

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Laparoscopic radical prostatectomy (LRP) can be described as a clean-contaminated operation (1). During surgery, opening of the urogenital tract is inevitable and Foley catheterization is mandatory after the procedure (2). Owing to the minimally invasive nature of the procedure and the necessity for Foley catheterization, the administration of prophylactic antibiotics is an indispensable step in the attempt to prevent postoperative infectious complications.
Antibiotic prophylaxis during the perioperative period is widely accepted as a requirement in open and LRP, and significantly reduces the rate of acquiring a febrile urinary tract infection (UTI) and surgical site infections (SSIs) (34). Unfortunately, only few studies have reported on the effect of antibiotic prophylaxis on radical prostatectomy (RP). (456). Moreover, the focus of these studies was infections at the surgical site only, and did not include risk factor assessment. In prostatectomy, the urinary tract is opened during the procedure; thus, postoperative bacteriuria is probably the main source of postoperative infectious complications.
Therefore, it is reasonable to identify the risk factors for postoperative bacteriuria or infectious complications and the effectiveness of prophylactic antimicrobial therapy for LRP. There is currently no information on the risk factors for infectious complications associated with LRP in Korea. In addition, the Health Insurance Review & Assessment Service of Korea recently recommended a short duration of prophylactic antibiotics in patients undergoing RP without any Korean report of evidence. Therefore, we evaluated the risk factors for infectious complications after laparoscopic prostate surgery, as well as the efficacy of antibiotic prophylaxis in relation to the duration of administration.
MATERIALS AND METHODS
Study population
We evaluated a total of 428 patients who underwent laparoscopic prostatectomy at a single institution in Korea, from January 2012 to April 2015. The inclusion criteria were as follows: 1) Patients administered intravenous second-generation cephalosporin antibiotics 30 to 60 minutes before surgery; and 2) Patients who underwent urinalysis and urine culture by collection of a midstream sample 3 to 5 days preoperatively, and patients at the time of Foley catheter removal 1 to 2 weeks postoperatively. On the other hand, patients who had no follow-up urinalysis and urine culture examination were excluded. In addition, 8 patients who had received other types of antimicrobial prophylaxis were excluded.
A total of 313 consecutive patients were finally recruited and divided into 2 groups, according to the duration of administration of antimicrobial prophylaxis. Group 1 consisted of 153 (49%) patients who received a second-generation cephalosporin for 2 days (4 doses or less than 4 doses) 30 minutes before surgery and through the next day, while 160 (51%) patients were administered prophylaxis for more than 2 days (more than 4 doses) (group 2). The incidence of postoperative bacteriuria, asymptomatic bacteriuria, SSI, remote infection (RI), and unexplained fever (> 37.8°C) was retrospectively investigated.
All data were recorded retrospectively. The clinical parameters subjected to analysis were age, prostate volume, prostate-specific antigen level, operative time (minutes), duration of postoperative catheterization, recent (within 2 weeks) or preoperative UTI, presence of preoperative Foley catheterization, duration of antibiotic therapy (intravenous), presence of diabetes mellitus (DM), operative method, and infectious complication rate.
Definitions of postoperative infectious complications
We chose postoperative bacteriuria as the primary outcome parameter. As we were aware of the possible lack of clinical significance of bacteriuria, our secondary outcome parameters (postoperative infectious complications) were asymptomatic bacteriuria, SSI, RI, and unexplained fever (> 37.8°C).
Definition of SSI
In this study, postoperative SSI and RI were classified and defined according to the guidelines of the Centers for Disease Control and Prevention (CDC) (2). Infections were classified as superficial incisional (which involved only skin or subcutaneous tissue, and excluded stitch-related abscesses), deep incisional (which involved deep soft tissue, bone, or joint), and organ/space SSI. RI included respiratory infection, bacteremia/septicemia, and UTI.
Administration of antibiotics
All patients received initial intravenous antibiotics 30 to 60 minutes before surgery. Second-generation cephalosporins were used for this study.
Statistical analysis
Statistical analysis was performed using SPSS software, version 17.0 (SPSS Inc., Chicago, IL, USA). Descriptive analysis was performed to assess patient demographics. Univariate and multivariate logistic regression analyses (stepwise backward procedure) were performed to assess the associations of clinical parameters with infectious complications. Statistical significance was set at P < 0.05 for all analyses.
