

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Behçet's disease (BD) is a chronic, recurrent, multisystem vasculitis with 4 cardinal symptoms, including oral ulcers, genital ulcers, skin lesions, and eye lesions. Besides these cardinal symptoms, central nervous system symptoms, vasculitis, arthritis, gastrointestinal symptoms, and epididymitis can be associated with the disease as minor symptoms. As a result of vasculitis, BD is a prothrombotic state which can cause superficial and deep venous thromboses, arterial aneurysms and occlusion (12). Even though various causes such as genetic factors, infections, and pollutants, have been proposed as potential causes for BD pathogenesis, the exact cause still remains to be elucidated.
After the introduction of bivalent and quadrivalent human papillomavirus (HPV) vaccination, postlicensure studies showed interesting data. Although the HPV vaccine is generally safe and well tolerated, issues about autoimmune disease was reported. It was a report on the rate of autoimmune, neurological, and venous thromboembolic adverse events after immunization of adolescent girls in Denmark and Sweden with the quadrivalent HPV vaccine. In this report, exposure to the quadrivalent HPV vaccine was associated with Raynaud's disease and type 1 diabetes. The quadrivalent HPV vaccine, in particular, was significantly associated with BD (3).
This means that either an HPV antigen, an immunostimulant contained in the vaccine, or an aberrant immune response of the host could be important initiators in the development of BD. Otherwise, HPV infection could be another plausible cause of BD development.
As there are some reports about related with BD and infections, we hypothesized HPV infection is related with BD. The objective of this study was to evaluate whether the anti-HPV antibody titer is increased in BD.
MATERIALS AND METHODS
Patients
A total of 93 Korean BD patients, who visited the BD Specialty Clinic at Severance Hospital and fulfilled the diagnostic criteria of the International Study Group for BD were recruited (mean age 42.85 ± 11.25 years; M/F 22/71). Healthy controls of 40 subjects were enrolled who visited our hospital for health checkup without active infectious disease (mean age 47.13 ± 8.95 years; M/F 18/22). Each subjects of both group had no history of any type of HPV vaccine. All serum samples were kept in a −70°C freezer and thawed at room temperature before use.
Assessment of disease activity
The clinical activity of BD was evaluated at the time of blood sampling. Two general assessment tools for the disease activity, the Behçet Disease Current Activity Form (BDCAF) and the electronic medical record (EMR)-based activity index (EMRAI) score, were used in this study. We used the latest version of the BDCAF (http://www.behcet.ws/behcetwsData/Uploads/files/BehcetsDiseaseActivityForm.pdf; last accessed: on 26 January, 2016) in this study. The EMRAI is a simplified activity measurement form for BD, which was validated by its good correlation with the BDCAF (16). In brief, the EMRAI score was calculated as the sum of one point for each of 9 findings/symptoms (oral and genital ulcers, ocular symptoms, skin lesions, epididymitis, and symptoms related to the joints, gastrointestinal tract, vascular system, and the central nervous system), and an additional one point was added if a symptom was a new event. An elevated erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) value above their reference levels would also each increase the EMRAI score by one point. Because practical cut-off values to define ‘active disease’ for BD are not currently available, we defined BD as being in the active phase if the patient presented with ≥ 2 major criteria according to the revised criteria of the BD Research Committee of Japan (4).
Preparation of antigen
HPV-16 L1 virus-like particle (VLP; stock number 120525-1) (5) was used in this study, which was supplied by EyeGene Inc. (Seoul, Korea). Briefly, HPV L1 VLP antigen was expressed from a yeast system. After cultured cells were disrupted, the lysate was precipitated using ammonium sulfate. Precipitated lysate was resuspended and then purified by cation exchange chromatography. The purified VLP was used in this experiment.
Enzyme-linked immunosorbent assay (ELISA)
One hundred microliters of a 20 µg/mL HPV-16 L1 VLP antigen solution was coated on an ELISA plate. After washing, 100 µL aliquots of 1/200 diluted sera from patients and normal controls were added. After washing, 100 µL of a horseradish peroxidase (HRP)-conjugated goat anti-human immunoglobulin G (IgG) polyclonal antibody (Sigma-Aldrich, St. Louis, MO, USA) bound to the primary antibodies. After washing away any unbound antibodies, 100 µL of the 1 mg/mL chromogenic substrate 3,3′,5,5′-tetramethylbenzidine (KPL Inc., Gaithersburg, MD, USA) diluted in 100 mM sodium acetate-phosphate buffer, pH 4.2, containing 0.015% H2O2 was added to visualize the antibody complexes. Absorbance at 450 nm was measured after 3–5 minutes with an automated plate reader (Dynatech Service Company, Inc., Alexandria, VA, USA). All the samples were analyzed in duplicate.
