%) patients with SRAD had a history of hypertension. On the other hand, four of 14 (28.6%) patients with an embolism had a history of hypertension. All of these patients with a history of hypertension were on antihypertensive medication at admission. Patients with SRAD experienced new-onset hypertension more frequently than patients with an embolism (P = 0.018). Patients with an embolism were found to have increased CRP more often than patients with SRAD (P = 0.002). The mean values of LDH, BUN, and BCR were all significantly higher in patients with an embolism than in patients with SRAD (P = 0.012, P = 0.009, and P = 0.025, respectively). Creatinine, eGFR, blood pressure, coagulation study, and urinalysis results were not significantly different between the 2 groups. Bilateral renal involvement, as visualized using MDCT, was detected significantly more often in patients with an embolism (n = 9, 64.3%) than in patients with SRAD (n = 0, 0%) (P = 0.014). All patients with SRAD showed normal ECG at admission. On the other hand, the findings of ECG in patients with an embolism were normal in 7 patients (50.0%), atrial fibrillation in 5 patients (35.7%), and nonspecific ST and T-wave changes in 2 patients (14.3%).
Table 3
Comparison of clinical, laboratory, and imaging characteristics in patients with SRAD and patients with an embolism

Values for categorical variables are given as a number (percentage); values for continuous variables, as mean ± standard deviation or median (range); P < 0.05 indicates statistical significance.
SRAD = spontaneous renal artery dissection, BUN = blood urea nitrogen, eGFR = estimated glomerular filtration rate, LDH = lactate dehydrogenase, WBC = white blood cell, CRP = C-reactive protein, PT = prothrombin time, INR = international normalized ratio, aPTT = activated partial thromboplastin time.
*Fisher's exact test; †Mann-Whitney test.
![]()
MDCT images in 4 of 6 (66.7%) patients with SRAD showed an intimal flap in the renal arterial lumen. In the remaining 2 patients with SRAD, there was no evidence of an intimal flap; however, eccentric mural thrombi with low attenuation along the artery were evident on the MDCT images, suggesting thrombosed false lumens. In patients with SRAD, the arteries involved were the main renal to divisional artery in 2 patients, the divisional to segmental artery in 2 patients, and the segmental artery in 2 patients. Stenosis of the true lumen, due to compression by a thrombosed false lumen, was present in all patients with SRAD, and the unaffected renal arteries and aorta had smooth walls and normal caliber, without evidence of any other arterial disease, such as fibromuscular dysplasia (14).
Clinical follow-up was available in 4 patients with SRAD (66.7%). Two patients with SRAD were lost to follow-up because of transfer to a different hospital. Median clinical follow-up of patients with SRAD was 12 months (range 4–36 months). All 4 patients with SRAD, except 2 who were lost to follow-up, were conservatively treated with anticoagulation (Warfarin), angiotensin receptor blocker (ARB), and/or angiotensin-converting enzyme (ACE) inhibitor. Anticoagulation therapy was started in 3 of the 4 patients with SRAD after the infarction and was continued until the last follow-up (mean, 28.7 months). The blood pressure of all 4 patients with SRAD was easily controlled by ARB and/or ACE inhibitor after the infarction. All of the laboratory markers except for eGFR returned to normal after the event. However, the eGFR of all 4 patients with SRAD indicated stage 2 chronic kidney disease at every follow-up visit. No patient with SRAD progressed to eGFR < 60 mL/min/1.73 m2 or end-stage renal disease (ESRD) during follow-up. The results of follow-up blood pressure and eGFR are compared between patients with SRAD and patients with an embolism (follow-up data were available in 5 outpatients) shown in Figs. 3 and 4.
 | Fig. 3Comparison of the eGFR between patients with SRAD (A) and patients with an embolism (B) during the follow-up period.
eGFR = estimated glomerular filtration rate, SRAD = spontaneous renal artery dissection.
|
 | Fig. 4Comparison of the blood pressure between patients with SRAD (A) and patients with an embolism (B) during the follow-up period.
