

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Inflammatory bowel disease (IBD) is a chronic relapsing-remitting condition whose 2 major subtypes are Crohn's disease (CD) and ulcerative colitis (UC). CD has the potential to affect any part of the gastrointestinal tract, while UC is typically confined to the colonic mucosa. IBD is a systemic disease with multiple extraintestinal symptoms and complications, including osteopenia and osteoporosis. In adults, factors contributing to this bone loss have been reviewed well and include persistent production of proinflammatory cytokines, low body weight, low lean mass, minimal physical activity, extended treatment with systemic steroids, micronutrient deficiencies, and variations in interleukin (IL)-6 or IL-ra gene (12). By contrast, data on low bone mineral density (BMD) in pediatric IBD are still limited. While the exact pathophysiology of impaired bone health in this population remains to be determined, vitamin D has garnered some interest in recent years (3).
Vitamin D is a well-known regulator of calcium homeostasis. After dietary intake or cutaneous synthesis, it is hydroxylated in the liver to form 25-hydroxyvitamin D (25[OH]D), the functional marker of vitamin D status in clinical practice. Further hydroxylation produces 1-25-dihydroxyvitamin D, which assists in regulating osteoblast differentiation, production of bone matrix components, gastrointestinal absorption of calcium, and reabsorption of calcium and phosphate in the kidneys (4). Young patients with IBD are predisposed to vitamin D deficiency due to limited sunlight exposure from bed rest, reduced absorption of vitamin D consequent to mucosal inflammation or bowel resection, increased uptake by inflammatory cells in the affected sites, and inadequate dietary intake from restricted diet or intentional avoidance (57). However, previous studies have reported vastly different prevalence rates of vitamin D deficiency in pediatric IBD patients, ranging from 19% to 62% (89).
To our knowledge, 6 studies have investigated the potential relationship between vitamin D deficiency and low BMD in children with IBD (101112131415). However, these studies have minimal to no inclusion of non-Caucasian subjects and no study has included a local control group for the comparison of BMD. Moreover, there is currently no published study that has examined the relationship between vitamin D and BMD among children with IBD in Asia, despite the dramatic rise in the incidence of pediatric IBD in this region in recent years (161718).
Therefore, our study aimed to evaluate differences in serum 25(OH)D and BMD z-scores in Korean children with CD, UC, and those with abdominal pain-related functional gastrointestinal disorder (AP-FGID) as the control group. We also aimed to examine the correlation between 25(OH)D and BMD z-score in these children, and to identify factors that impact on BMD z-score or 25(OH)D.
MATERIALS AND METHODS
Study subjects
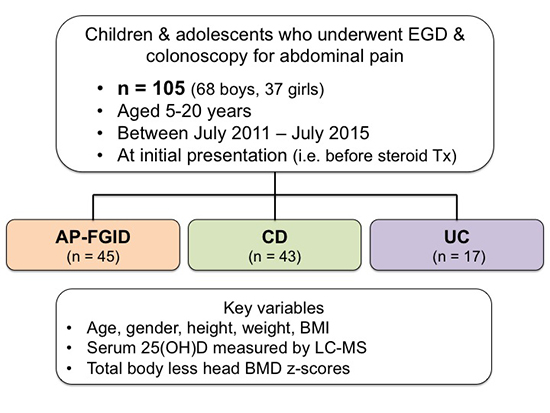
Electronic medical record database at Seoul National University Bundang Hospital (SNUBH) was reviewed for this retrospective study. A total of 105 patients, aged 5 to 20 years, who underwent upper gastrointestinal endoscopy and colonoscopy for abdominal pain at SNUBH between July 2011 and July 2015 were included. Subjects were divided according to their diagnosis: AP-FGID (n = 45), CD (n = 43), and UC (n = 17). All children underwent relevant investigations including laboratory tests and BMD measurement at initial presentation and prior to commencing any steroid treatment.
Exclusion criteria were diagnosis of IBD-unclassified, incomplete data, history of vitamin D supplementation, steroid therapy or orthopedic surgery, and concurrent diagnosis of any other condition known to cause malabsorption syndrome.
Anthropometric data
Anthropometric measurements of all patients were collected from the hospital's medical records. Height was measured in centimetres to 1 decimal place using a standard stadiometer and weight was measured kilograms to 1 decimal place using a digital scale. Body mass index (BMI) was expressed as kg/m2.
