

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
A delayed or advanced bone maturation rate may be associated with various endocrine disorders. Among the most common causes of markedly accelerated bone maturation is exposure to elevated levels of estradiol, testosterone, or adrenal androgen, which occurs in the case of precocious puberty (1) or congenital adrenal hyperplasia (2).
There are also concerns that bone age (BA) advancement may lead to a low final adult height and insulin resistance related to obesity, which causes young adult metabolic disorder (3,4). There is evidence that BA advancement is related to obesity and adrenal androgen. Mildly advanced BA has been observed in precocious adrenarche (5) and, to a lesser extent, in premature thelarche (6).
The prevalence of childhood obesity is currently increasing, and obesity is considered an intriguing link between androgen regulation and BA advancement (7). However, the cause of early-age BA advancement in prepubertal children and the roles played by obesity and adrenal androgens in BA remain unclear and understudied. Therefore, the aim of this study was to investigate the effects of adrenal androgen on BA advancement, independent of obesity, in a cohort of prepubertal children.
MATERIALS AND METHODS
Study subjects
As a part of the Ewha Birth & Growth Cohort Study, we conducted the present investigation to assess the effects of adrenal androgen on BA advancement in prepubertal children. The Ewha Birth & Growth Cohort Study involves a prospective birth cohort, established in 2001–2006. A detailed explanation of this cohort has already been provided in previous studies (8,9). Briefly, we recruited pregnant women at gestational age 24–28 weeks, who sought prenatal care at the Ewha Womans University Mokdong Hospital, Seoul, Korea. The Ewha Womans University Mokdong Hospital is a large general hospital (857 beds; –2,700 outpatients per day on average) located in the western region of central Seoul. A total of 940 women participated in this study, and their children were followed up. In 2011, 664 children reached 7–9 years of age. Of these, 344 subjects were contactable, and 240 participated in a follow-up program in July and August 2011. During that period, the subjects visited the hospital, where we conducted a physical examination and collected blood samples for assessment by a clinician for onset of puberty. Both the children and their parents or guardians granted consent for participation in this study.
In the present investigation, subjects who were entering puberty (Tanner stage ≥ 2, n = 36) at the time of enrollment and those with missing anthropometric or BA data (n = 4) were excluded. Consequently, 200 children with complete data were included in this analysis.
Pubertal and anthropometric assessments
Breast and pubic hair were assessed by a clinician by visual inspection and palpation using the rating scales of Marshall and Tanner (10). Subjects without budding breasts or enlarging testes, classified to be in the prepubertal stage, were included.
The methods used to measure height, weight, and waist circumference were as described previously (9). Body mass index (BMI) was calculated by dividing the subjects' weight in kilograms by the square of their heights in centimeters. We converted height, weight, and BMI into an age- and sex- specific z-score based on the 2007 Korean Children and Adolescents Growth Standard (11). Subjects in the > 85th percentile of age- and sex-specific BMI values based on this standard (8) were defined as overweight. Body fat mass (BFM) was measured using Inbody 230 (GE Healthcare, Madison, WI, USA).
BA assessment
An X-ray scan was recorded for the left hand of all subjects, and BA was determined using the standards of the Greulich-Pyle method (12). All BA measurements were read by a single investigator who was blinded to the identities of the subjects. An index of BA advancement was calculated as the ratio of BA to chronological age (CA) (BA/CA) and classified into tertiles. Sex-stratified analysis was used for association studies.
Blood sampling
We collected fasting venous blood samples for measurement of adrenal androgens such as testosterone (normal range, 3–10 ng/dL), dehydroepiandrosterone (DHEA) (normal range, 20–275 ng/dL), androstenedione (normal range, 8–50 ng/dL), and estradiol (normal range lower than 1.5 ng/dL). Testosterone (KIP1709; DIAsource ImmunoAssays S.A., Nivelles, Belgium), DHEA (IMaa38; IMMUNOTECH, Marseille, France), and androstenedione (KIP0451; DIAsource ImmunoAssays, S.A., Louvain-la-Neuve, Belgium) were measured using commercial kits.
The estradiol level in blood was measured only in female subjects (n = 94) by using a competitive electrochemiluminescence immunoassay method with an Elecsys E170 analyzer (Elecsys Estradiol II; Roche Diagnostics GmbH, Mannheim, Germany).
Statistical analysis
In the descriptive analysis, summary values are presented as means ± standard deviations for numeric variables with normal distribution, medians with interquartile ranges for numeric variables with skewed distribution, and subject numbers and percentages for categorical variables.
