

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Humans have the right to the highest attainable standard of health, and society has duties to protect individuals from unintentional exposure to hazards that cause health inequity. Those rights and duties are essential concepts in most international legal instruments such as World Health Organization (WHO) (1). Recently, WHO announced that involuntary smoking (IS) exposure, which has the nature of passive, environmental, or second-hand exposure, can disturb the fundamental right and freedoms of non-smokers. Because those unintentional health disturbances are deeply related to systemic social regulation for smoke-free laws, IS has been discussed in environmental justices, particularly for vulnerable subjects such as children and women (2).
Although a number of policies for protection of the general population from IS exposure have been introduced since 2000 worldwide, 58 million persons were still exposed to IS from 2011–2012 in the United States (3), and 4.9%–55.2% of the general population, including adolescents, was exposed to IS at home or in public places in Asia during the same period (4).
Previous studies have indicated that higher passive exposure to cigarette smoke leads to a higher risk of disease than secondary exposure to less cigarette smoke, but there is no ‘safe’ level of exposure to IS (35). Non-smokers are not safe from breathing IS despite opening windows, using air filters, or separating smokers from non-smokers in public spaces (3). Thus, IS exposure to non-smokers might exacerbate the environmental inequalities. Yet, surprisingly, the effects of exposure to environmental toxicants on non-smokers, which are hazardous compounds from IS, have not been closely examined, particularly cadmium.
Involuntary exposure to cadmium is a serious public health problem as it is causally related to respiratory diseases (6), several cancers (7), cardiovascular diseases (8), and toxic effects on the reproductive system and the foetus (9). Furthermore, cadmium is poorly excreted and, as it has a long biological half-life that leads to extreme accumulation, it is toxic for a relatively long time (over 20 to 30 years) for the general population (10). A previous study demonstrated the possibility of obtaining an actual cigarette addiction status using cadmium as an indicator (10). Thus, cadmium level in the blood may serve as a good reflection of the body's burden of IS exposure in the general population (11). For this reason, we have focused in the present study on non-smokers' cadmium levels out of the other cigarette-smoke-linked heavy metals.
Research into the issue of humans' early cadmium exposure from smoking has generally not been concerned with the general population or non-smokers but mainly with smokers' health problems. A previous study has analyzed exposure to heavy metals according to IS status, but it did not obtain information about the amount of exposure to IS (12). Furthermore, it did not investigate vulnerable members of the population, such as children. One study has reported an analysis of children, but it did not account for the most common sources of cadmium, such as lifestyle factors, including food consumption (13). Investigation of the level of both IS exposure and cadmium are important for the understanding of the dose-response relationship of IS hazard. However, a previous study has demonstrated this relationship only in a specific gender and age group: the adult female population (1415). Such approaches have been limited in examining the comprehensive association between IS and cadmium exposure in non-smokers.
Therefore, the primary objective of this study was to investigate the blood cadmium level in both adults and adolescents related to IS exposure with urine cotinine level, evaluated by gender stratification and considering both food consumption and IS exposure level using national representative data. We hope our investigation supports scientific evidence to discuss about the health effects of IS, including environmental justices for vulnerable populations.
MATERIALS AND METHODS
Data collection and study design
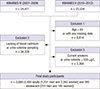
The Korea National Health and Nutrition Examination Survey (KNHANES) is a series of nationally representative, cross-sectional, and population-based surveys of the health and nutritional status of Koreans, which has been conducted by the Korea Centers for Disease Control and Prevention (16). The current study used the KNHANES IV–VI (2007–2012) survey data, which included heavy metal and urine cotinine sampling with IS exposure history. From an initial 50,405 males and females, we excluded those older than 65 years and those missing data on age, sex, sociodemographic factors (education level, occupational status, household income, and residential area), or health behavior factors (exercise level and alcohol consumption status). We further excluded those lacking blood cadmium level, urine cotinine level, IS exposure status, or with missing data or no answers given on the food frequency questionnaire. Moreover, we excluded those who were current smokers or defined as active smokers by self-report of smoking status and a biochemical marker (urine cotinine level over 550 μg/L) (17). Finally, 3,493 adults (1,231 males and 2,262 females) and 395 adolescents (210 males and 185 females) met the inclusion criteria for this study (Fig. 1).
