

 PDF
PDF ePub
ePub Citation
Citation Print
Print




INTRODUCTION
Helicobacter pylori is the main causative agent of gastric diseases, and there are various tests for diagnosing infection. In an endemic area of H. pylori infection, chronic atrophic gastritis (CAG) and metaplastic gastritis (MG) may lead to a low sensitivity for invasive tests due to the low density of H. pylori population on the gastric biopsied samples (12). To avoid the risk of false negative findings of invasive tests, adding noninvasive test such as serum anti-H. pylori immunoglobulin G (IgG) assay is recommended (34). Although serology testing cannot distinguish between current and past infections, it is reliable in endemic areas of H. pylori infection where the prevalence of CAG and MG is high (5).
The serum pepsinogen (PG) assay is used for the diagnosis of gastric corpus atrophy, based on the concept that there is a stepwise PG I/II ratio reduction with a progress of atrophic gastritis from the antrum to the corpus (67). The serum PG assay estimates the secreting ability of the gastric mucosa cells, and therefore, it is useful when selecting asymptomatic subjects for endoscopy surveillance before and after the resection of gastric neoplasm (78910). Nonetheless, there are still controversies with regard to the link between the serum PG assay findings and abnormal upper gastrointestinal (UGI) endoscopic findings.
Important UGI endoscopic findings related to active H. pylori infection are gastric ulcer (GU), duodenal ulcer (DU), and nodular gastritis (NG), while those related to chronic infection are CAG and MG (11). On the other hand, erosive esophagitis (EE) is more common in the absence of H. pylori infection (12). The aim of this study was to elucidate the significance of serum PG assay findings for correlating with endoscopic findings, and its association with H. pylori-seropositive test findings.
Go to : 
MATERIALS AND METHODS
Subjects
Koreans who visited our center between 2010 and 2015 were enrolled consecutively in this cross-sectional study. Subjects were included if the serum PG assay, serum anti-H. pylori IgG test, and UGI endoscopy were performed on the same day at our center. The exclusion criteria were being younger than 18 years, being pregnant, having a history of gastrectomy or successful H. pylori eradication, having significant disease(s) that should be managed promptly, or incomplete finding in any of the performed tests. After the endoscopic examination, subjects were excluded if there was an adenoma or adenocarcinoma on the gastric biopsied specimen.
Serum PG assay
Blood samples were obtained from the patients after 12 hours of fasting before UGI endoscopy. The samples were centrifuged and stored at −70oC before analysis. Serum PG I and PG II concentrations were analyzed using the latex-enhanced turbidimetic immunoassay (HBi, Anyang, Korea) as described (8).
H. pylori serology test
The serum anti-H. pylori IgG titer was measured using the Vidas H. pylori IgG assay (BioMérieux, Marcy-l'Etoile, France) until 2012, and using the Chorus H. pylori IgG assay (DIESSE Diagnostica Senese, Siena, Italy) thereafter. All of these tests were performed using the same blood sample with that of the serum PG assay according to the manufacturer's instructions (13). For the Vidas H. pylori IgG assay, the result was considered positive when test value (TV) of ≥ 1.00 and negative if TV of < 0.75. According to the Vidas H. pylori IgG assay package insert, the sensitivity and specificity of this test were 98.1% and 90.8%, respectively. For the Chorus H. pylori IgG assay, the yielded values lied in the range from 0 to 200 arbitrary units (AU)/mL. If the value exceeds the upper limit, it was expressed as > 200 AU/mL. The result was considered positive if a serum anti-H. pylori IgG titer of ≥ 12.0 AU/mL and negative if < 8.0 AU/mL. A were defined as a seropositive finding. The sensitivity and specificity were 89% and 100%, as claimed on the package insert.
Endoscopic examination
UGI endoscopy was performed at our center by one of the board-certified attending gastroenterologists using either a GIF-H260 (Olympus, Tokyo, Japan) or an EG-2990i (Pentax, Tokyo, Japan) endoscope. Endoscopic findings were initially described based on the criteria of the Sydney classification, and additional findings were recorded. With regard to the background gastric mucosa, the presence of H. pylori-related endoscopic findings was recorded (Fig. 1). NG was defined as chicken-skin like mucosal changes on the antrum. CAG was diagnosed when there was permeability of blood vessels with an atrophic border. MG was defined as whitish patches with or without depressed hyperemic lesions. GU and DU were diagnosed as a deep mucosal defect suspicious for submucosal invasion. An old ulcer scar due to a past history was not included as GU or DU subject in this study. A diagnosis of EE was made only when there was an erosion (hyperemic streak) on the low esophagus.
