

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Marfan syndrome (MFS) is an autosomal dominant disorder (1,2) caused by mutations in the fibrillin-1 (FBN1) gene on chromosome 15 (3). FBN1 is essential for the proper formation of the extracellular matrix, including the biogenesis and maintenance of elastic fibers. Elastic fibers are found throughout the body, but are particularly abundant in the aorta, ligaments, and the ciliary zonules of the eye (4). Abnormal or deficient FBN1 probably affects the structural integrity of the extracellular matrix and may enhance the release of active transforming growth factor-β (TGF-β) (5), resulting in aberrant thickening of the aortic media with fragmentation and disarray of elastic fibers. Clinical presentation of MFS ranges from mild to severe systemic disease. If MFS patients are not correctly managed, the affliction can lead to early or sudden death, as MFS affects the circulatory system, causing mitral valve prolapse, aortic regurgitation, dilated aorta, aortic aneurysm, or aortic dissection. MFS can also affect the lungs, causing spontaneous pneumothorax or emphysema; the eyes causing lens dislocation; the dural sac surrounding the spinal cord, causing dural ectasia; the skeleton, causing abnormal curvature of the spine, abnormal indentation or protrusion of the sternum, abnormal joint flexibility, flat feet, hammer toes, and stooped shoulders; the hard palate, causing a high-arched palate or malocclusions; or the skin, causing unexplained stretch marks. A previous study showed that MFS affects males and females equally (6) and shows no ethnic or geographical bias (7). However, few studies have evaluated the prevalence of MFS in Korea. Therefore, we investigated the prevalence of MFS in Korea between 2006 and 2013.
MATERIALS AND METHODS
Study population
Data were collected from the Korean National Health Insurance Benefit records from 2006 through 2013. Records for Medical Aid of the National Health Insurance Service were excluded. A main diagnosis was extracted from the records of the Korean National Health Insurance Benefit system when the data described primary diagnosis based on complaints and symptoms without the diagnosis being confirmed during the period of treatment. Patients had been seen at various medical institutes. The data consisted of primary diagnoses related to MFS (Q87.4) diagnosed according to the 10th revision of the International Statistical Classification of Diseases and Related Health Problems. Therefore, the finalized diagnoses may be different from the diagnoses in the data. Data in the National Health Insurance Benefit records represent the first diagnosis in that year.
Diagnostic criteria
Diagnostic criteria of MFS were conformed internationally in 1996 (8). The Ghent Nosology was revised in 2010, and new diagnostic criteria superseded the previous agreement made in 1996 (9). The new criteria that lead to a diagnosis are the following: if no family history of MFS, 1) an aortic root Z-score ≥ 2 using echocardiographic or thoracoabdominal computed tomography (aortic root Z-score ≥ 2) and ectopia lentis, 2) aortic root Z-score ≥ 2 and FBN1 mutation, 3) aortic root Z-score ≥ 2 and a systemic score > 7 points, or 4) ectopia lentis and an FBN1 mutation with known aortic pathology. In a patient with family history of MFS, 1) ectopia lentis, 2) a systemic score less than or equal to 7 points, or 3) an aortic root Z-score ≥ 2. The systemic score is calculated using the following characteristics: 3 points for the wrist and thumb signs (1 point for the wrist or thumb sign); 2 points for pectus carinatum (1 point for pectus excavatum or chest asymmetry); 2 points for hindfoot deformity (1 point for plain pes planus); 2 points for dural ectasia; 2 points for protrusio acetabuli; 1 point for a reduced upper segment/lower segment ratio and increased arm/height ratio and no severe scoliosis; 1 point for scoliosis or thoracolumbar kyphosis; 1 point for reduced elbow extension; 1 point for facial features (the presence of at least 3 of following 5 features: dolichocephaly, enophthalmos, downslanting palpebral fissures, malar hypoplasia, or retrognathia); 1 point for skin striae (stretch marks); 1 point for myopia > 3 diopters; and 1 point for 25% mitral valve prolapse.
RESULTS
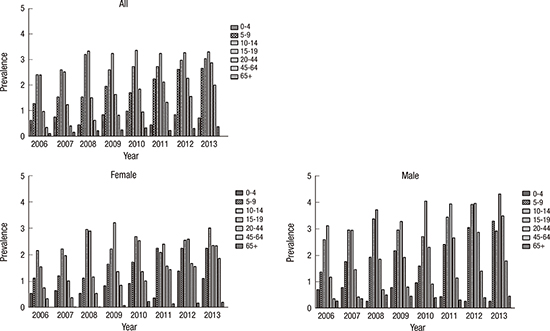
Overall, the age-standardized prevalence of MFS was 0.90 per 100,000 persons in 2006 and 2.27 in 2013. For males in 2006, the prevalence of MFS per 100,000 persons was 0.70 in 0–4 years old, 1.36 in 5–9 years old, 2.59 in 10–14 years old, 3.12 in 15–19 years old, 1.17 in 20–44 years old, 0.36 in 45–64 years old, and 0.27 in men older than 65 years. For males in 2013, the prevalence of MFS per 100,000 persons was 0.26 in 0–4 years old, 3.29 in 5–9 years old, 3.92 in 10–14 years old, 4.32 in 15–19 years old, 3.49 in 20–44 years old, 1.79 in 45–64 years old, and 0.45 in men over 65 years. For females in 2006, the prevalence of MFS per 100,000 persons was 0.55 in 0–4 years old, 1.12 in 5–9 years old, 2.17 in 10–14 years old, 1.55 in 15–19 years old, 0.76 in 20–44 years old, 0.34 in 45–64 years old, and 0 in women older than 65 years. For females in 2013, the prevalence of MFS per 100,000 persons was 1.11 in 0–4 years old, 2.25 in 5–9 years old, 3.02 in 10–14 years old, 2.36 in 15–19 years old, 2.35 in 20–44 years old, 1.87 in 45–64 years old, and 0.21 in women over 65 years (Fig. 1, Table 1).