Second-hand tobacco smoke exposure level
To investigate the IS exposure level, we used data both from a self-report questionnaire about IS status by non-smokers and urine cotinine level. The questionnaire asked about the hourly exposure level to IS in both the workplace and at home during the day in adults. In adolescents, IS level or status was not asked about in the KNHANES. Thus, we could investigate the association between self-reported IS exposure level and blood cadmium level only in adults.
A trained pathologist collected urine samples from selected participants (both adult and adolescent) in a urine specimen cup. Participants were requested to submit early morning samples when possible. All samples were stored in an icebox, which maintained a temperature of 4°C–7°C, and were transported to the permitted central laboratory. For cotinine analysis, 175 µL diphenylamine, the internal standard, was added and then 1 mL of each urine sample was hydrolyzed with 50 µL of 0.1 M sodium hydroxide and extracted with 500 µL of chloroform. After centrifugal separation (1,900 × g, 10 minutes), the residue was dried with sodium sulphite. Urinary cotinine was analysed by gas chromatographic mass spectrometry using a PerkinElmer Clarus 600T instrument (PerkinElmer, Waltham, MA, USA) (18). As part of external quality assurance and control, the German External Quality Assessment Scheme (G-EQUAS) was conducted for the measurement of urine cotinine.
Determination of cadmium in whole blood
To determine the concentrations of blood cadmium in whole blood, 3 mL blood samples were collected from each participant into a standard commercial evacuated tube containing sodium heparin (Vacutainer®; BD, Franklin Lakes, NJ, USA). For trace elements, the drawn samples were collected using an ethylenediaminetetraacetic acid tube. The concentration of blood cadmium was measured by graphite-furnace atomic absorption spectrometry with Zeeman background correction (PerkinElmer AAnalyst 600; PerkinElmer, Turku, Finland) and presented as μg/L. All blood cadmium analyses were performed by the Neodin Medical Institute, a laboratory certified by the Ministry of Health and Welfare, Korea. Internal quality assurance and control was conducted 4 times per month using 4 commercial reference materials (Lyphochek Whole Blood Metals Control; Bio-Rad Laboratories, Hercules, CA, USA) with different concentrations, and most of the results were within an allowable range. The coefficients of blood cadmium variation were within 0.95%–4.82% in the reference samples. External quality assurance and control was performed 4 times per year; the institute passed both the G-EQUAS operated by Friedrich-Alexander University and the Quality Assurance Program operated by the Korea Occupational Safety and Health Agency (19). The institute is also certified by the Ministry of Labor as one of the designated laboratories for special chemicals, including heavy metals. In this study, method detection limits for blood cadmium were 0.056 μg/L. None of the samples was below the detection limits (20).
Other covariates
Accessible covariates were different according to age group (adult and adolescent) from the KNHANES. The covariates were socioeconomic and lifestyle factors of the adult population that could affect IS status and blood cadmium level. Due to social disparities, people with lower socioeconomic status (i.e. poor education, lower household income, and poor working conditions) are more likely to be exposed to IS (21). Furthermore, the blood cadmium level of the general population is associated with socioeconomic status (22). Educational level was classified as less than middle school, high school, and college or more. Household income was calculated using standardized classification by sex, residence, and 5-year age groups, and the value was compared with the standard income level of Korean citizens. Then, the total household income was divided into quartiles. Type of residence was categorized as rural and urban areas by population size (50,000 citizens) primarily using the Korean administrative units. Occupation was categorized as white-collar workers, blue-collar workers, or unemployed. Managers, experts and related workers, and office workers were classified as white-collar workers. Workers in sales and services, agriculture, forestry, fishery, engineering, assembling, technical work, and manual labor were classified as blue-collar workers. The unemployed were included as no job, students, and homemakers.
Lifestyle factors included alcohol consumption, exercise level, and food consumption pattern, especially the high cadmium-containing food-intake status linked to blood cadmium level (23). Alcohol consumption level was classified as never, moderate, and heavy. It was defined differently according to sex. Heavy drinking was defined as at least 7 glasses of alcohol twice or more per week for men and at least 5 glasses of alcohol twice or more per week for women. Level of exercise was divided into 3 categories: none, moderate (between none and high), and high (more than 20 minutes at least 3 times per week of activity that resulted in increased respiration). Information about high cadmium-containing food consumption was obtained using a food frequency questionnaire administered by a trained nutritionist for both the adult and adolescent population. High cadmium-containing food includes seaweed, mushrooms, root vegetables, and shellfish (2224). In the present study, high cadmium-containing food consumption status was classified as less than, more than, or once per week.