SRAD = spontaneous renal artery dissection.
|
MDCT follow-up was available for 3 of the 4 patients with SRAD and complete follow-up notes. The median MDCT follow-up was 22 months (range 1–26 months). One-month follow-up MDCT, which was available for 2 patients, showed the progressed compression of the true lumen caused by the expansion of the thrombosed false lumen. An aneurysmal change in the renal artery was detected in one patient (Fig. 2). Final follow-up MDCT images (median 26 months, range 22–26 months) were available in 3 patients with SRAD, and they revealed the decreased size of the affected kidney, parenchymal scarring of the previous infarction area, and normalization of dissected renal vessels.
DISCUSSION
Acute renal infarction, resulting from an acute disruption of renal blood flow, is rare in clinical practice, with an estimated incidence of 0.004% (15). The diagnosis tends to be missed or made late, mainly due to nonspecific clinical presentation and rarity of the disease. However, acute renal infarction may cause irreversible damage to the kidney, and can be indicative of serious cardiovascular disease (131617). It is, therefore, essential to identify the cause of acute renal infarction, as this will affect both the management and prognosis of the patient. Among the various causes of acute renal infarction, the most common cause is cardiogenic thromboembolism; other causes include an underlying disease, such as atrial fibrillation, cardiomyopathy, valvular heart disease, infective endocarditis, and thrombi from either the left ventricle or the suprarenal aorta (1). Rare causes of acute renal infarction include renal artery injury caused by trauma or an angiographic procedure, hypercoagulable diseases, and hematologic disorders (18). In the current study, we investigated the causes of renal infarction. We found that an embolism was the most frequent cause of renal infarction (40.0%), and 35.7% of patients with an embolism had an atrial fibrillation; this agrees with the results from a previous study that reported that renal infarction often has a cardiogenic origin (55.7%), and 86.5% of patients with renal infarction of cardiogenic origin also have atrial fibrillation (1).
SRAD is a rare event. The first report of SRAD was in 1944 (19), and since then approximately 200 cases have been published in the literature, with most publications reporting on isolated cases or a small series of cases (234). Until the 1970s, SRAD was usually diagnosed by autopsy or angiography (320), therefore the incidence of SRAD has not been well understood in previous reports. Recently, Oh et al. (1) reported that, of 438 patients with renal infarction, 21 (4.79%) patients had SRAD. With improvements in technology, resulting in the high spatial resolution of current MDCT scanners, SRAD is increasingly being identified correctly and reported in the literature (720). In the current study, SRAD was the second most common cause of acute renal infarction (17.1%). This incidence is even higher than that of previous report by Oh et al. (1), and this difference is probably caused by the retrospective analysis of CT source data. Our result is presumably close to the true incidence of SRAD, and suggests that SRAD might be a crucial cause of acute renal infarction.
Previous studies reported that 28.0%–30.1% of patients with renal infarction had no known cause (121). Similarly, seven (20.0%) patients in the current study had no known cause of renal infarction, despite exhaustive investigations. Radiological images and clinical histories help us to investigate the etiologies of acute renal infarction caused by trauma, angiographic injury, or aortic dissection but, nevertheless, the characteristics of SRAD visualized by CT scanning might be subtle and could be easily overlooked during daily practice. In the current study, only 1 of 6 (16.7%) patients with SRAD was diagnosed correctly during the routine interpretation of abdominal CT, and the remaining 5 cases were diagnosed by retrospective review; a careful interpretation of thin-section imaging was needed to diagnose a renal infarction caused by SRAD (2223). Even though embolism is the most common cause of acute renal infarctions, it is sometimes hard to find evidence of embolism.
SRAD is more common among men, with a prevalence of between 4:1 and 10:1, and predominantly occurs in the 4th to 6th decade of life in the absence of underlying co-morbid conditions (24252627). Consistent with previous reports, the current study also shows that acute renal infarction is more common in men than in women, that SRAD is a cause of acute renal infarction in younger patients more often than an embolism, and that the incidence of classic cardiovascular risk factors is more frequent in patients with an embolism than in patients with SRAD. However, none of these parameters was statistically significant in the current study, probably as a result of the small number of included patients.