Laboratory tests
Laboratory tests included in this study were serum hemoglobin, hematocrit, platelet count, white blood cell (WBC), absolute neutrophil count (ANC), calcium, phosphorus, alkaline phosphatase (ALP), total serum protein, albumin, erythrocyte sedimentation rate (ESR), high-sensitivity C-reactive protein (hs-CRP), and 25(OH)D. Serum 25(OH)D concentration was measured in nanograms per millilitre using liquid chromatography-mass spectrometry (LC-MS) (LC-MS/MS; Waters, Milford, MA, USA).
BMD measurement
BMD of the whole body was measured using dual-energy X-ray absorptiometry (DXA; software enCORE 2011 version 13.60; Lunar Prodigy, GE Medical systems, Madision, WI, USA). The scan was performed on all children at initial presentation and within 3 days of laboratory tests. Total BMD and total body less head (TBLH) BMD were expressed as z-scores using sex-specific and age-matched reference data provided by the manufacturer.
Statistical analysis
SPSS 20.0 software program (IBM Corp., Armonk, NY, USA) was used to perform statistical analyses. Data were expressed as mean ± standard deviation. Parametric analysis was performed using one-way analysis of variance (ANOVA). Chi-square test was applied to assess the difference in sex among all subjects. Pearson's correlation was used to determine the correlation between serum 25(OH)D and TBLH BMD z-score in all patients, while Spearman's correlation was used to determine the correlation within each study group. Multiple regression analysis (analysis of covariance; ANCOVA) was used to evaluate various factors affecting TBLH BMD z-score or serum 25(OH)D concentration. A P value less than 0.05 was regarded as statistically significant.
RESULTS
Patient characteristics
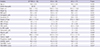
Clinical and biochemical profiles of pediatric patients with AP-FGID, CD, and UC are listed in Table 1. Among the 3 study groups, there were significant differences in hemoglobin, hematocrit, platelet count, WBC, ANC, ESR, hs-CRP, albumin, and calcium.
Table 1
Clinical and biochemical profiles of children with AP-FGID, CD and UC
Data presented as mean ± standard deviation.
AP-FGID = abdominal pain-related functional gastrointestinal disorder, BMI = body mass index, CD = Crohn's disease, UC = ulcerative colitis, WBC = white blood cell, ANC = absolute neutrophil count, ESR = erythrocyte sedimentation rate, hs-CRP = high-sensitivity C-reactive protein, ALP = alkaline phosphatase, 25(OH)D = 25-hydroxyvitamin D, BMD = bone mineral density, TBLH = total body less head.
*P value less than 0.05 is regarded as statistically significant.
No significance was observed for serum 25(OH)D concentration among the 3 groups (16.5 ± 5.3 ng/mL in AP-FGID; 16.3 ± 9.3 ng/mL in CD; 19.9 ± 7.2 ng/mL in UC; P = 0.224), despite a significant difference between the CD group and the UC group (P = 0.028). Among the 3 groups, TBLH BMD z-score was found to be significantly different (−0.1 ± 1.1 in AP-FGID; −0.5 ± 0.8 in CD; 0.1 ± 0.8 in UC; P = 0.037).
Correlation between serum 25(OH)D and BMD
Correlation between serum 25(OH)D concentration and TBLH BMD z-score is shown in Fig. 1. Serum 25(OH)D was positively correlated with TBLH BMD z-score when all subjects were included in the analysis (rs = 0.231; P = 0.021). However, no significant correlation was observed within each study group (r = 0.151; P = 0.323 in AP-FGID; r = 0.249; P = 0.132 in CD; r = −0.032; P = 0.906 in UC).
Fig. 1
Correlation between serum 25(OH)D and TBLH BMD z-score in the 3 study groups. There was no significant correlation in the AP-FGID group (r = 0.151; P = 0.323), CD group (r = 0.249; P = 0.132), or the UC group (r = −0.032, P = 0.906).
25(OH)D = 25-hydroxyvitamin D, TBLH = total body less head, BMD = bone mineral density, AP-FGID = abdominal pain-related functional gastrointestinal disorder, CD = Crohn's disease, UC = ulcerative colitis.

Factors affecting TBLH BMD z-score in all subjects
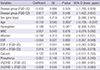
When multiple regression analysis of TBLH BMD z-score was performed, sex (P = 0.018), age (P = 0.005), and hemoglobin (P = 0.041) were found to be significant factors (Table 2). TBLH BMD z-score was lower in girls and older children, with a BMD z-score decrement of 0.118 for one-year increase in age. In addition, hemoglobin was positively correlated with TBLH BMD z-score in children with CD (r = 0.377; P = 0.018), but not in the other 2 study groups.