Statistical analysis
The statistical analyses were conducted using SAS statistical software (version 9.4; SAS Institute, Cary, NC, USA). The age-adjusted blood cadmium levels were calculated according to baseline characteristics with stratification of age (adult and adolescent population). To explore visually the association between blood cadmium level and both the greatest risk factor (age) and potential related factor of interest (cotinine level), we used the ‘CAR’ and ‘RGL’ R packages with gender stratification. It demonstrated plotting of the regression surface that using contour or perspective plots to visualization of models with interactions (25). In the current study, we fitted a complicated model that was based on calculation of vectors with a least-squares linear regression involving a multiplicative interaction between 2-degree-of-freedom natural spline terms for a logarithm of urine cotinine level and age with gender stratification.
Regression models were performed for urine cotinine level by IS exposure level to estimate the objective exposure level of passive nicotine in non-smokers according to gender. To investigate the relationship between IS exposure level and blood cadmium, we conducted regression models for blood cadmium level by the self-reported IS status in adults, and urine cotinine level in both adults and adolescents with gender stratification. We conducted 2 regression models: an age-adjusted and a fully adjusted model. The full model was adjusted for age, sociodemographic factors (educational level, occupation, household income, and residence), and lifestyle factors (alcohol consumption, level of exercise, and high cadmium-containing food consumption, including seaweed, laver, mushrooms, root vegetables, and shellfish) for adults, and adjusted for age and high cadmium-containing food consumption (seaweed, laver, mushrooms, root vegetables, and shellfish) for adolescents. For all statistical calculations, a P value < 0.05 was considered statistically significant both tails.
RESULTS
The baseline characteristics and age-adjusted blood cadmium levels of the study population of Korean adults and adolescents are presented in Table 1. There were 1,231 (35.3%) adult men and 2,262 (64.8%) adult women, and 210 (53.1%) adolescent males and 185 (46.9%) adolescent females. In the adults, the women's age-adjusted blood cadmium level was significantly higher than the men's. The age-adjusted blood cadmium concentration was highest in the oldest group and in those with a low level of education and household income. Regarding the blood cadmium concentration in the occupational category, it was significantly higher in the unemployed, followed by white-collar workers and then blue-collar workers. In the case of alcohol consumption and level of exercise, the ‘never’ alcohol intake and non-exercising groups of participants showed a significantly higher level, followed by those with heavy alcohol intake and moderate exercise. No significant differences were found for residence. The blood cadmium level was highest in those exposed to IS. It was also highest when there was more intake of high cadmium-contained food per week and when urine cotinine concentration was higher. Gender and age did not show any significant correlation with blood cadmium level in the adolescent group. However, the same result was found as for the adult group regarding consumption of cadmium-containing food per week and urine cotinine level.
Table 1
Baseline characteristics of study participants

IS = involuntary smoking.
*P value for statistical different of age adjusted blood cadmium level (μg/L) by each category; †Cadmium contained food included seaweed, mushrooms, root vegetables, and shellfish.
![]()
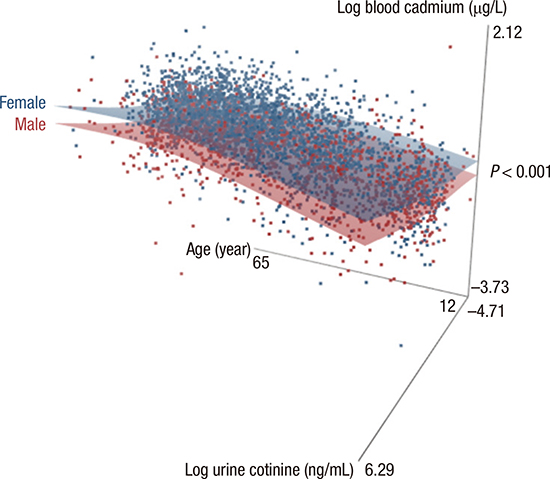
A 3-dimensional scatter graph that shows the fit to the regression model is presented in Fig. 2. There was a significant visual positive correlation of blood cadmium level with age and urine cotinine level in both men and women. In addition, there was a significant difference of the fit to the model between men and women (P < 0.001). The model fit of the blood cadmium level of women had a higher relationship with urine cotinine level and age (blue dots and blue surface) than that of men.