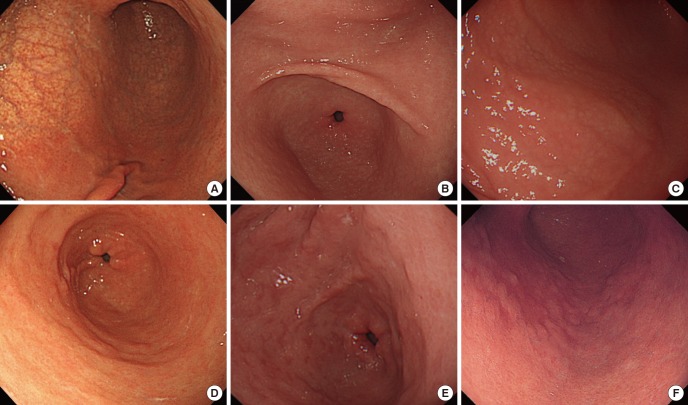 | Fig. 1Diagnostic criteria used for discriminating endoscopic findings of H. pylori-related gastritis on the background gastric mucosa. (A) CAG. Transparent vessels are visible from the lesser curvature side to the anterior wall of the antrum extending up to the low-body with a demarcation line, so-called atrophic border. (B) NG on the antrum. Multiple and tiny, colorless nodules are scattered. The shape and size of the nodules are regular. (C) NG on the body. The nodules may extend up to the body, since they are submucosal protrusions that consist of lymphoid follicles. (D) MG with whitish color change. Large-sized, whitish elevations are noticed on the antrum. The shape and size of the discolored lesions are irregular. (E) MG with hyperemic color changes. Multiple, hyperemic depressions are augmented by irregular, whitish surrounding mucosa which indicates intestinal metaplasia. (F) MG on the body. Intestinal metaplasia has variable appearances from irregular, whitish elevations to geographic, hyperemic depressions.
CAG = chronic atrophic gastritis, MG = metaplastic gastritis, NG = nodular gastritis.
|
Statistical analysis
All analyses were conducted using PASW Statistics 17.0 (SPSS Inc., Chicago, IL, USA), and the threshold for statistically significance was set at P value < 0.05. Categorical variables are presented as frequency (%) and differences were assessed using the χ2 test. Continuous variables are presented as mean ± standard deviation values and were assessed using Student's t-test. Differences among the groups were analyzed by analysis of variance (ANOVA) with Bonferroni correction for numerical variables, and χ2 test with Bonferroni correction for categorical variables. Linear regression analyses were performed to verify the significance on the continuous variables including the serum PG concentrations.
Ethics statement
All procedures were in accordance with the ethical standards of the Konkuk University Medical Center of Institutional Review Board (institutional approval No. KUH1010290 and national approval No. KCT0000719) and with the Helsinki Declaration of 1964 and later versions. Informed consent or substitute for it was obtained from all patients for being included in the study.
Go to :
RESULTS
Characteristics of the included subjects
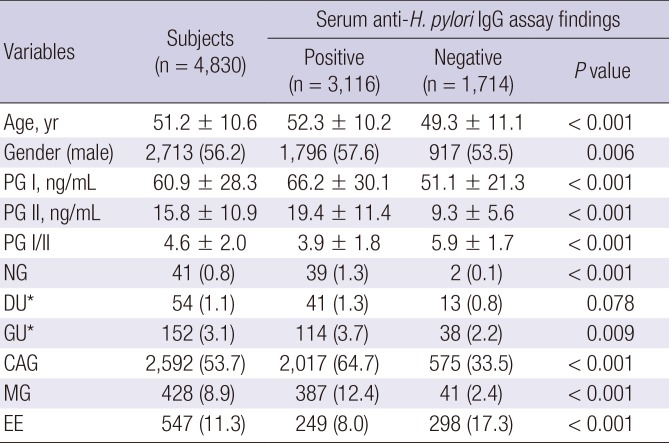
Of the 5,301 potential subjects, 275 were excluded due to a history of successful H. pylori eradication, and 169 were excluded due to equivocal serology test findings. Based on the endoscopic biopsy findings, 12 subjects were excluded due to adenocarcinoma and 15 subjects were excluded due to adenoma (Fig. 2). The remaining 4,830 subjects were classified into 2 groups based on their serum anti-H. pylori IgG test findings (Table 1). Significant differences were found between the seropositive and seronegative subjects with regard to the age (P < 0.001) and gender (P = 0.003). The prevalence of NG (P < 0.001), GU (P = 0.009), CAG (P < 0.001), and MG (P < 0.001) were higher in the seropositive group. Conversely, that of EE was higher in the seronegative group (P < 0.001).
