

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Cap polyposis was first described by Williams et al. (1) in 1985. Thereafter, about 60 sporadic cases of cap polyposis have been reported in the literature, but it is rarely observed in children. A case series showed that patients' median age was 52 years and the age range was from 12 years to 76 years (2). Li et al. (3) reported the youngest case of cap polyposis in a 5-year-old male in 2013. The most common site of polyposis is the rectosigmoid colon, but lesions have also been detected proximal to the colon and in the stomach (4). Macroscopic findings include sessile and erosive polyps, dark red in color with fibrous, purulent, and mucoid discharge. An inflammatory and fibrinopurulent mucous cap of granulation tissue is a special histopathological feature of this disease. The etiology and curative treatment remain unknown to date.
An epidermal nevus is a hamartoma which is defined as hyperplasia of the epidermis in any part of the body. An epidermal nevus manifests as a yellowish, discrete papillomatous plaque or papule, and is classified according to the cellular component. It may be classified into apocrine, eccrine, sebaceous, follicular, or keratinocytic type. Epidermal nevus syndrome is a sporadic neurocutaneous disease with associated ectodermal defects in the brain, eyes, and skin (5). Herein, we present an extremely rare case of cap polyposis in an infant with an epidermal nevus and provide a review of the literature.
CASE DESCRIPTION
An 11-month-old male patient visited our pediatric department because of rectal prolapse and intermittent bloody stools, in September 2014. He presented with eventration of a reddish mass with intermittent fibrous and purulent exudation from the anus. He was born through cesarean section at 38 weeks of gestation, and his birth weight was 3,890 g. He had received all scheduled vaccinations. At 10 months of age, he was diagnosed with an epidermal nevus which was confirmed through biopsy at our hospital. The skin lesion was located in the sacral area (Fig. 1). The patient's parents reported no familial history of gastrointestinal polyps or carcinomas.
 | Fig. 1This picture shows asymmetric, bright, brown colored, diffuse groups of verrucous plaque, and an elevated macular epidermal nevus located in the lower back and sacral area.
|
He did not have any symptoms such as constipation or diarrhea. Also, his growth was normal. Laboratory test results were as follows: hemoglobin, 12.7 g/dL; hematocrit, 37.6%; platelets, 227,000/μL; protein, 6.8 g/dL; albumin, 4.7 g/dL. The serum levels of tumor markers such as carcinoembryonic antigen (CEA), α-fetoprotein (AFP), and CA 19-9 were within the normal range. His thyroid function test was normal. Plain radiographs of the abdomen and the chest showed normal findings. In the abdominal and pelvic computed tomography (CT) scan, well-enhanced multiple polypoid lesions, each about 1 cm in size, were seen at 4 to 6 cm above the anal verge. Enlargement of regional lymph nodes and lymph nodes of both iliac chain areas was noted. CT images suggested the possibility of rectal cancer (T3, N1) with metastasis (Fig. 2). However, brain magnetic resonance imaging showed normal findings. Hence, we concluded that he did not have metastatic malignancy or neuroanatomical abnormality.
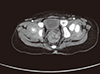 | Fig. 2CT image shows well-enhanced, multiple polypoid lesions about 1 cm in size located at 5 cm above the anal verge. Multiple lymph node enlargement was noted.
CT = computed tomography.
