

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The kidney is known as one of the most radiosensitive organs in the abdominal cavity and is the dose-limiting structure for abdominal irradiation (1). Furthermore, over the past decades, total body irradiation (TBI) has emerged as a potential cause of renal impairment after receiving bone marrow transplantation (BMT) (23). Radiation nephropathy is characterized by a slow progressive reduction of renal function, and its clinical symptoms such as hypertension, azotemia, and anemia start after 6 to 12 months after irradiation (4). The radiation-induced kidney damage could progress to chronic renal failure, which was reported to develop in more than 20% of patients receiving TBI (56).
Coenzyme Q10 (CoQ10) is a fat-soluble, vitamin-like substance also called ubiquinone. CoQ10 is found everywhere in the body, and the highest concentrations are found in vital organs with high-energy turnover such as brain, heart, liver, muscle, and kidney (7). CoQ10 is an indispensable compound in the respiratory chain of the inner mitochondrial membrane and acts as essential and powerful antioxidants, scavenging free radicals, and inhibiting lipid peroxidation (8). The antioxidant effect of CoQ10 also enhance the availability of other antioxidants such as vitamin C, vitamin E, and beta-carotene (9).
The anti-oxidative and anti-inflammatory potential of CoQ10 was reported to be beneficial for the nephropathy induced by cisplatin or cyclosporine (1011). However, there has been no previous report of treatment of CoQ10 for radiation nephropathy. The aim of this study was to identify the effects of CoQ10 on radiation nephropathy in rats.
Go to : 
MATERIALS AND METHODS
Animals
A total of 72 adult male Sprague-Dawley rats aged 3–4 months, weighing 300–330 g, were used. The animals were housed in wire cages at a constant temperature of 22°C ± 2°C. They were maintained on a 12-hour dark-light cycle with free access to standard laboratory chow and ultraviolet (UV)-sterilized water. After adaptation period of 1 week, all rats were randomly divided into the 4 groups of 18 animals each: Control, CoQ10, irradiation with 10 Gy (RT) + placebo, or RT + CoQ10.
Irradiation
All rats were anesthetized with an intraperitoneal injection of 100 mg/kg ketamine hydrochloride. The RT + placebo and RT + CoQ10 groups received a single 10 Gy of whole abdominal irradiation using a 6-MV photon beam. The dose of 10 Gy was given based on the previous report that the significant renal function decline occurred 6 months after irradiation with a single dose of 10 Gy and higher in rats (12). Six rats at a time were restrained by the tail in a prone position on a 1 cm-thick acrylic plate and covered by another plate with the same thickness. Radiation was administered simultaneously to the rats at a 3 cm depth through anterior-posterior and posterior-anterior fields using a linear accelerator (Clinac iX, Varian Medical System, Inc., Palo Alto, CA, USA). The radiation dose rate was 1.06 Gy per minute.
Drugs and laboratory test
The control and RT + placebo group received daily intraperitoneal injection of 1 mL of soybean oil for 24 weeks after irradiation. The CoQ10 and RT + CoQ10 group received the same volume of soybean oil containing 10 mg/kg of CoQ10 using the same protocol. Body weights were checked daily. On the last experimental day, the animals were anesthetized by 100 mg/kg ketamine hydrochloride and blood samples of them were taken from trunk vessels for measurement of blood urea nitrogen (BUN) and creatinine levels.
Histopathologic evaluation
All rats were sacrificed by cervical dislocation after blood collection and underwent laparotomy immediately, and right kidneys of each animal were removed. The kidneys were cut in half perpendicular to the long axis at the level of the renal pelvis. Tissue samples were then fixed in 10% buffered formalin for 24 hours and embedded in paraffin wax. The sections were cut at 5 µm and stained with hematoxylin and eosin (H & E), periodic acid Schiff (PAS), and Masson's trichrome stains.
The severity of glomerulosclerosis was assessed using a semiquantitative scoring method that was used widely in previous reports (13). One hundred glomeruli per animal on PAS stained sections (× 400) were selected randomly and graded from 0 to 4: grade 0, normal; grade 1, sclerotic area up to 25% of glomerular tuft; grade 2, sclerotic area 25%–50%; grade 3, sclerotic area 50%–75%; and grade 4, sclerotic area 75%–100%. The glomerulosclerosis index (GSI) was calculated as follows:
The degree of tubulointerstitial fibrosis was also evaluated by a semiquantitative analysis from previous study (14). Twenty fields per section, randomly selected, were assessed on Masson's trichrome stained section (×100) and graded as follows: 0, no fibrosis; 1, fibrosis in up to 10% of field; grade 2, fibrosis in 10%–25% of field; grade 3, fibrosis in 25%–50% of field; grade 4, fibrosis in 50%–100% of field. The tubulointerstitial fibrosis index (TIF) was calculated as follows:
All histopathological evaluation was performed in a blind method.
