

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Long-term oral anticoagulant therapy is frequently and increasingly prescribed for preventing thromboembolism in patients who are at risk because of atrial fibrillation or mechanical heart valves or patients with prior thromboembolic events who are at risk of recurrent venous thromboembolism (VTE) (1).
Despite the large number of patients who require temporary interruption of anticoagulants for elective surgical or invasive procedures, managing these patients has been poorly investigated (2). Although there is a lack of reliable estimates of the incidence of thromboembolic events associated with warfarin interruption (2), such events can have devastating clinical consequences: thrombosis of a mechanical heart valve is fatal in 15% of patients (3), and embolic stroke results in a major neurologic deficit or death in 70% of patients (4).
During perioperative withdrawal of oral anticoagulants, one strategy to maintain a degree of functional anticoagulation is to administer short-acting parenteral anticoagulants such as heparin while oral anticoagulant therapy is sub-therapeutic, a strategy known as bridging therapy (5). However, bridging anticoagulation can expose patients to serious bleeding complications (6). Low-molecular-weight heparin (LMWH) can be administered subcutaneously, in a fixed-weight-based dose without the need for laboratory monitoring, thereby obviating the need for hospitalization to administer anticoagulants (7).
Although the safety and efficacy of LMWH for the prophylaxis and treatment of deep vein thrombosis and treatment of acute coronary syndromes have been well described in clinical trial settings, there is little evidence to support its efficacy and safety as a bridging anticoagulant (89). This study was designed to evaluate the efficacy and safety of perioperative anticoagulation with enoxaparin.
MATERIALS AND METHODS
Study design
This was a retrospective, single-center study that evaluated the efficacy and safety of therapeutic-dose enoxaparin combined with which bridging therapy was planned for invasive procedures or surgeries in patients on long-term warfarin. The study population had been admitted to Soonchunhyang University Hospital in Korea between August 2009 and July 2011. The primary purpose of this study was to investigate the incidence of thromboembolic or bleeding events during the perioperative period in patients who had received bridging anticoagulation with enoxaparin.
Study sample
The patients were aged 18 years and over and were receiving warfarin therapy for atrial fibrillation, VTE, or mechanical heart valves; they had been referred to the Anticoagulation Clinic to use proper therapeutic-dose LMWH as a perioperative bridging therapy before undergoing major or minor surgery or invasive procedures that necessitated temporary interruption of warfarin. Patients were excluded if they had had ischemic stroke 3 months before enrollment, any previous hemorrhagic stroke, active bleeding, recent gastrointestinal bleeding, a bleeding disorder, thrombocytopenia, or pregnancy.
Major surgeries or procedures included intraabdominal surgery, intrathoracic surgery, major orthopedic surgery, peripheral arterial revascularization (e.g., abdominal aortic aneurysm repair, vascular bypass), urologic surgery (e.g., prostatectomy, bladder tumor resection), permanent pacemaker or internal defibrillator insertion, a major procedure (e.g., colonic polyp resection, biopsy of kidney or prostate), and any other surgery or procedure lasting ≥ 1 hour (10).
Minor surgeries or procedures included gastrointestinal endoscopy, cardiac catheterization, dental surgery or other dental procedure, dermatologic surgery or other dermatologic procedure, cataract removal or other ophthalmologic procedure, and any other surgery or procedure lasting < 1 hour (Table 1).
Table 1
Baseline chracteristics of patients receiving bridging anticoagulation

Values are presented as number (%).
VTE = venous thromboembolism, IQR = interquartile range, CHF = congestive heart failure, CVA = cerebrovascular accident, TIA = transient ischemic attack, GFR = glomerular filtration rate.
*The CHA2DS2-VASc score is a measure of the risk of stroke in which congestive heart failure, hypertension, an age of 65 to 74, diabetes mellitus, vascular disease (e.g., prior myocardiac infarction, aortic plaque, or peripheral arterial disease), female gender are each assigned 1 point and previous stroke, transient ischemic attack, thromboembolism or age older than 75 is assigned 2 points; the score is calculated by summing all the points for a given patient.
![]()
Perioperative management of anticoagulation
Warfarin was discontinued 5 days before surgery. Three days before the procedure, enoxaparin was administered twice daily by subcutaneous injection at a dose of 1 mg per kg; the last preoperative dose was administered on the morning before the procedure. On the day before or on the morning of the procedure, the international normalized ratio (INR) was measured to ensure that it was normalized (≤ 1.3).