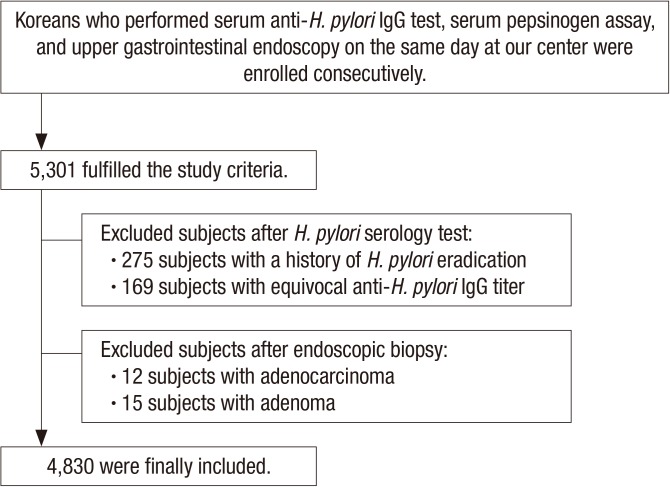 | Fig. 2Flow of the study. Subjects with a history of successful H. pylori eradication were excluded from the beginning due to an altered serum PG assay finding after the eradication. After the evaluation, subjects with an equivocal H. pylori serology test finding and those who were confirmed as adenoma or adenocarcinoma were excluded.
IgG = immunoglobulin G, PG = pepsinogen.
|
Table 1
Baseline characteristics of the included subjects
Data are shown as mean ± SD or number of subjects (%).
IgG = immunoglobulin G, SD = standard deviation, PG = pepsinogen, NG = nodular gastritis, DU = duodenal ulcer, GU = gastric ulcer, CAG = chronic atrophic gastritis, MG = metaplastic gastritis, EE = erosive esophagitis.
*These consist of 54 DU (22 active and 32 healing stages) and 152 GU (52 active and 100 healing stages). DU scar (n = 72) and GU scar (n = 110) were excluded from the analysis.
![]()
Distribution by the endoscopic findings
There were 152 subjects with GU (52 active-stage and 100 healing-stage) and 54 subjects with DU (22 active-stage and 32 healing-stage). Subjects with GU were male-predominant (P < 0.001) and showed higher prevalence of seropositive finding (P = 0.009) than those without GU (Table 2). The serum PG I concentration (P < 0.001) and PG II concentration (P = 0.028) were higher in the GU subjects than the counterparts. In similar, subjects with DU were male-predominant (P < 0.001) and showed higher serum PG I concentration (P = 0.009) than those without DU. Although it was statistically insignificant (P = 0.078), seropositive finding was more common in the subjects with DU (75.9%, 41/54) than those without DU (64.4%, 3,075/4,776).

Table 2
Characteristics of the subjects according to the endoscopic findings
Data are shown as mean ± SD or number of subjects (%). Statistically significant values are highlighted in bold.
PG = pepsinogen, NG = nodular gastritis, DU = duodenal ulcer, GU = gastric ulcer, CAG = chronic atrophic gastritis, MG = metaplastic gastritis, EE = erosive esophagitis.
*Higher than the subjects without particular endoscopic finding (P < 0.05). †Lower than the subjects without particular endoscopic finding (P < 0.05).
![]()
NG was more common in young-aged (P < 0.001), women (P < 0.001), and those with H. pylori seropositive finding (P < 0.001). The serum PG I (P < 0.001) and PG II (P < 0.001) concentrations were higher, while PG I/II ratio was lower (P = 0.044) in the subjects with NG than those without NG. Of all endoscopic diagnoses, NG showed the highest serum PG I and PG II concentrations (Table 2).
The subjects with CAG or MG were elder (all P < 0.001), and showed higher prevalence of H. pylori-seropositive finding (all P < 0.001). A higher serum PG concentrations and a lower PG I/II ratio (all P < 0.001) were found in the subjects with CAG. Furthermore, the PG I/II ratio (P < 0.001) was inversely correlated with the presence of MG.