Statistical analysis
Mean differences between the 4 groups were assessed by one-way analysis of variance followed by Bonferroni's multiple comparison test. Statistical analyses were performed using SPSS, version 22.0 (IBM Corp., Armonk, NY, USA).
Ethics statement
The experimental protocol was reviewed and approved by the Institutional Animal Care and Use Committee at Pusan National University Hospital (No. PNUH 2014-065).
Go to :
RESULTS
Laboratory findings and body weights
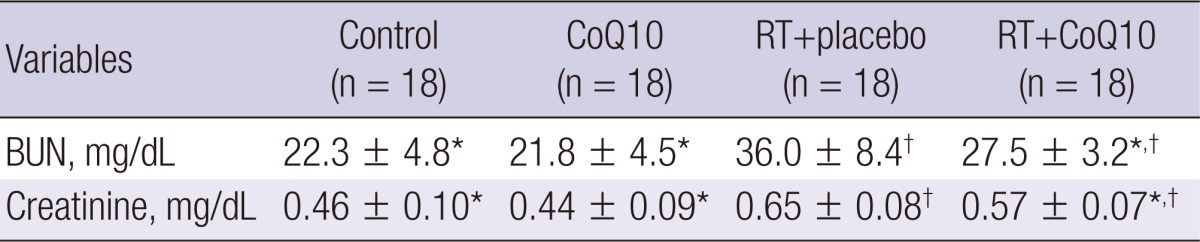
The levels of BUN and creatinine showed significant differences between the 4 groups (P < 0.001). Rats received 10 Gy of whole abdominal irradiation represented significant increases in BUN and creatinine levels, compared to the control group (P < 0.001 for both). CoQ10 administration resulted in a significant reduction of BUN levels in irradiated rats (P < 0.001). The creatinine level was also significantly decreased in the RT + CoQ10 group, compared with RT + placebo group (P = 0.038). The laboratory results were exhibited in Table 1.
The control and CoQ10 groups showed steady weight gain and the average increases of body weight were 194 g and 197 g, respectively. All the irradiated rats developed diarrhea and did not gain weight for about 1 week since irradiation. Mean weight gain of the RT + placebo and RT + CoQ10 group were 164 g and 176 g, respectively. The RT + placebo and RT + CoQ10 groups showed significant differences in mean weight change compared with the control group (P < 0.001 and P = 0.028, respectively). There were no significant differences between the control and CoQ10 groups with laboratory findings and weight changes.
Histopathologic results
The kidney sections of the control and CoQ10 groups showed no obvious glomerular change and the mean GSI of them were measured as 0.08 ± 0.02 and 0.07 ± 0.02, respectively. Glomerular injury such as mesangiolysis and glomerulosclerosis were observed in the 2 RT groups. The mean GSI were 1.61 ± 0.26 in the RT + placebo group and 1.03 ± 0.29 in the RT + CoQ10. CoQ10 treatment significantly decreased the mean GSI of irradiated kidney (P < 0.001). The comparisons of glomerular changes of rat kidneys were displayed in Figs. 1 and 2.
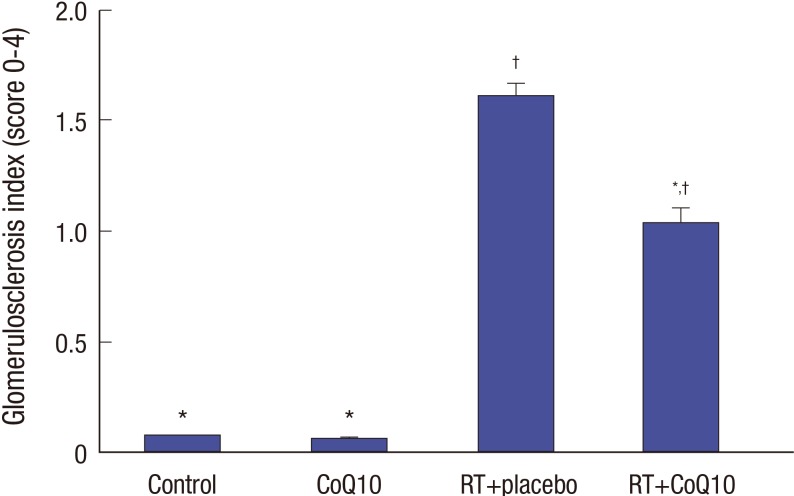 | Fig. 1GSI in rats. Data represent means ± SD (n = 18 per group).