RESULTS
Baseline demographics
The total mean age of the enrolled patients was 67.3 ± 5.6 years, and the mean prostate volume was 32.2 ± 14.1 mL. The total frequencies of DM, recent UTI, preoperative UTI, and preoperative Foley catheter placement were 15.7%, 1.6%, 5.1%, and 1.3%, respectively. Differences in these parameters between both groups were not statistically significant as shown in Table 1.
Table 1
Baseline characteristics of patients
Of the 313 patients, 272 underwent LRP and 41 underwent robot-assisted LRP (RALRP). There was significant difference of operation type between group 1 and 2. Group 2 (16.9%) was performed more RALRP than group 1 (9.2%) (P = 0.046). The mean operative duration was 185.7 ± 53.4 minutes. Operative duration was longer in group 2, possibly because of the operation type (pure laparoscopic vs. robot-assisted). The mean durations of postoperative Foley catheterization and drain placement were 14.1 ± 5.5 days and 4.8 ± 3.6 days, respectively. The difference in duration of catheterization and use of a surgical drain between the 2 groups was not statistically significant.
The overall incidence of postoperative bacteriuria was 50.8%, but was significantly higher in group 1 (56.9%) than in group 2 (45%) (P = 0.042). Postoperative infectious complications developed in 174 patients (55.6%), with the prevalence being significantly higher in group 1 (61.4%) than in group 2 (50%) (P = 0.042). The incidence of asymptomatic bacteriuria, RI, and unexplained fever was not significantly different between the 2 groups. However, the incidence of SSI was significantly higher in group 1 (5.2%) than in group 2 (0.6%) (P = 0.018; Table 2).
Table 2
Perioperative characteristics
Clinical parameters associated with postoperative infectious complications
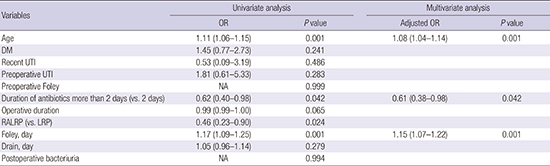
Univariate analysis revealed that older age (odds ratio [OR], 1.11; 95% confidence interval [CI], 1.06–1.15; P = 0.001), duration of antibiotics administration of more than 2 days (OR, 0.62; 95% CI, 0.40–0.98; P = 0.042), RALRP (OR, 0.46; 95% CI, 0.23–0.90; P = 0.024), and duration of Foley catheterization (OR, 1.17; 95% CI, 1.09–0.25; P = 0.001) were risk factors for postoperative infectious complications. Multivariate analysis revealed that older age (OR, 1.08; 95% CI, 1.04–1.14; P = 0.001), duration of antibiotic administration of more than 2 days (OR, 0.61; 95% CI, 0.38–0.98; P = 0.042), and duration of Foley catheterization (OR, 1.15; 95% CI, 1.07–1.22; P = 0.001) were independently associated with postoperative infectious complications (Table 3).
Table 3
Associations between clinical parameters and infectious complications after RP, and multivariate analysis of clinical parameters independently affecting infectious complications after RP

Infectious complications include asymptomatic bacteriuria, SSI, RI, and unexplained fever > 37.8°C.
RP = radical prostatectomy, OR = odds ratio, DM = diabetes mellitus, UTI = urinary tract infection, LRP = laparoscopic radical prostatectomy, RALRP = robot-assisted laparoscopic radical prostatectomy, SSI = surgical site infection, RI = remote infection.
Clinical parameters associated with postoperative SSI
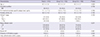
Univariate analysis revealed that antibiotic administration for more than 2 days (OR, 0.11; 95% CI, 0.14–0.92; P = 0.042), duration of Foley catheterization (OR, 0.85; 95% CI, 0.72–1.02; P = 0.085), and duration of use of surgical drain (OR, 1.11; 95% CI, 1.01–1.21; P = 0.031) were risk factors for SSI. Multivariate analysis revealed that antibiotic administration for more than 2 days (OR, 0.11; 95% CI, 0.11–1.04; P = 0.054), duration of Foley catheterization (OR, 0.81; 95% CI, 0.71–0.93; P = 0.004), and duration of use of surgical drain (OR, 1.29; 95% CI, 1.14–1.46; P = 0.001) were independently associated with postoperative SSI (Table 4).