With regard to EE, subjects with EE were male-predominant (P < 0.001) and showed higher prevalence of seronegative finding (P < 0.001) than those without EE. The serum PG II concentration (P < 0.001) were lower in the EE subjects, while PG I/II ratio (P < 0.001) were higher than the subjects without EE.
Significant variables for a specific endoscopic finding
After adjusting age and gender of the subjects, a higher serum PG I concentration was an independent predictive factor for the presence of NG (P = 0.003) and GU (P = 0.003) on linear regression analyses (Table 3). Moreover, a higher serum PG II concentration was related to the presence of NG (P = 0.003) and CAG (P < 0.001), independently. CAG and MG were inversely correlated with serum PG I/II ratio (all P < 0.001). Conversely, EE was correlated with a decreased PG II concentration (P < 0.001) and an increased PG I/II ratio (P < 0.001).
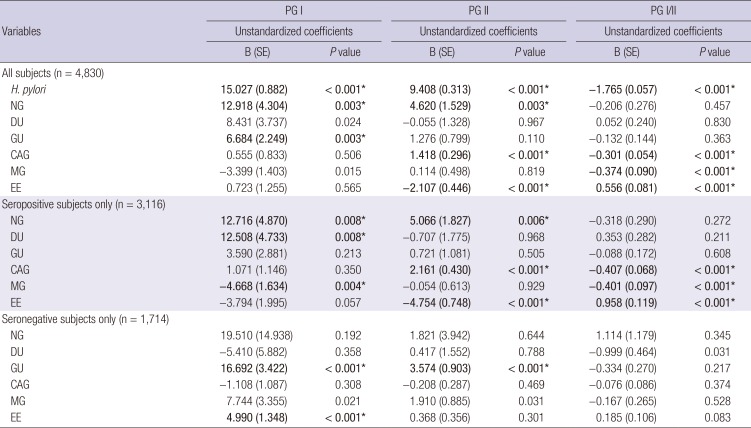
Table 3
Variables related to the serum PG assay findings after adjusting age and gender
Significant values are highlighted in bold.
PG = pepsinogen, SE = standard error, NG = nodular gastritis, DU = duodenal ulcer, GU = gastric ulcer, CAG = chronic atrophic gastritis, MG = metaplastic gastritis, EE = erosive esophagitis.
*Statistical significance was considered as a P = 0.008 after the post-hoc analysis.
![]()
Different findings between the seropositive- and seronegative-subjects
The serum PG I (P < 0.001) and PG II (P < 0.001) concentrations were significantly higher and the serum PG I/II ratio (P < 0.001) was lower in the seropositive group than in the seronegative group. In the 3,116 seropositive subjects, significant correlations found between the serum PG assay and endoscopic findings were similar to those found in the entire subjects.
When analyzed only for the 1,714 seronegative subjects, the correlations found between endoscopic findings and serum PG concentrations were no longer significant, except for the link found between GU and serum PG I concentration. The serum PG I (P < 0.001) and PG II (P < 0.001) concentrations were positively correlated with GU. Furthermore, correlation was found between the serum PG I concentration and EE (P < 0.001) only in the seronegative subjects.
Go to :
DISCUSSION
Our study findings demonstrate that the serum PG assay findings are related to endoscopic findings both in the seropositive and seronegative subjects. The serum PG concentrations differed between the endoscopic findings related to active H. pylori infection (NG, DU, and GU) and those related to chronic infection (CAG and MG). A higher serum PG concentration indicated an increased risk for NG and peptic ulcer disease, while a lower serum PG concentration indicated an increased risk for EE than a higher PG concentration. Moreover, serum PG assay findings were independently correlated with the endoscopic findings in seronegative subjects. Increased serum PG I concentration in seronegative subjects with EE or GU suggest that endoscopic findings reflect gastric secreting ability.
Of the several H. pylori-associated endoscopic findings, NG is closer to an active-staged infection than CAG and MG which are found during a long-term, chronic infection (11). In our study findings, CAG and MG showed lower serum PG I/II ratios than NG. Furthermore, serum PG concentrations were higher in NG, DU, and GU, indicating an increased gastric secreting ability of the gastric mucosa. Since most of NG are found in the subjects with an active H. pylori infection, the correlation between NG and serum PG concentration was no longer significant in our seronegative subjects. In similar, positive correlations between DU and PG I concentration were found only in seropositive subjects, and not in seronegative subjects. In seronegative subjects, significant correlation was found only between GU and serum PG I. This exceptional link may be due to a higher incidence of H. pylori-negative ulcer in the stomach than the duodenum (14).