Statistical analysis
All statistical analyses were performed using SAS statistical software (version 9.3; SAS Institute Inc., Cary, NC, USA). Discrete variables were described using the frequency (percentages), and continuous variables were reported using the median (range) or mean (standard deviation [SD]). The Mann-Whitney U-test was used for comparison of serum anti-HPV-16 antibody titers between the 2 independent groups. A receiver operating characteristic (ROC) curve was created to determine the optimal anti-HPV-16 antibody titer cut-off level. Using this cut-off value for anti-HPV-16 antibody titer, the sensitivity and specificity were calculated. A univariate logistic regression analysis was performed to investigate possible differences in BD patients depending on serum anti-HPV-16 antibody titers. A Pearson's correlation analysis was used to evaluate the relationship between the different study parameters. All probabilities were 2-tailed, and statistical significance was set at P < 0.05.
Ethics statement
This study was approved by the Institutional Review Board of Severance Hospital, Yonsei University College of Medicine, Seoul, Korea (IRB No. 4-2015-0259). All participants provided written informed consent. The study was conducted according to the Declaration of Helsinki Principles.
RESULTS
Characteristics of the study population
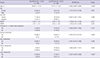
The detailed demographic and clinical characteristics of our subjects are summarized in Table 1. The prevalence of both cardinal symptoms and current symptoms at the time of blood sampling was evaluated. Recurrent oral ulcers were observed in all patients. Other areas of involvement included genital ulcers (n = 87, 93.5%), skin lesions (n = 85, 91.4%), articular involvement (n = 61, 65.6%), ocular involvement (n = 29, 31.2%), gastrointestinal lesions (n = 6, 6.5%), vascular involvement (n = 1, 1.1%), and neurological involvement (n = 1, 1.1%). Positivity for human leukocyte antigen-B51 (HLA-B51), a gene allele associated with susceptibility to BD, was noted in 31 (36.5%) of 85 tested patients. At the time of blood sampling, the mean BDCAF score was 2.25 ± 1.31 (range: 0–6), and the mean EMRAI score was 2.77 ± 1.26 (range: 0–7). The mean values for ESR and CRP were 33.77 (range: 2.0–94.0) mm/hr and 5.84 (range: 0.30–71.07) mg/dL, respectively.
Table 1
Characteristics of patients with BD

BD = Behçet's disease, BDCAF = Behçet's disease current activity form, CNS = central nervous system, CRP = C-reactive protein, EMRAI = electronic medical record-based activity index, ESR = erythrocyte sedimentation rate, GI = gastrointestinal, HLA-B51 = human leukocyte antigen-B51.
*Continuous variables = mean ± SD; †Categorical variables = number (%); ‡Patients treated with corticosteroids ≥ 5 mg/day, colchicine, and/or azathioprine were included; §HLA-B51 was assessed in 85 patients; ∥Continuous variables: median (interquartile range).
![]()
Serum anti-HPV-16 antibody titers and determination of the optimal cut-off point
As shown in Fig. 1, patients with BD had significantly higher antibody titers against HPV-16 (optical density [OD], 0.210–3.675; mean 0.992) than did healthy controls (OD, 0.248–0.762; mean 0.517; P < 0.001). Using a ROC analysis, the cut-off value for the anti-HPV antibody titer of 0.578 OD was determined to differentiate BD patients from healthy controls. This cut-off value established a sensitivity of 67.7% and specificity of 71.8% (Fig. 2).
 | Fig. 1Serum anti-HPV 16 antibody levels in the patients with BD. (mean OD in BD patients: 0.992; mean OD in normal control: 0.517).
HPV = human papillomavirus, BD = Behçet's disease, OD = optical density.