|
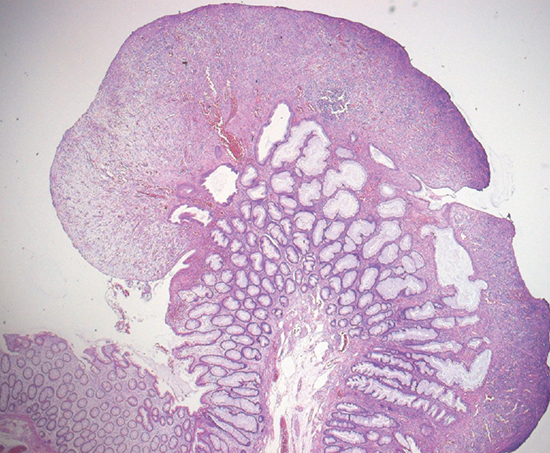
Further evaluation with barium enema study showed several polypoid lesions without stalks in the anus (Fig. 3). A barium swallow study revealed normality of the stomach or the small bowel. Anorectal manometry showed normal pressure within the rectum and anus. The rectoanal inhibitory reflex was normal. The upper gastrointestinal endoscopy and colonoscopy were performed under anesthesia. Colonoscopy revealed variously sized polypoid lesions without stalks in the anus (Fig. 4). Histological findings revealed reactive lymphoid hyperplasia and multiple polyps with hyperplastic crypts covered with granulation tissue, and showing dystrophic calcification (Fig. 5). Normal mucosa was noted on the upper gastrointestinal endoscopy. He had no evidence of Helicobacter pylori infection in the Campylobacter-like organism test (CLO test), a serologic antibody test. The polypoid lesions were removed through transanal polypectomy. Three multilobulated polyps were located 1 cm above the anal verge at the 7 o'clock position, 3 cm above the anal verge at the 5 o'clock position, and 3.5 cm above the anal verge at the 4 o'clock position, respectively. Under general anesthesia, these polyps were completely removed by electrical cauterization using the Bovie cautery.
 | Fig. 3Barium enema study shows multilobulated mass-like mucosal lesions in the recto-anal area. There was no evidence of mucosal destruction or obstruction from the rectum to the ascending colon.
|
 | Fig. 4Multilobulated, 4–6 cm in size polypoid groups were seen from the anus to the proximal rectum on colonoscopic view.
|
 | Fig. 5Hyperplastic crypts covered with calcified granulation tissue were revealed on histologic examination (H & E, ×100).
H & E = hematoxylin and eosin.
|
After surgical treatment, he did not have hematochezia for 5 months. Afterwards, he experienced recurrent bloody and mucoid stools. Colonoscopy revealed very small polypoid lesions at the previous location (Fig. 6). The lesions were too small to be removed through surgery. After mesalazine enema was administered, his clinical symptoms improved, and he no longer had bloody stools. At two months after recurrence, endoscopy showed that the size of polyps had decreased. Daily mesalazine enema was continued for 6 months prior to its discontinuation. The patient did not have any relapse for more than 12 months thereafter.

DISCUSSION
Cap polyposis is a very rare disease characterized by hematochezia or mucoid diarrhea. There are several case reports of cap polyposis in adults, but only few cases have been reported in children. In particular, a case of cap polyposis in an infant has not been reported. We herein described a case of an 11-month-old infant with localized cap polyposis in the rectoanal area causing hematochezia. He may be the youngest patient diagnosed with cap polyposis in the literature to date. In infants, more common causes of bloody and mucoid stools are infectious gastroenteritis, intussusception, anal fissure, and allergic proctocolitis. However, he had moderate amount of hematochezia and mucoid stools. Prolapsed mucosa suggested rectal masses.
There is no clear explanation of the etiology. Several causes have been investigated in occasional case reports. Suspected causes of cap polyposis include abnormal motility of the colon, chronic straining at stool, mucosal prolapse, infectious agents such as H. pylori and immune disorders. Naturally, the treatment of polyposis also varies according to the suspected cause, and the optimal management has not been established. The mucosal lesions in some patients were healed with metronidazole, suggesting that an infectious pathogen might play a role in focal inflammation (6). But Suzuki et al. (7) reported that the efficacy rate of metronidazole treatment was only 28.6% (6/21 cases). Although the results were from only small reports, the effectiveness of metronidazole as single therapy seemed unsatisfactory. In our case, there was no evidence of systemic inflammation such as leukocytosis or elevated C-reactive protein level. Furthermore, no infectious organism was detected in the stool culture or multiplex PCR.