 | Fig. 2The 3-dimensional scatter graph with fit models for the blood cadmium level related with both age and urine cotinine level according to gender.
|
As shown in Table 2, there was no statistically significant association between blood cadmium levels and the level of exposure to IS in both adult men and women. However, IS exposure level was significantly related to urine cotinine level in all of regression model l. In adults, after controlling for age, socio-demographics, lifestyle factors, and high cadmium-contained food intake, each 1 hour per day exposure to IS was associated with 2.7252 (± 1.2769) and 5.4270 (± 0.7733) ng/mL increase in urine cotinine level in men and women respectively. There were still statistically significant linear correlations between blood cadmium level and urine cotinine level in all strata after full adjustment. In adults, the results of fell adjusted model showed that increasing each 1 ng/mL of urine cotinine level did elevate 0.0004 (± 0.0001) and 0.0006 (± 0.0002) μg/L of blood cadmium level in men and women respectively. Furthermore, adolescents also showed a statistically significant positive correlation between urine cotinine level and blood cadmium level; 0.0006 (± 0.0002) in boy and 0.0016 (± 0.0006) in girl.
Table 2
Results of regression models relating urine cotinine level and blood cadmium level to IS exposure

IS = involuntary smoking, B = effect value, SE, standard error.
*Adjusted for age, sociodemographic factors (educational level, occupation, house hold income, and residence), life style factors (alcohol drinking, level of exercise, and high cadmium-contained food-intake status including seaweed, mushrooms, root vegetables, and shellfish for adult and adjusted for age and high cadmium-contained food-intake status (seaweed, mushrooms, root vegetables, and shellfish) for adolescent; †P value < 0.05; ‡P value < 0.01.
![]()
DISCUSSION
Our nationwide cross-sectional study showed that the relationship between urine cotinine level and blood cadmium level was statistically significant. Moreover, this association was not attenuated even after the adjustment of potential confounders, including particularly high cadmium-containing food consumption status. Such a link was also observed in both genders and even in the adolescents who have susceptibilities to environmental toxicants.
The inequality of exposure level and its health effect among different socioeconomic systems is one of the starting factors of environmental justice. Environmental exposure to smoke in Korea is merely unintentional and merely depends on social systems including smoke-free regulation laws. Furthermore, our study shows the IS exposure related to increment of blood cadmium level in both genders and even in adolescents. Because many advanced societies made rules that severely restricted IS exposure from non-smokers, particularly from vulnerable humans such as adolescents, even public open areas potentially accessible to the general population are defined as smoke-free zones. However, our study reported that non-smokers are exposed to IS and those exposures also show potential health effects which are related to blood cadmium. Furthermore, because the blood cadmium level was increased in adolescent non-smoker women, who are our future, urgent social concern is needed to prevent health effects of IS.
In our study design, we excluded active or current smokers using both a self-reported questionnaire and urine cotinine level. Urine cotinine level can be a biochemical indicator of current exposure to IS in non-smokers. Cotinine is a key metabolite of nicotine, with a half-life of about 20 hours, which can be measured in blood, saliva, hair, and urine, and is therefore a reliable and useful biochemical marker of current nicotine exposure from smoking (2627). Thus, the observed increase in blood cadmium level could be attributed to passive exposure to cigarette smoke in non-smokers.
Cadmium can be absorbed into the body through multiple routes, including inhalation, ingestion, and directly through the skin. Inhalation is considered the main exposure route in non-smokers. Up to 50 percent of cadmium released from burning cigarettes can enter the body by inhalation (14). The main target organ of inhaled cadmium toxicity is the lung. In the lung, cadmium is efficiently absorbed when inhaled in cigarette smoke by cadmium oxide, which is highly bioactive when generated during the burning of cigarettes (28). Cadmium oxide particles affect the gene expression of several different inflammation inducers and trigger pulmonary cell apoptosis even at fairly low concentrations in humans (29). In addition, a previous study indicated that even very short-term inhalation of cadmium oxide particles could produce persistent pulmonary cell injury and stimulate pathways in the lungs associated with inflammation, as well as alter systemic immune function (30). These mechanisms of pulmonary irritation by inhaled cadmium seem to be involved in the development of many lung and systemic diseases.