 | Fig. 1Age-adjusted cumulative prevalence of MFS per 100,000 persons by age group and years (2006–2013) overall, in female, and in male.
MFS = Marfan syndrome.
|
Table 1
Age-adjusted cumulative prevalence* and 95% CI of MFS overall and by sex (per 100, 000 persons)

CI = confidence interval, MFS = Marfan syndrome.
*Age-standardized prevalence rates of MFS were calculated using age groups according to a direct method using the estimated Korean population in 2010 as a reference.
![]()
DISCUSSION
The overall age-standardized prevalence of MFS increased from about 1 to 3 persons per 100,000 persons between 2006 and 2013. The patterns of the prevalence of MFS in the age groups of 20–44 years-old and 45–64 years-old for both sexes showed the steady increase from 2006 through 2013. For males, the age-standardized prevalence of MFS was 2.6 persons per 100,000 persons in 2013. For female, the prevalence of MFS was 1.9 persons per 100,000 persons. Few studies have reported the age-standardized prevalence of MFS overall by sex. Therefore, the results in this study cannot be compared to those from other geographic or ethnic groups. Nevertheless, the results of the present study are similar to those of earlier studies. In 2,329 MFS patients from the Taiwan National Health Insurance database from 2000 to 2012 (21), the overall prevalence of MFS was 10.2 persons per 100,000 persons.
MFS is an autosomal dominant connective tissue disorder caused by abnormal microfibrillin protein and is not sex-linked. If a parent is affected by the disorder, their offspring statistically have a 50% chance of inheriting it, regardless of whether the baby is a boy or a girl. Our results show that males had a slightly higher prevalence of MFS than females, consistent with the higher male distribution of MFS in Taiwan (58.0%) (21), Denmark (52.1%) (6), and Korean children (55.1%) (22). Therefore, more accurate hospital-based MFS registries can help verify whether these sex-based discrepancies in diagnosis are indeed accurate.
Interestingly, the peak age range of MFS prevalence was 15–19 years old overall; the prevalence peaked in 15–19 years old males and 10–14 years old females. The results of the present study correspond well with those of an earlier study; the Taiwan National Health Insurance database also showed that the highest prevalence was in 15–20 years old (21). The reason for the high prevalence of MFS in teenagers is that they physically develop and grow very actively during this stage.
We are concerned that the data obtained for this study from the Korean National Health Insurance Benefit records may not be completely accurate. For MFS patients, abnormal echocardiograms should be followed up in order to assess the size of the aorta. In Korea, the number of echocardiography devices available at hospitals or clinics registered with the National Health Insurance Service in the middle of 2013 was 21,301 among 62,853 medical institutions (20,23). In addition, 343 Korea MFS patients between 1995 and 2015 at a single tertiary medical center showed that cardiovascular manifestations such as aortic root dilatation or aortic root dissection were present in 88.6% of the patients (24). Furthermore, the FBN1 genetic test has been covered by National Health Insurance since January 2016, in Korea. Therefore, we expect that suspected MFS patients are now easily able to undergo genetic testing at a lower fee than before it was covered by insurance. To observe the prognosis and establish a treatment plan for patients with MFS, we need to assess the distribution of Marfan-related disorders such as familial thoracic aortic aneurysm syndrome, bicuspid aortic valve and ascending aortic aneurysm, Ehlers-Danlos syndrome, Loeys-Dietz syndrome, homocystinuria, congenital contractural arachnodactyly, and isolated ectopia lentis in Korea (25).
There were several limitations to our study. First, the data only included MFS. We used the primary diagnosis based on signs and/or symptoms, which may differ from the final diagnoses. For this reason, the prevalence of MFS in this study might be under- or over- estimated. Second, the National Health Insurance Benefit records may have missed potential patients with MFS who did not use medical services, paid for their own medical expenses, or had Medical Aid. Therefore, because of the trend toward increasing MFS, a hospital-based MFS registry should be developed in Korea in order to determine if our results are reproducible.
In conclusion, the age-standardized overall prevalence of MFS in 2013 was 2.27 persons per 100,000 persons (1.92 in female and 2.61 in male). And the overall age-standardized prevalence of MFS increased from approximately 1 to 3 persons per 100,000 persons between 2006 and 2013. The patterns of the prevalence of MFS in the age groups of 20–44 years-old and 45–64 years-old for both sexes showed the steady increase from 2006 through 2013. Adolescents showed a higher prevalence than other age groups, especially 15–19 years old males and 10–14 years old females. Males also showed slightly higher prevalence of MFS than females.
 XML Download
XML Download