Table 2
Multiple regression analysis of TBLH BMD z-score according to disease group, patient demographics, and laboratory results
ANCOVA was used for statistical analysis; × symbol denotes interaction between the variables.
TBLH = total body less head, BMD = bone mineral density, SE = standard error, 95% CI = 95% confidence interval, FGID = abdominal pain-related functional gastrointestinal disease, UC = ulcerative colitis, CD = Crohn's disease, FGID-UC = UC in comparison to FGID, FGID-CD = CD in comparison to FGID, girls-boys = boys in comparison to girls, WBC = white blood cell, ESR = erythrocyte sedimentation rate, 25(OH)D = 25-hydroxyvitamin D, ANCOVA = analysis of covariance.
*P value less than 0.05 is regarded as statistically significant.
Factors affecting serum 25(OH)D in all subjects
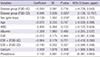
Multiple regression analysis of serum 25(OH)D revealed that sex (P = 0.018), CD group with reference to AP-FGID (P = 0.020), and serum phosphorus (P = 0.018) were significant factors in these children (Table 3). Lower serum 25(OH)D levels were associated with female sex, CD group status, and lower serum phosphorus levels. Moreover, serum phosphorus was positively correlated with 25(OH)D in children with CD (r = 0.386; P = 0.012).
Table 3
Multiple regression analysis of serum 25(OH)D according to disease group, patient demographics, and laboratory results
ANCOVA was used for statistical analysis; × symbol denotes interaction between the variables.
25(OH)D = 25-hydroxyvitamin D, SE = standard error, 95% CI = 95% confidence interval, FGID = abdominal pain-related functional gastrointestinal disease, UC = ulcerative colitis, CD = Crohn's disease, FGID-UC = UC in comparison to FGID, FGID-CD = CD in comparison to FGID, girls-boys = boys in comparison to girls, ESR = erythrocyte sedimentation rate, ANCOVA = analysis of covariance.
*P value less than 0.05 is regarded as statistically significant.
DISCUSSION
On the background of the rising incidence of pediatric IBD in Asia, this study is the first to formally investigate vitamin D status and BMD in Korean children with IBD. Our results demonstrated that in this cohort of children with CD, UC, AP-FGID, and TBLH BMD z-scores were significantly different and the lowest in children with CD. According to our study, the important determinants of TBLH BMD z-score in these children are sex, age, and hemoglobin concentration, rather than vitamin D status. Therefore, it seems that vitamin D may not be a useful predictor of bone loss in children with IBD as it is for their adult counterparts.
Our study revealed similar levels of serum 25(OH)D among children with CD, UC, and AP-FGID. This is possibly due to the AP-FGID group's low 25(OH)D levels, which were similar to those of the CD group. AP-FGID is a functional gastrointestinal condition without any evidence of organic disease, but our results indicate that patients with severe symptoms may also develop nutrient deficiencies. Moreover, our results may reflect the fact that Korean children and adolescents in general are prone to vitamin D insufficiency from their largely sedentary indoor lifestyle and the consequent lack of exposure to sunlight (19).
TBLH BMD, along with lumbar spine BMD, was recently recommended as the preferred skeletal site for DXA evaluation of pediatric subjects (20). Excluding the cranium minimizes contribution of the child's proportionally large head that may mask potential BMD deficits at other sites (21). In our study, TBLH BMD z-scores were significantly different among the 3 groups, with BMD considerably lower in children with CD compared to those with UC or AP-FGID. Therefore, our study supports previous studies on children that have reported higher prevalence of low BMD in CD compared to UC (10132223), and higher prevalence of growth failure and vertebral fractures in CD (242526). Higher risk of poor bone health in CD patients can be explained by small intestine involvement causing malabsorption or protein-losing enteropathy, and the higher systemic inflammatory load that confers both direct effects on osteoblast activity and indirect effects such as more frequent use of steroids (25).
A major finding of our study was that sex, age, and hemoglobin concentration significantly influenced TBLH BMD z-scores in this cohort of children. Girls were found to have lower TBLH BMD z-scores, in line with the recent study by Schmidt et al. (14) who found TBLH BMD z-scores to be lower in girls at both baseline and 2 years later. Other studies that have contradicted this observation were cross-sectional studies with CD patients only (1125), or included femoral neck BMD in their analysis (10) although this region has been deemed inappropriate for DXA scanning in children (27). It is well known that boys have greater bone mass after the onset of puberty, but the comparatively lower BMD in girls across all ages may also be explained by lower body weight, lower lean mass, and lower levels of physical activity.