In subjects with chronic H. pylori infection, the findings of endoscopic, histological, and serological atrophic gastritis are known to be well-correlated (15). Notably, there were 2 different serum PG assay findings between CAG and MG in this study. The serum PG I concentration was decreased in MG, while the serum PG II concentration was increased in CAG. A higher serum PG II concentration in CAG indicates that gastric secreting ability is still preserved throughout the stomach. Besides, a lower serum PG I concentration in MG denotes decreased gastric secreting ability due to the progress of gastric corpus atrophy. Interestingly, a lower serum PG I concentration in MG was significant only among the seropositive subjects. This might be attributable to a long-term, persistent infection that leads to gastric corpus atrophy in seropositive subjects.
Of the several endoscopic diagnoses, the serum PG assay findings of EE were mostly similar to those of the normal findings. The serum PG concentrations and H. pylori-seropositive test findings were lowest in subjects with EE as previous study (12). A recent large-sized study showed that H. pylori infection is not related to EE, although the prevalence of EE is increasing in Korea (16). In our EE subjects, a lower serum PG II concentration and a higher PG I/II ratio were observed. Interestingly, these findings were significant only in seropositive subjects. In seronegative subjects, a higher PG I concentration was found in EE. These findings suggest that EE is not attributable to H. pylori infection, and there is no excessive PG secretion in seropositive subjects. Nevertheless, mucosal breaks on the low esophagus may be attributable to gastric inflammation of the fundus by stimulating gastric mucosa to secrete PG I in seronegative subjects. Such an intact gastric secreting ability can be found in seronegative subjects, because gastric mucosal cells are not damaged by H. pylori infection.
Endoscopic diagnoses differed significantly between the H. pylori-seronegative and -seropositive subjects in this study. Previous studies have shown that H. pylori-related gastritis can be evaluated using serum PG levels (1718). Besides the detection of atrophic gastritis using the serum PG assay findings (1920), an increased PG II concentration indicates H. pylori-infected condition which consists of an ongoing active infection (1821). Their findings are consistent with our study that a high PG concentration is significantly correlated with NG, while it is inversely related to EE in seropositive subjects.
In our H. pylori-seronegative subjects, increased PG I and PG II concentrations were correlated only with GU among all endoscopic findings. These suggest that an extremely high gastric secreting ability is found in a H. pylori-naïve stomach when an ulcer develops. The recent increase of H. pylori-negative ulcers may be attributable to drugs, toxic foods, systemic complications, or psychological stress that stimulate gastric mucosal cells (14). In similar, EE was correlated with PG I concentration, but not with PG II concentration in seronegative subjects. PG I is secreted only from the fundus, while PG II is secreted throughout the stomach and also from the duodenal bulb (22). Therefore, mucosal breaks of the low esophagus in EE subjects may contribute more to PG I secretion from the fundus than contributing PG II secretion from other parts of the stomach.
There are several limitations in this study. First, gastric biopsy was not performed in all subjects. Since the subjects were consecutive Korean adults without significant disease who visited for a health check-up, gastric mucosa was biopsied only when there is a suspicious lesion as reflected by color or structural changes during the endoscopic examination. Second, the serum anti-H. pylori IgG was measured using one or other of 2 commercially available immunoassays: the Chorus H. pylori IgG assay and the Vidas H. pylori IgG assay. Nonetheless, it can be assumed that the findings of these 2 tests would not vary, because they exhibit a similar accuracy and a high concurrence rate compared with the Korean H. pylori IgG assay (13). Our study findings can be also supported by a recent study which showed that the serum anti-H. pylori IgG and IgA levels correlate well with the positive findings of the urease test and anti-CagA protein antibody test as well as the degrees of gastritis and H. pylori infiltration (23).
In conclusion, the serum PG assay finding correlated well with the H. pylori-infection related endoscopic findings including NG, GU, DU, CAG, and MG. Increased serum PG concentrations were related to higher risks of NG, GU, and DU, while they were related to a lower risk of EE. Furthermore, a lower PG I /II ratio indicated increased risks of CAG or MG. In H. pylori-seronegative subjects, the serum PG assay findings were correlated with endoscopic findings including EE and H. pylori-negative GU. Taken together, there is a link between UGI endoscopic finding and the serum PG assay, which reflects gastric secreting ability.
Go to :
 XML Download
XML Download