In previous reports of renal infarction, less than 15.0% of patients had bilateral renal involvement, whether caused by SRAD or an embolism (220). In the current study, however, 100% of patients with SRAD had unilateral renal involvement and 64.0% of patients with embolic disease had bilateral renal involvement. This statistically significant difference (P = 0.014) is probably a result of the improved ability of MDCT to detect minimal changes of renal infarction. These findings also suggest that bilateral renal involvement could be used to differentiate renal infarction caused by an embolism from renal infarction caused by SRAD.
Hypertension was reported in almost all previous studies of patients with SRAD (2). This is probably explained by the presence of renal ischemia due to the compression of the true lumen. In the current study, all 6 patients with SRAD were hypertensive at the time of admission. Although there is the possibility that SRAD may be the consequence of uncontrolled hypertension in 1 patient with SRAD who had a history of hypertension before the event, our results showed that hypertension was likely the consequence of SRAD because remaining 5 patients with SRAD had no history of hypertension before admission. On the other hand, the incidence of new-onset hypertension at the time of admission was significantly higher in patients with SRAD than in patients with an embolism. Thus, the detection of new-onset hypertension might play an important role in differentiating patients with SRAD from patients with an embolism.
We used laboratory data to investigate whether certain laboratory tests can help to discriminate between patients with SRAD and those with an embolism. We discovered that the mean values of LDH, BUN, and BCR were all significantly higher in patients with an embolism than in patients with SRAD. This is plausible because patients with an embolism were at higher risk of a cardiovascular event than patients with SRAD, and this consequently reduced the kidney function. In addition, patients with SRAD were able to preserve renal function, as all of the renal lesions in patients with SRAD were unilateral.
The outcomes for patients with SRAD have not been clearly elucidated in previous reports. In the current study, the blood pressure in patients with SRAD was controlled without difficulty, using either ARB or ACE inhibitor. Laboratory results, including tests for creatinine, LDH, BUN, and BCR were all in the normal ranges at every follow-up appointment. All 4 patients with SRAD who had follow-up notes had mildly reduced eGFR during the follow-up period. This is perhaps because of the reversible renal insufficiency associated with ACE inhibitor therapy (28). Moreover, none of the patients with SRAD progressed to eGFR < 60 mL/min/1.73 m2 or ESRD during the follow-up period.
The characteristics of SRAD, as visualized on MDCT images, have previously been reported as severe luminal narrowing, caused by an intimal flap, or widening of the renal artery and its branches due to an opacified false lumen (7). In the current study, an intimal flap with an eccentric low attenuation in the renal arterial lumen was found on initial CT in patients with SRAD, which is consistent with the previous studies (1219). In the current study we also found stenoses of the true lumen due to compression by a thrombosed false lumen in all patients with SRAD. These findings correlate with the clinical finding of high blood pressure in all patients with SRAD. Short-term follow-up MDCT images in 2 patients with SRAD revealed expansion of the false lumen and aggravated compression of the true lumen. Furthermore, the long-term follow-up MDCT images of 3 patients with SRAD showed normalized renal vessels due to the absorption of the thrombosed false lumen. This agrees with the clinically stable course of patients with SRAD.
The current study has several limitations. Firstly, the data were collected retrospectively. As a result, they are susceptible to all limitations and biases inherent in any retrospective design; for example, we would expect pain scores to be different between patients with SRAD and those with an embolism, but we could not obtain exact information about patient-reported pain. Secondly, there might be a difference of sensitivity between 16-detector and 64-detector scanners. Thirdly, our study was conducted at a single institute. This can have a negative influence on selection bias, although it can limit the impact of investigator bias. Last, the sample size is too small to clarify any statistical difference in parameters such as age and sex. These limitations could be overcome by a blinded, prospective, and randomized study with a large patient population from multiple institutions.
In conclusion, SRAD is not a rare cause of acute renal infarction, and it has a benign clinical course. It should be considered in a differential diagnosis of acute renal infarction, particularly in patients with new-onset hypertension, unilateral renal involvement, and normal ranges of CRP, LDH, BUN, and BCR.
 XML Download
XML Download