H. pylori infection has been implicated in the etiology of cap polyposis (89). The researchers suggested that H. pylori eradication indicates successful management of these patients. In 2002, Oiya et al. (8) first described H. pylori eradication therapy in a patient with cap polyposis. A 63-year-old man was diagnosed with cap polyposis and intestinal metaplasia associated with H. pylori by gastroscopy. After H. pylori eradication, follow-up colonoscopy revealed that the elevated mucosal cap lesions had disappeared. This indicated that the immune response to persistent H. pylori infection may be the cause of cap polyposis (8). In 2004, Akamatsu et al. (9) reported three cases of cap polyposis that were treated successfully with eradication therapy. They reported that Ménétrier's disease is related to H. pylori infection, and it has histological findings that are similar to cap polyposis (9). In 2014, Suzuki et al. (7) reported that the efficacy of H. pylori eradication therapy in treating cap polyposis was 100% (14/14 cases), and they strongly recommended it. But in our case, the patient showed no evidence of H. pylori infection in gastric mucosal biopsy. Mucosal prolapse syndrome is a group of benign chronic inflammatory diseases that includes rectal prolapse, solitary rectal ulcer syndrome, inflammatory polyps, and proctitis cystica profunda (10). These diseases are caused by an increase in anal pressure during defecation and chronic excessive straining due to constipation. Cystica profunda of the rectum is characterized by fibromuscular obliteration, hyperplastic glands, and mucin cystic change in the submucosal layer (11). Because of the histological similarity between mucosal prolapse syndrome and cap polyposis, chronic mechanical injury to the mucosa due to abnormal motility has been suggested as a crucial etiological factor in the pathogenesis of cap polyposis. The avoidance of excessive straining during defecation has been reported as a successful treatment strategy in some cases (12). On the other hand, some authors reported that chronic straining or constipation was noted in only 7 out of the 11 patients (64%) (13). Also, the infant in our case report showed normal results in the anorectal motility study, no constipation, and no evidence of abnormal motility of the colon.
Steroids, aminosalicylates such as 5-ASA, and infliximab have been used to treat cap polyposis. Abnormal mucus in cap polyposis is similar to mucosal inflammation in ulcerative colitis. The author suggested that helper T-cell mediated inflammation is the mechanism for explaining the pharmacodynamic effectiveness of steroids or infliximab (14). However, there are many reports on the failure of steroids or infliximab (1315). Consequently, it is controversial whether steroids or infliximab should be administered uniformly. Even close observation without medication has resulted in spontaneous regression of polyposis (7). There has been no evidence of malignant transformation of cap polyposis. We speculate that the disease may have a self-limiting course or it may have many deteriorating causes. Symptom-alleviating surgical removal is usually needed in patients with cap polyposis. The optimal timing for surgical removal is still under discussion. If patients have refractory or recurrent symptoms despite medical treatment, the attending surgeon should consider total colectomy (613). After complete polypectomy in patients with a few polyps (less than 10 polyps), patients are generally symptom-free for several years (13). In some patients, polyps regrow even after surgical removal. Preoperative colonoscopy should be performed for identifying the current status of the disease and for planning the extent of surgical resection. If a patient has persistent symptoms for three months in spite of medical treatment, surgical removal should be performed (16).
To the best of our knowledge, the relationship between cap polyposis and epidermal nevus has not been explored in the relevant literature. The skin and the gastrointestinal tract are derived from the ectoderm. Hence, some skin lesions are associated with intestinal diseases. For example, Proteus syndrome is characterized by epidermal nevus and colonic hamartomas (17). A case of Gardner syndrome with epidermal nevus reported by Romiti et al. (18) is another example. Gardner syndrome is a type of colonic adenomatous polyposis with extracolonic benign lesions that include cutaneous epidermal cysts, fibromas, osteomas, and dental abnormalities. In our case, there may be an association between sacral epidermal nevus and cap polyposis or there was simple incidental coexistence of the two conditions. Because cap polyposis is a very rare disease, no large-scale study has been conducted, let alone a case of cap polyposis in an infant. Nevertheless, investigation of cap polyposis in children is necessary. The infant in our case report remains in remission after 5-ASA enema that was tried in response to postsurgical recurrence. Close observation is warranted until adulthood.
 XML Download
XML Download