GSI = glomerulosclerosis index, CoQ10 = coenzyme Q10, RT = irradiation with 10 Gy, SD = standard deviation.
*P < 0.05, compared with the RT + placebo group; †P < 0.05, compared with the control group.
|
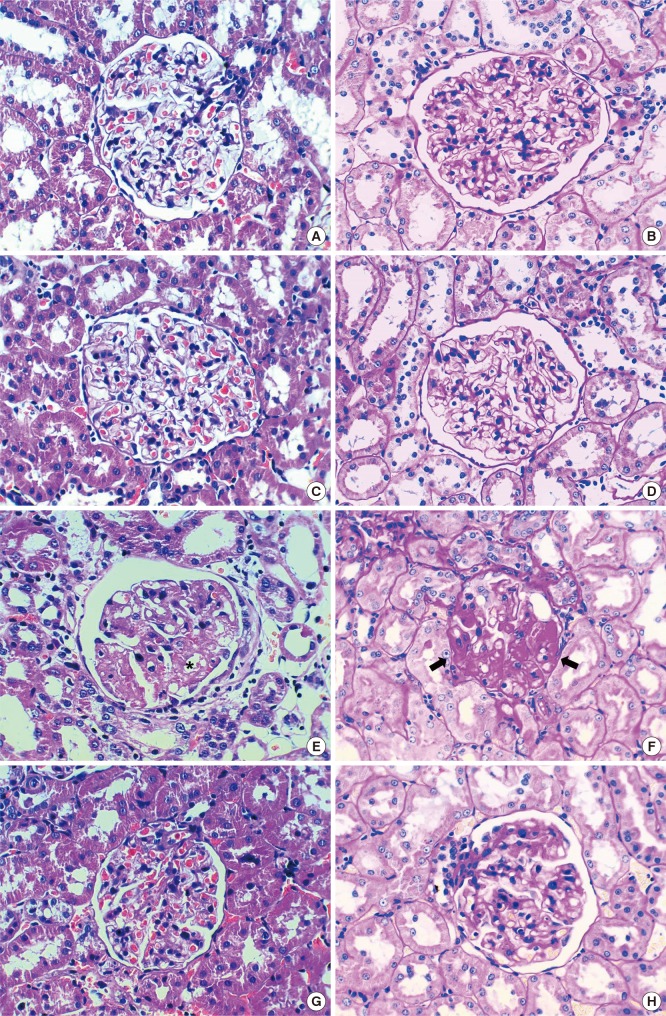 | Fig. 2Histopatholologic features of rat kidneys. (A, B) Control kidney. (C, D) CoQ10 group, exhibiting normal glomeruli. (E, F) RT + placebo group, showing mesangiolysis (asterisk) and glomerulosclerosis (arrow). (G, H) RT + CoQ10 group, representing marked reduction of glomerulosclerosis compared to RT + placebo group (A, C, E, G: H & E; B, D, F, H: PAS, × 400).
CoQ10 = coenzyme Q10, RT = irradiation with 10 Gy, H & E = hematoxylin and eosin, PAS = periodic acid Schiff.
|
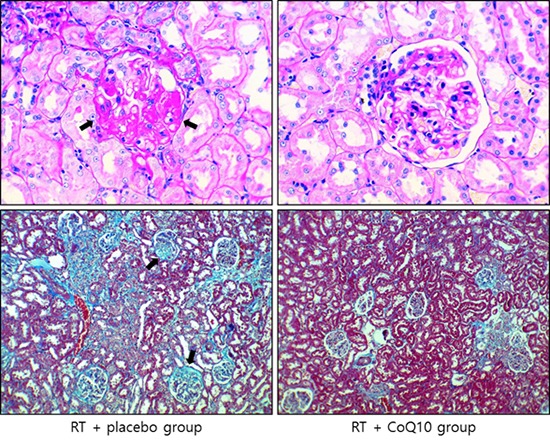
There were no tubulointerstitial fibrosis in the control and CoQ10 groups and their mean TIF were calculated as 0.06 ± 0.04 and 0.05 ± 0.04, respectively. The sections of irradiated rats showed significant tubulointerstitial fibrosis. The mean TIF of RT + placebo and RT + CoQ10 groups were 1.43 ± 0.16 and 0.55 ± 0.17, respectively. The RT + CoQ10 group showed a significantly lower fibrosis grade than RT + placebo group (P < 0.001). The comparisons of fibrotic changes of the kidneys from rats were represented in Figs. 3 and 4.