Subcutaneous enoxaparin was reinitiated at a dose of 1 mg per kg twice daily 48–72 hours. after a major surgery or procedure and 12–24 hours. After a minor surgery or procedure provided that adequate hemostasis had been achieved; the first postoperative dose of enoxaparin could have been delayed if the surgeon assessed that the hemostasis was inadequate.
Warfarin was restarted on the day enoxaparin was started or on the following day. The warfarin dose was double the patient's usual daily dose for the first 2 days and then the same as the usual daily dose. Treatment with enoxaparin was continued until the INR was within the target range for 2 consecutive days. The same perioperative protocol was applied to patients with mechanical valve.
Outcomes
The primary efficacy outcome was the incidence of acute thromboembolic events within 30 days after the procedure (e.g., ischemic stroke, transient ischemic attack, systemic embolism, or symptomatic VTE). The secondary efficacy outcome was the rate of all-cause mortality.
The primary safety outcome was the incidence of major bleeding within 30 days after the procedure, and major bleeding was defined as overt bleeding leading to a ≥ 2 g/dL drop in hemoglobin, transfusion of ≥ 2 units of packed red blood cells (RBCs), need for re-operation or invasive intervention, any bleeding at a critical anatomic site (e.g., intracranial, retroperitoneal, intraocular, or pericardial), or fatal bleeding.
RESULTS
Patient and procedure characteristics
In total, 49 patients (25 men, 24 women; mean age, 63 years; range, 19–84 years) were included in the study between August 2009 and July 2011 (Table 1). Approximately two-thirds of the patients had received warfarin therapy for prior VTE and one-fifth for atrial fibrillation. Twenty-nine patients (59.2%) underwent major surgery and 20 patients (40.8%) minor surgery. Twenty patients (40.8%) received warfarin therapy less than or equal to 90 days before the procedure, and 29 patients (59.2%) received it for more than 90 days. The mean duration on warfarin was 122 days. Among 34 patients with VTE, 19 patients (55.9%) had experienced warfarin for more than 90 days before procedure, including 8 patients (23.5%) with active cancer. There were various comorbidities, including active malignancy in 16 patients (32.7%), congestive heart failure in 3 patients (6.1%), cerebrovascular accident or transient ischemic attack in 3 patients (6.1%), ischemic heart disease in 4 patients (8.2%), and renal insufficiency in 10 patients (20.4%).
Adherence to bridging anticoagulation protocol
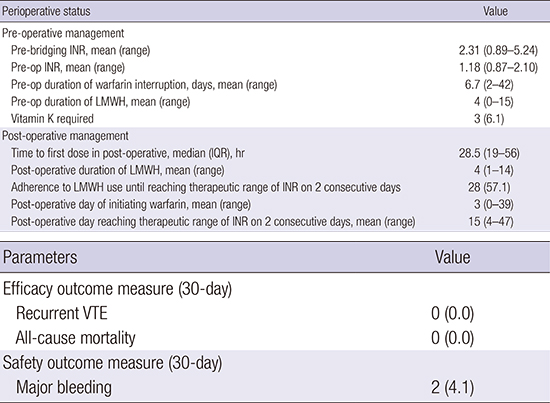
The mean INR before warfarin was withheld was 2.31 (range, 0.89–5.24; Table 2). The mean preoperative durations of warfarin interruption and enoxaparin administration were 6.7 days (range, 2–42), and 4 days (range, 0–15), respectively. Three patients (6.1%) received preoperative vitamin K to normalize the INR.
Table 2
Perioperative status and adherence to bridging protocol (n = 49)

Values are presented as number (%).
INR = international normalized ratio, LMWH = low-molecular-weight heparin, IQR = interquartile range.
![]()
The enoxaparin was restarted a mean 39 hours (range, 11–150) after a surgery or procedure, and the mean postoperative enoxaparin duration was 4 days (range, 1–14). In only 28 patients (57.1%) was enoxaparin administered until the INR was within the therapeutic range for 2 consecutive days; in other words, enoxaparin was stopped prematurely in 21 patients (42.9%). Warfarin was restarted a mean 3 days after a surgery or procedure, and the mean time until INR reached the therapeutic range for the 2 consecutive days after the surgery or procedure was 15 days.
Outcomes
None of the 49 patients under bridging therapy had thromboembolic complications within 30 days of the procedure (Table 3), and the overall 30-day mortality rate was 0%. Major bleeding occurred in 2 patients (4.1%), a hemarthrosis in a patient who had a total knee replacement arthroplasty and a gross hematuria in a patient who underwent a percutaneous nephrolithotomy. Both of them recovered after cessation of anticoagulation therapy, packed RBC transfusion, and conservative treatment, without vitamin K administration.