*
P < 0.001.
|
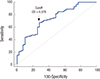 | Fig. 2Serum anti-HPV 16 antibody levels and determination of cut-off point. Cut-off value for Serum anti-HPV 16 antibody levels which differentiates BD patients from normal controls was determined by Youden index method. Youden index was 0.3954, cut-off point was 0.578 OD. AUC was 0.737. Sensitivity was 67.74%. Specificity was 71.79%.
HPV = human papillomavirus, OD = optical density, AUC = area under curve.
|
A logistic regression analysis was performed to evaluate the validity of the cut-off value from the ROC analysis and to identify any associations between the different clinical manifestations and the serum anti-HPV-16 antibody titer in BD patients (Table 2). BD patients were categorized into 2 groups according to the serum anti-HPV-16 antibody titer (≥ 0.578 OD and < 0.578 OD). In regards to disease activity, no meaningful differences were identified between these 2 groups. Patients with an anti-HPV-16 antibody titer ≥ 0.578 OD did not possess significantly higher BDCAF and EMRAI scores compared to patients with a titer < 0.578 OD. The proportion of patients presenting with ≥ 2 major criteria (with or without any minor criteria), who were defined as having BD in the active phase according to the revised criteria of the BD Research Committee of Japan, was not significantly different from that of the group with an anti-HPV-16 antibody titer ≥ 0.578 OD. When we compared the clinical features of BD between the 2 groups, articular involvement of BD was more likely in patients with an anti-HPV-16 antibody titer < 0.578 OD (P = 0.035). In addition, patients with an anti-HPV-16 antibody titer < 0.578 were significantly younger than patients with a titer ≥ 0.578 OD. However, no statistically significant differences were observed in the gender, HLA-B51 genotype, or any other single organ involvement between the 2 titer groups. A Pearson's correlation analysis also failed to find significant differences in anti-HPV antibody titers with respect to the disease activity scores or the serum levels of ESR and CRP (Table 3).
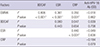
Table 2
Comparison of clinical features and disease activity between patient subgroups categorized according to the cut-off value for anti-HPV-16 antibody titer (0.578 OD)
Data are shown as mean ± standard deviation or number (%).
HPV = human papillomavirus, OD = optical density, BDCAF = Behçet's disease current activity form, EMRAI = electronic medical record-based activity index, HLA-B51 = human leukocyte antigen-B51, Ab = antibody, OR = odds ratio, CI = confidence interval.
*Differences were considered statistically significant at P < 0.05; †HLA-B51 was assessed in 85 patients.
![]()
Table 3
Correlation between serum anti-HPV-16 antibody titers, clinical variables, and disease activity scores
Spearman analysis-no significant association with anti-HPV-16 antibody titers with any other values.
HPV = human papillomavirus, BDCAF = Behçet's disease current activity form, EMRAI = electronic medical record-based activity index, ESR = erythrocyte sedimentation rate, CRP = C-reactive protein, Ab = antibody, OD = optical density.
*Pearson correlation coefficient; †Differences were considered statistically significant at P < 0.05.
![]()
DISCUSSION
BD is a chronic, multisystem inflammatory disorder characterized by the recurrent involvement of mucocutaneous (oral and genital ulceration, erythema nodosum like skin eruption, acne-like skin eruption, etc.), ocular, vascular, digestive, and/or nervous system organs (6). Although the etiology of BD remains unknown, the pathogenesis has been clarified by extensive studies of the disease's epidemiology, clinical manifestations, and basic etiological research based on the intrinsic genetic and extrinsic triggering factors and the immunological findings (7).
An unhygienic oral condition may be suspected as an extrinsic triggering factor because periodontitis, delayed teeth, chronic tonsillitis, etc. are frequently associated in the oral cavity of BD patients (8). In addition, infectious agents, especially Streptococcus sanguinis and viruses such as herpes simplex virus (HSV), have long been postulated as major triggering factors for BD. The proportion of S. sanguinis in the oral bacterial flora of BD patients is significantly higher than those of healthy and disease controls (9). Serum IgA antibody against S. sanguinis has been reported in patients with BD (10). The target antigen for this antibody is hnRNP A2/B1 in endothelial cells, which possibly contribute to the development of vasculitis in BD patients (11).