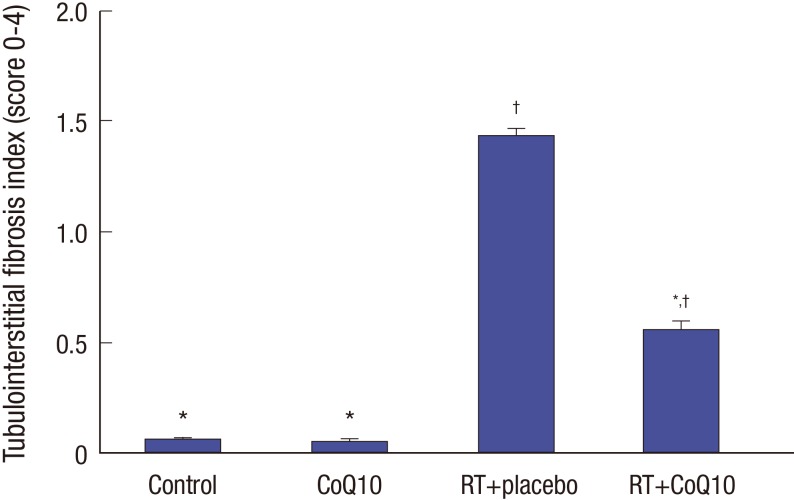 | Fig. 3Tubulointerstitial fibrosis index in rats. Data represent means ± SD (n = 18 per group).
CoQ10 = coenzyme Q10, RT = irradiation with 10 Gy, SD = standard deviation.
*P < 0.05, compared with the RT + placebo group; †P < 0.05, compared with the control group.
|
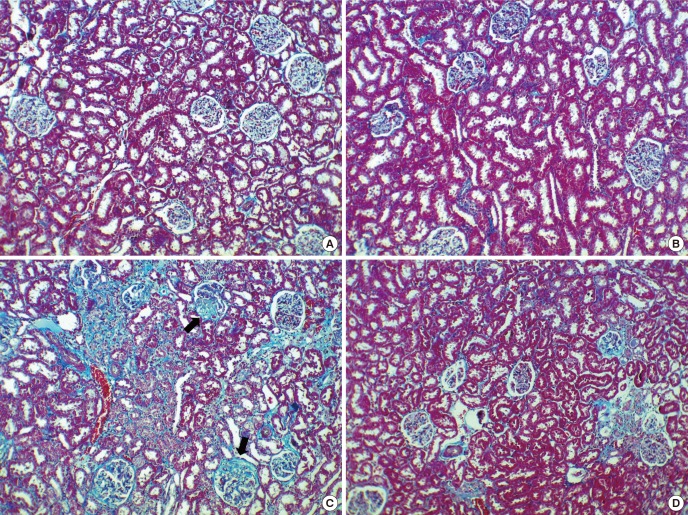 | Fig. 4Histopathologic features of rat kidneys. (A) Control kidney. (B) CoQ10 group, exhibiting no fibrosis. (C) RT + placebo group, showing tubulointerstitial fibrosis and glomerulosclerosis (arrow). (D) RT + CoQ10 group, representing marked alleviation of fibrosis compared to RT + placebo group (Masson's trichrome, × 100).
CoQ10 = coenzyme Q10, RT = irradiation with 10 Gy.
|
Go to :
DISCUSSION
In the present study, we demonstrated that daily supplementation with 10 mg/kg of CoQ10 has beneficial effects in preventing radiation-induced nephropathy in experimental rats. The abdominal irradiation with single dose of 10 Gy increased the BUN and creatinine levels known as serum markers of kidney function, and CoQ10 administration reduced the degrees of elevations of them. CoQ10 also alleviated the pathologic changes in kidney such as glomeulosclerosis and tubulointerstitial fibrosis resulting from whole abdominal irradiation.