Study subjects were classified into 3 groups by BA/CA tertile. We assessed the relationships between BA advancement and anthropometric characteristics and adrenal androgen levels using one way analysis of variance (ANOVA). Considering age and sex as basic demographic variables, we assessed the strength and direction of the relationships among anthropometric characteristics, adrenal androgen and sex hormone levels, and BA advancement using a partial correlation test adjusted for age and sex. Because of their non-normal distribution, adrenal androgen levels were analyzed using the Spearman partial correlation analysis after controlling for sex and age.
Additionally, we used a 2-stage regression analysis to exclude the effects of a correlation between BMI and adrenal androgen in relationship to adrenal androgen, BMI, and BA advancement as below.
Second stage regression:
where α represents the intercept, β the coefficient, and ε the residuals. BA/CA residuals provide a measure of BA/CA ratios that were not correlated with age, sex, or BMI. Before the regression analysis, androstenedione and testosterone hormone levels were log-transformed to satisfy statistical normal distribution. Because log-transformed DHEA values do not satisfy the assumption of normality, we presented only the results for androstenedione and testosterone in Fig. 1.
 | Fig. 1Association between BA/CA and adrenal androgen levels.
Residual obtained from the regression model using BA/CA as the dependent variable and BMI, age, and sex as independent variables. These residual values were then used as dependent variables with log-transformed hormone concentrations as the independent variables in the regression model. The regression line indicates the linear association between (A) log-transformed androstenedione or (B) log-transformed testosterone levels and the BA/CA ratio residual.
BA = bone age, CA = chronological age, BA/CA = bone age to chronologic age ratio, BMI = body mass index.
|
Statistical analysis was conducted using SAS version 9.3 (SAS Institutes, Cary, NC, USA). All analyses were 2-tailed, and a P value of < 0.05 was considered statistically significant.
RESULTS
The baseline data, adiposity, and hormonal characteristics of the children are presented in Table 1. The study group comprised 200 prepubertal children (106 boys and 94 girls), of whom 26 (13%) were found to be overweight. The subjects were divided into 3 groups according to the BA/CA tertile. The mean BA/CA ratio in the third group (1.18 ± 0.10) was approximately 1.4-fold higher than that in the first group (0.85 ± 0.05). The median levels of serum testosterone, DHEA, and androstenedione were within the normal prepubertal ranges. The mean estradiol level, measured only in girls, was 7.45 (range, 4.90–11.36) ng/mL (Table 1). When we evaluated height, weight, the level of adrenal androgens by sex, the results showed no significant differences with height and the level of adrenal androgens except weight. When we analyzed the BA/CA tertile groups using one-way ANOVA, height, and weight z-scores showed significant differences (P < 0.001) among the 3 groups, but the obesity indicators did not. The proportion of overweight subjects differed marginally but significantly (P = 0.007) among the groups and was higher in the third group than the first group (P
Trend = 0.03). Correlation analyses showed that BMI (r = 0.16; P = 0.02) and BFM (r = 0.16; P = 0.02) were positively associated with BA/CA after adjusting for age and sex. The levels of all hormones evaluated, except estradiol, showed significant differences (P < 0.001) among the 3 BA/CA tertile groups, and correlation analysis for adrenal androgen levels adjusted for age and sex showed a positive correlation between BA/CA and the levels of testosterone (r = 0.26; P < 0.001), DHEA (r = 0.21; P < 0.001), and androstenedione (r = 0.20; P < 0.001) (Table 2).
Table 1
Basic characteristics of the study subjects
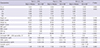
SD = standard deviation, IQR = interquartile range, BA = bone age, CA = chronological age, BA/CA = bone age to chronologic age ratio, BMI = body mass index, BFM = body fat mass, WC = waist circumference, DHEA = dehydroepiandrosterone, HOMA = homeostasis model assessment.
*Result presents as number of subjects with percent; †Estradiol concentration was measured only in female subjects (n = 94).
![]()
Table 2
Relationships between anthropometric data and adrenal hormone levels in the BA/CA tertiles
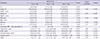
BA = bone age, CA = chronological age, BA/CA = bone age to chronologic age ratio, BMI = body mass index, BFM = body fat mass, WC = waist circumference, DHEA = dehydroepiandrosterone, HOMA = homeostasis model assessment, ANOVA = analysis of variance.
*P value obtained using one-way ANOVA for variables with normal distribution or the Kruskal-Wallis test for variables with non-normal distribution; †P value for partial correlation adjusted for age and sex obtained using Pearson correlation for variables with normal distribution or Spearman correlation for variables with non-normal distribution; ‡Estradiol concentration was measured only in female subjects (n = 94).