DISCUSSION
In this study, efficacy was assessed in bridging anticoagulation with therapeutic-dose enoxaparin in 20 patients (41%) with VTE within 3 months (a high risk of recurrence), 11 patients (22%) with VTE within 3–12 months, and 16 patients (33%) with active malignancy, both moderate risks of recurrence (111213). There were no thromboembolisms, in contrast with another study that found 1.8% occurrence in a similar population of both high-risk patients who received bridging therapy and low-risk patients who did not (14). Fourteen patients who had VTE within > 12 months without cancer were deemed low risk and had no embolism 30 days after bridging. Our findings demonstrate that bridging therapy with enoxaparin is feasible and associated with a low incidence of thromboembolic complications.
The mean time when INR reached the therapeutic range of 2 to 3 for the 2 consecutive days after the surgery or procedure was 15 days (range, 4–47), which is longer than the 3.3 to 4.3 days that was found in another study (15).
During perioperative bridging, withdrawal of oral anticoagulants can place patients in a hypercoagulable state and increase their risk of stroke (16). Recently, Schulman et al. (17) showed that doubling doses for the first 2 postoperative days resulted in more patients having a therapeutic INR on days 5 and 10 compared with their usual doses without increased risk of bleeding.
Two major bleeding events in this study occurred following a major orthopedic surgery and a urologic procedure, both of which are associated with high risk of bleeding (6). Of the 49 patients in this study, 29 (59%) underwent major surgeries or procedures that had high risk of bleeding. The rates of major bleeding for minor and major surgeries or procedures, 0% and 4.1%, respectively, corresponded well with those (0.9%–6.7%) reported in recent, large, prospective studies of bridging therapy in which major bleeding occurred in patients who underwent major surgery (571018).
LMWH is the preferred bridging regimen. It has greater bioavailability and a more predictable dose response than unfractionated heparin (UFH) (571819). Jaffer et al. (20) reported that the risk of major bleeding is strongly associated with the use of postoperative therapeutic doses of heparin/LMWH based on the analysis of practice patterns at 9 hospitals. Low-dose LMWH/UFH may be considered an alternative option during resumption of anticoagulant bridging, particularly after major surgery (12).
Recently there are controversial views on perioperative anticoagulation in regard to bleeding complication. Douketis et al. (21) showed forgoing bridging anticoagulation was noninferior to perioperative brdging with LMWH for patients with atrial fibrillation who need to interrupt the warfarin for an elective operation. Mathew et al. (22) reported that therapeutic dose bridging was associated with 2.5 to 3-fold increased risk of major bleeding compared with prophylactic dose bridging.
Because there is no consensus on a bridging protocol, clinicians must estimate and balance the risk of postoperative major bleeding and thromboembolic events in patients who receive full-dose parenteral anticoagulation perioperatively while oral anticoagulant therapy is interrupted (232425). The first step in bridging management is to assess the risk of thromboembolic events during cessation of anticoagulation. This study suggests that bridging therapy with a therapeutic twice-daily dose of enoxaparin can be used safely for patients who are undergoing major or minor surgeries or procedures.
Recently, direct oral anticoagulants (DOACs) (i.e., dabigatran, rivaroxaban, apixaban, or edoxaban) are being increasingly prescribed to treat VTE and prevent stroke in atrial fibrillation. Annually, approximately 10% of those patients will need to interrupt DOACs for an elective procedure (2627). The study on the safety of perioperative management of DOACs using a specified protocol based on the creatinine clearance and procedure-related bleeding risk is underway, and the results are expected.
To our knowledge, this is the first study in Korea that assessed efficacy and safety in bridging therapy with LMWH during temporary interruption for an elective procedure or surgery in patients who were on chronic oral anticoagulant therapy. However, there are limitations to this study that should be addressed. Firstly, this was retrospective study at a single center. Secondly, the population size of this study was too small (n = 49) to generalize the result of this study to clinical practice. Thirdly, there was no comparable group regarding perioperative bridging therapy. Fourthly, the post-procedural patient follow-up was limited to 30 days. Consequently, our findings may underestimate the risk of thromboembolic events because clinical manifestations of periprocedural thrombus formation, such as embolic stroke or valve thrombosis, may be delayed over a month after warfarin interruption (282930). Consequently, our findings may not be generalizable to all patients planning to undergo bridging.
In conclusion, our findings demonstrate that bridging therapy with therapeutic-dose enoxaparin is feasible and associated with a low incidence of major bleeding and thromboembolic complications. However, the optimal approach to managing patients who require temporary interruption of warfarin or DOACs for invasive procedures is still uncertain and requires evaluation in randomized controlled trials.
 XML Download
XML Download