DNA from various types of viruses, including HSV, varicella zoster virus, cytomegalovirus, Epstein-Barr virus, human herpes viruses 6 and 7, hepatitis virus, human immunodeficiency virus, and parvovirus B19 have been isolated from BD patients (12). Among these viruses, HSV is the leading candidate for playing a potential role in the pathogenesis of BD. The presence of the HSV genome in peripheral blood mononuclear cells of patients with BD has been demonstrated by in situ DNA-RNA hybridization techniques and polymerase chain reaction (PCR) studies (13). PCR studies have demonstrated significantly greater quantities of HSV-1 DNA in saliva, intestinal ulcers, and genital ulcers from BD patients than controls (1314). In addition, an animal model created by inoculating ICR mice with HSV (1516) and receiving subsequent antiviral treatment showed improving BD-like symptoms in 40% of famciclovir-treated BD mice (17). However, whether these 2 pathogens, HSV or S. sanguinis, can play an important role in the development of BD should be resolved.
In this report, we demonstrated that anti-HPV-16 antibody titers in the sera of patients with BD are significantly increased when compared to those of normal controls. However, there were no correlations between anti-HPV-16 antibody titers and various parameters, including disease activity, clinical symptoms, or laboratory findings. However, articular involvement of BD may be more likely in patients with anti-HPV-16 antibody titer < 0.578 OD (P = 0.035). We could not explain the correlation between the clinical significance of articular involvement and increased anti-HPV-16 titer. In addition, patients with an anti-HPV-16 antibody titer < 0.578 were significantly younger than patients with anti-HPV-16 antibody titer ≥ 0.578 OD. This difference in titer level might be from more active immunological responses in the younger generation than those in the older generation. These 2 parameters are not important for the association of HPV infection with BD.
We still do not understand the meaning of the increased anti-HPV-16 antibody titers in the sera of patients with BD. However, HPV may be another possible infectious agent causing the development of BD. As stated previously, an unhygienic oral condition has been suspected as one of the extrinsic triggering factors for the development of BD. HPV infection is also associated with poor oral hygiene. Patients may be unable to maintain a clean hygienic condition because of their painful pathological lesions. We speculate that BD patients may be more easily infected with HPV. This might be another explanation for the increased anti-HPV-16 antibody titers in the sera of patients with BD.
HPV antigen may be a plausible triggering factor for the development of BD in genetically susceptible populations. This proposal is possible because recent studies suggest an interaction between genetic factors and environmental factors, such as the immune response to pathogens and the gut microbiome composition. This may explain the role of environmental factors in the development of BD (7).
Recently Tomljenovic and Shaw (18) found evidence of an autoimmune vasculitis potentially triggered by cross-reactive HPV-16 L1 antibodies binding to the walls of cerebral blood vessels in postmortem brain tissue from 2 young women who suffered from cerebral vasculitis-like symptoms following vaccination with the quadrivalent HPV vaccine. Lee (19) reported that a healthy teenage girl suffered from a sudden death in her sleep 6 months after 3 intramuscular injections of the quadrivalent HPV vaccine. The postmortem blood and splenic tissue obtained at autopsy were found to contain HPV-16 L1 gene DNA similar to the HPV-16 gene DNA fragments in the quadrivalent HPV vaccine, suggesting a possible link. These mean HPV-16 can be associated with vasculitis. However, there has been no evidence for an HPV infection in BD patients which is thought to be vasculitis. To elucidate the abnormal humoral immune response to HPV and to analyze cellular immune response to the HPV antigen, additional studies should be conducted.
Still we do not know the pathogenesis of HPV infection and relation between HPV infection and antibody titer. Relation between antibody titer itself and infection status or cervical lesion is also unclear. In one study, ELISA assays correlate good/very good with HPV-16/18 detected by PCR (20).
Although the increased antibody titer does not mean that there is an ongoing infection, and does not reveal when the patient was infected, it can indirectly suggest that there is a history of exposure to the virus. And also there can be another factor such as sexual activity. This is the first limitation of our study. Second, as the study was limited by our hospital, total patient group and control group were relatively small. Third, data of sexual activity and Papanicolaou smear test to correlate with HPV infection is not included.
In conclusion, we have demonstrated increased anti-HPV-16 antibody in the serum of the patients with BD. However, the significance of this finding remains still unclear. Further studies will need to be conducted to clarify whether HPV plays a role in the development of BD.
 XML Download
XML Download