![]()
Multiple regression analysis was conducted using a stepwise regression model to predict the relationship between adrenal androgen levels and BA/CA adjusted for sex, age, and BMI. This model accounted for 5.8% of the variance in the BA/CA ratio in our study population. BA/CA showed a positive correlation with androstenedione (β = 0.04; R
2 = 3.7%) and testosterone (β = 0.05, R
2 = 4.7%) levels (Fig. 1) independent of BMI.
DISCUSSION
The main finding of our study was that BA advancement and adrenal androgen levels are positively associated independent of obesity. It is widely assumed that obesity is strongly associated with BA advancement in children with premature adrenarche (4). Our results showing that the BA/CA ratio was correlated with BMI and BFM agree with those of previous studies that showed a correlation between the degree of obesity and advancement of BA (13-16). The degree of obesity, as expressed using BMI or BFM, and increased levels of estrogen and DHEA have been shown to be associated with advanced BA (15,16). Several investigations found overweight children to have advanced BA that significantly exceeded their CA (17), and in overweight prepubertal children, puberty seems to be initiated and progress at an earlier age than it does in prepubertal children with normal body weight (18). Adrenal androgen levels are higher in children with obesity than in those with normal body weights, and these increased levels are believed to be responsible for the accelerated prepubertal growth of the former (16), although the mechanism is not clear. The present study showed a more accurate association between the BA/CA ratio and androstenedione and testosterone levels. The supposed mechanism is as follows. It has been generally believed that an important part of the effect of androgens or their metabolites on the skeleton is exerted via a direct stimulation of the androgen receptor (AR), estrogen receptor (ER) α, ER β. AR expression has been observed at different ages and no major sex difference in human growth plate chondrocytes. Therefore, androgen could have important role at bone maturation of prepubertal children on both sexes (19).
The ossification of the epiphyseal plate when final adult height is reached is a complex process involving parathyroid-related peptides, matrix metalloproteinases, and vascular endothelial growth factors. Estrogens, androgens, and insulin-like growth factor (IGF)-1 influence the activity of these factors and the progression of skeletal maturation (20). We analyzed IGF-Ι, insulin, and other metabolic components but found no meaningful relationships between them and the advancement of BA in our subjects (Table 2).
Both BA and weight have been shown to be significant covariates of DHEA levels (17), and DHEA may be a marker of estradiol production (21). The higher sex hormone levels in prepubertal overweight children could stimulate linear growth, skeletal age, and hypothalamic maturity, ultimately leading to earlier onset of puberty. It remains unclear which hormones play the most significant roles. Estrogen is widely thought to promote BA advancement, but in the present study, no differences in estradiol levels were found among the 3 tertile groups of female subjects.
Our cohort study consisted of general children and we did not limit the target population for prepubertal overweight children as in previous study. It could be the one reason to explain the difference between research results from estradiol or insulin resistance influence on BA advancement.
However, a positive correlation was found between the DHEA levels and the BA/CA ratio. There are concerns that children with advanced BA who are taller than those in the same age bracket during prepubescence could ultimately have a lower final height than their predicted height in adulthood (22). In terms of the implications of our study findings, the finding that advanced BA is associated with elevated adrenal androgen levels independent of obesity indicates that attention must be paid to adrenal androgen levels even among non-obese prepubertal children.
Our study has several strengths. First, we conducted pubertal examinations for all subjects, who comprised Asian children from the general population, and excluded those with signs of precocious puberty. Studies of BA advancement in prepubertal Asian children are rare and have significance, because BA advancement and adrenarche in prepubertal children show racial differences (7,13,17). On the other hand, the limitations of this study are the small sample size and the fact that our results do not reveal the direct cause of BA advancement but only show its association with various factors. Larger studies are needed in the future to investigate both the clinical features and hormone levels of prepubertal children to better understand the factors involved in BA advancement and their mechanisms of action. Owing to limitation of the amount of research funding, we could not measure free testosterone and sex hormone binding globulin (SHBG). We just chose and measured the 4 representative adrenal androgens. DHEA-sulfate (S) is the metabolites of the DHEA and in the blood, most DHEA is found as DHEA-S. Whereas DHEA levels naturally reach their peak in the early morning hours, DHEA-S levels show no diurnal variation and measurement of DHEA-S is preferable to DHEA. But, both measurements of DHEA-S/DHEA are useful to detect adrenal activity and we chose DHEA, testosterone, androstenedione as andrenal androgen and collected the blood samples early morning. Further, systematic longitudinal studies in children with premature adrenarche are warranted to address the apparent links among early-onset androgen excess, insulin resistance and metabolic risk, and advanced BA.
In conclusion, our study demonstrated that the levels of adrenal androgens (testosterone and androstenedione) are associated with BA advancement independent of BMI.
 XML Download
XML Download