Older age was associated with lower BMD z-score in these children, echoing the results reported by Herzog et al. (28) who found that among children with CD in remission, those older were more likely to have low BMD. However, disease duration would have been responsible to an extent in this study, whereas all of our subjects were evaluated at initial presentation. Our results could therefore be related to higher disease severity in children with earlier onset of symptoms, or characteristics of older children and adolescents that predispose them to low BMD, such as sedentary lifestyle or reduced compliance to treatment.
To our knowledge, this is the first study to report hemoglobin as a determinant of BMD in children with IBD. We observed a positive correlation between hemoglobin and BMD in children with CD, which may be reflective of poor overall nutritional status and lack of hematopoietic nutrients such as iron, vitamin B12, and folate. Alternatively, lower hemoglobin may be related to higher disease activity, since low hematocrit is one of the components of the Pediatric Crohn's Disease Activity Index. It would be interesting to see if future studies replicate this novel finding and aid in characterising more predictive markers of diminished bone mass in pediatric IBD.
In accordance with other published studies (101112131415), we found no significant correlation between serum 25(OH)D and BMD z-score. Although the lack of correlation is somewhat counterintuitive, this was observed in both UC and CD groups with the use of different vitamin D assays and BMD measurements sites, and after taking into account the disease activity (11). By contrast, majority of adult studies have demonstrated a significant correlation between the 2 parameters (29303132). Thus, it seems that the pathophysiology of bone loss in pediatric IBD may be fundamentally different or more complex, with the contribution of vitamin D status more limited than previously thought.
It is currently unclear whether the prevalence of poor vitamin D status is significantly different between the 2 IBD subtypes, as studies continue to show divergent results. In our study, CD disease status, but not UC, was found to affect 25(OH)D when compared to the AP-FGID group as the reference point. Therefore, our results support the hypothesis that children with CD are more at risk of subnormal vitamin D status. Researchers have so far postulated that this could be due to poor digestion of lipid-soluble compounds and less absorption of vitamin D via the jejunum and terminal ileum (33). None of our IBD subjects had undergone bowel resection, but this would also be more common among patients with CD and cause malabsorption of a wide range of nutrients.
Our study is limited by a retrospective, single-center study design. Extracting data from the hospital electronic medical records yielded a disease-control group, but we believe that AP-FGID is a good substitute due to its lack of organic pathology. Our study may have been improved by inclusion of disease activity index to account for the variability in disease severity, although currently there is no unified index for both UC and CD. A possible clustering of 25(OH)D sampling by season may have affected our results. However, seasonal variance in vitamin D levels may not be as prominent in children with IBD, as those with severe disease are limited to bed rest and indoor confinement regardless of the season.
Our study has several strengths that deserve a mention. It is the first study to formally investigate the correlation between vitamin D and BMD in Asian children with IBD, since the few studies that have been published thus far have almost exclusively focused on Caucasian children. Our subjects were also evaluated at diagnosis, minimizing the possible effects of disease duration and pharmacological treatment on bone mass. Moreover, serum 25(OH)D was measured using LC-MS/MS, which is widely considered as one of the most accurate assays for vitamin D (34). Another aspect of our study that merits attention is the inclusion of a local control group to compare BMD z-scores. Other studies have used densitometer reference data as a surrogate control group, which can yield misleading results. In their 2004 study, Gupta et al. (35) concluded that normal population values derived from commercial densitometers were not appropriate for the local patient population studied. By comparing BMD z-scores of the disease groups to those of a control group of the same ethnicity and locality, our study is likely to have been more accurate in detecting true discrepancies in BMD.
The present study adds significant findings to the scarce literature on the potential relationship between vitamin D status and bone loss in pediatric IBD. Limited bone mass accrual in pediatric IBD poses a real risk of reducing the child's peak bone mass, the strongest predictor of future risk of osteoporosis in adulthood (36). Our results indicate that vitamin D status may not be a significant determinant of BMD in pediatric IBD patients as it is for adult IBD patients. However, given the chronic and variable course of IBD, more longitudinal studies are needed to evaluate vitamin D status and BMD at different phases of the disease (37).
In conclusion, our study demonstrated that TBLH BMD z-scores were significantly different among children with AP-FGID, CD, and UC, despite similar serum 25(OH)D levels. Our results suggest that significant risk factors for low BMD in these children are female sex, older age, and low hemoglobin levels, while vitamin D status may not be as important. The link between vitamin D and bone loss in pediatric IBD seems more complex than previously thought and more studies on predictors of bone loss in these children are warranted for their long-term skeletal health.
 XML Download
XML Download