The tolerance dose of kidney had been thought to be 20 to 25 Gy in 3 to 5 weeks (1516). In more recent studies, however, the reasonable threshold dose of radiation nephropathy was reported to be lower than 15 Gy with conventional fractionation (5). The radiation nephritis also can occur even after irradiation with a single dose of 5 Gy (17). The improvements in radiation techniques such as intensity-modulated radiation therapy and volumetric arc radiation therapy have resulted in decreasing the radiation dose of kidney and the incidence of radiation nephropathy. Radiation-induced renal damage, nevertheless, cannot be prevented thoroughly because of the low tolerance of kidney. Radiation-induced renal injury is still considered as the principal late toxicity of abdominal irradiation or TBI associated with an inevitable radiation exposure of kidney (123).
Radiation nephropathy is known as typical chronic radiation damage characterized by progressive glomerulosclerosis and tubulointerstitial fibrosis, resulting in ultimate renal failure (418). Several studies showed that the glomerular and tubular fibrotic changes occurred most significantly 24 weeks after irradiation (1419). The chronic progressive nature of radiation-induced renal damage has been reported without any recovery (20). Although there were variable experimental trials to manage the radiation nephropathy, such as angiotensin-converting-enzyme (ACE) inhibitor, amifostine and L-carnitine, only ACE inhibitor was considered to have a clear benefit of mitigating nephropathy without severe adverse effect (212223). ACE inhibitor may slow but not prevent the progression of radiation nephropathy by controlling blood pressure or reducing proteinuria (23).
Radiation damage to cells results from the direct and indirect actions on deoxyribonucleic acid (DNA) molecules. About two-thirds of the damage induced by photon is occurred through the indirect effect. The free radicals, produced by radiolysis of water, indirectly interact with DNA molecules and cause the critical cell damages. Free radicals have unpaired electrons, resulting in highly reactive and short-lived characteristics. These reactive oxygen species play a significant role in the oxidative damage of DNA by radiation therapy (24). The development and progression of radiation nephropathy, especially, was known to be associated chronic oxidative stress (25). The oxidative stress of irradiation can be a cause of the fibrogenesis (26). Radiation-induced lipid peroxidation, that is an important cause of cell damage and destruction, stimulates fibrogenic cytokines, and drives the radiation-induced fibrosis (27). Antioxidants such as CoQ10 have a positive role in preventing the fibrosis by their abilities to scavenge free radicals and inhibit lipid peroxidation (28). In addition, CoQ10 has anti-inflammatory potentials reducing the pro-inflammatory cytokines in inflammatory process (29). These anti-oxidative and anti-inflammatory effects of CoQ10 have been used in treatments of various clinical conditions with oxidative stress and damage such as cardiovascular diseases, neurodegenerative diseases, diabetes, and migraines (30).
Emulsified and oil-based preparations was reported to be helpful to improve the absorption rate of CoQ10 (31). A wide range of doses (60–300 mg/day) of CoQ10 are generally used clinically, and a dose up to 2,400 mg/day was used safely for neurodegenerative disease (30). The administration of CoQ10 was well-tolerated in rats with daily dose of 1,200 mg/kg (32). CoQ10 is known to be safe and well-tolerable, and consumption of high dose CoQ10 over long periods has excellent safety reports (3033). In the present study, 10 mg/kg of CoQ10 was administered to rats based on the previous experimental researches that showed the positive effect of the same dose of CoQ10 on the drug-induced oxidative stress and nephrotoxicity (1011). There were no deaths or CoQ10-related toxicity findings during the experimental period. Supplemental CoQ10 increases plasma CoQ10 concentrations, but may not accumulate in tissues. Furthermore, because the half-life of CoQ10 in plasma is only about 33 hours, steady administration of CoQ10 is needed for chronic oxidative diseases (34).
In conclusion, the administration of CoQ10 improved the radiation-induced nephritis of rats in both laboratory and histopathologic findings. This result indicated that steady supplementation of CoQ10 after abdominal or TBI could ameliorate radiation-induced nephrotoxicity. Further studies will be required to clarify the protective mechanism against radiation-induced nephrotoxicity and confirm the feasibility of CoQ10 supplementation for preventing radiation nephropathy in patients.
Go to :
 XML Download
XML Download