Recent epidemical evidence has suggested that the cadmium level in the human body is closely related with smoking rate changes. In the United States' general population, the cadmium level declined markedly over 2 decades (1988–2008), and the smoking rates and changes decreased with a similar trend in the same period, which might importantly have been caused by reducing exposure to tobacco smoke for both smokers and non-smokers (31). In addition, blood cadmium level was usually assessed using whole blood and was considered the most valid marker of recent exposure (32). A previous research indicated the possibility of obtaining an actual cigarette addiction information of smokers using cadmium as an indicator (10). According to our present research, blood cadmium level was significantly related to urine cotinine level in non-smoker groups including both adolescent and adult. Thus, cadmium level in the blood may serve as a good reflection of the body's burden of IS exposure in the general population (11).
The finding that blood cadmium level was closely associated with urine cotinine from IS exposure offers some important insights into the control of smoking for non-smokers. It indicates that the IS exposure level can be checked using urine cotinine, although it is still difficult to know whether it is linked with the severity of IS exposure. Cadmium could be an important indicator of the harmfulness of IS to the general non-smoking population as smokers'. Although we did not find a statistically significant direct association between self-reported IS exposure level and blood cadmium level, we can suggest that cadmium level might be useful for understanding, examining, and preventing public health concerns about IS through the relationship between urine cotinine level and blood cadmium level.
Another important finding was that there were gender and age group differences in the regression models. Women and adolescents had higher estimates for blood cadmium level according to urine cotinine level than men and the adult population in the final regression model. It is possible that these results are due to gender differences of the body burden for cadmium. Women have a higher cadmium body burden than men from the highly increased absorption of environmental cadmium into the body due to lower iron stores (33). This indicates that women are more vulnerable than men to IS even with the same exposure level. Furthermore, it is a serious public health concern because women exposed to IS can develop an unhealthy status not only as individuals but also in the next generation due to an irritated reproductive system from involuntary cigarette smoke exposure (34).
Regarding the biology of adolescence, it is important to prevent exposure to IS. The maturation of several whole organ systems including not only the reproductive system but also the skeletomuscular, respiratory, immune, and central nervous systems occurs during this period. Differences in body surface, blood volume level, metabolic needs, and both sensitivity and capacity all contribute to an altered exposure level for toxicity of IS (35). Furthermore, our study demonstrated that the blood cadmium level by IS of adolescents had higher effect values than that of adults in both genders. As their bodies and minds are developing, adolescents (who are our future) are especially vulnerable to the hazardous effect of IS. Thus, more proactive strategies for preventing IS exposure are needed that focus on women who have a high body burden for IS and adolescents who are vulnerable to the exposure to IS.
These findings may be somewhat limited by the study design. We adjusted or stratified many possible confounders including age, sociodemographic factors, and lifestyle factors with both gender and age group, which could have an effect on the level of blood cadmium. However, it is uncertain if there was another potential source of cadmium exposure. For example, blood cadmium level could be affected by working tasks (smelting, plating, and welding) and living area conditions (air and water) (3637). Furthermore, we only could investigate blood cadmium linked to IS without urine cadmium level. The blood cadmium level was known to reflect longer-term exposure that accumulates in the blood stores over a 10-year period. On the other hand, the urine cadmium level reflects recent exposure. Thus, it is important to bring a clinical implication of IS exposure to non-smokers that to measure and to analyze IS exposure level with both urine and blood cadmium level. Unfortunately, these data about occupational characteristics or urine cadmium level were not accessible because of the nature of the KNHANES data. In addition, we used both self-reported IS level and urine cotinine level to evaluate the exposure level to IS. Only urine cotinine level was related to blood cadmium level with statistical significance. Our current study might be biased due to using the self-reported questionnaire, which might be misleading regarding the statistical association between blood cadmium level and self-reported IS status. Nevertheless, as we found a significant association between IS and blood cadmium level after adjusting for potential confounders as much as possible in all age groups and both genders for the first time, its clinical implications may not be attenuated by these limitations.
The present study makes several noteworthy contributions to the public issues of preventing and understanding IS exposure in general non-smokers (both adults and adolescents) using national representative data with gender stratification for the first time. Greater efforts are needed to improve environmental justices regarding IS, especially women and adolescents, considering the severe harmful effects of involuntary exposure to even a low level of cadmium.
 XML Download
XML Download