Table 4
Associations between clinical parameters and SSI after RP, and multivariate analysis of clinical parameters independently affecting SSI after RP

Results of culture in patients with asymptomatic bacteriuria and SSI
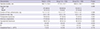
The most common species detected in patients with asymptomatic bacteriuria were enterococcus species, and resistance to quinolone was observed in the isolates obtained from 15 of 149 (10%) patients (Table 5). Only 1 of 9 patients with SSI had bacteremia (Table 6).
Table 5
Results of urine culture performed for patients with asymptomatic bacteriuria
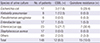
Table 6
Results of cultures performed for patients with SSI

DISCUSSION
In the present study, the postoperative infectious complication rate was 55.6%, and included postoperative asymptomatic bacteriuria (47.3%), fever (2.2%), SSI (2.9%), and RI (4.8%). The duration of antibiotic administration affected the postoperative infectious complications. We examined the results of urine cultures, using urine samples collected at the time of Foley catheter removal following RP. Despite prophylactic antibiotics, a large portion (50.8%) had bacteriuria. A more than 2-day administration of antimicrobial prophylaxis was associated with decreased bacteriuria and infectious complications, especially SSI.
LRP is classified as a clean-contaminated surgery (2). The Best Practice Policy panel of the American Urological Association recommends a course of intravenous cephalosporins lasting 24 hours in clean-contaminated urological operations involving the opening of the urinary tract. The panel also advocates 24 hours of oral antibiotics (fluoroquinolones or trimethoprim-sulfamethoxazole [TMP-SMX]) at the time of external urinary catheter removal if the patient has infection-related risk factors. Alternatively, a culture-directed antimicrobial can be administered for documented bacteriuria, or treatment can be omitted if urine culture shows no growth (7). However, these recommendations were based on the findings of 2 randomized controlled trials that involved patients who underwent transurethral surgery. In these studies, patients receiving cefotaxime (a single dose in 1 study, a 3-day course in the other) at the time of catheter removal had a significantly reduced postoperative complication rate and length of hospital stay compared to a control group not receiving antimicrobials at the time of catheter removal (89). However, there are no specific recommendations concerning antibiotic prophylaxis in LRP. In general, the incidence of postoperative infections after laparoscopic surgeries is lower than that after open surgeries, suggesting that only short-term prophylactic antimicrobial use is necessary for laparoscopic surgeries. However, the evidence is limited, and prophylaxis is largely empirical. According to the Japanese guidelines for open urological surgery, ampicillin (AMP) should be administered within 3 days (72 hours). Single-dose or 1 day of AMP is recommended for a clean operation; 2 or 3 days of AMP is recommended for clean-contaminated operations. The recommended AMP dosing for laparoscopic urological surgery is similar to that for open surgery (10).
After RP, primary healing of the vesicourethral anastomosis is important to the recovery of normal voiding function. Continuous urinary catheter drainage is typically used; however, with each day that the catheter is left in place, the risk of bacterial colonization increases (11). Catheter-associated bacteriuria is usually asymptomatic and uncomplicated, and resolves spontaneously after catheter removal; however, up to 30% of patients develop genitourinary or systemic symptoms (12). In this study, postoperative bacteriuria developed in 50.8% of patients, and 6.9% (11/159) had symptomatic UTI.
The best strategy for managing catheter-acquired bacteriuria after LRP has not been investigated, but studies in the non-urologic setting have shown beneficial effects of antibiotic treatment once bacteriuria has been identified. In a randomized controlled trial comparing oral antimicrobials with no treatment for asymptomatic bacteriuria following short-term catheter use in women, bacteriuria resolved in 81% of patients treated with antimicrobials. In contrast, bacteriuria resolved in only 36% of untreated patients, and another 17% of untreated patients went on to develop UTI symptoms (13). There are few studies on antimicrobial prophylaxis in RP, and most have focused on SSI and not UTI, as in transurethral resection of the prostate (TURP). No consideration has been given to postoperative UTI in prostatectomy, which carries a higher risk of bacteriuria than does TURP, owing to the long-term postoperative catheterization associated with the procedure. According to this study, clinicians should be aware of the high risk for bacteriuria in patients who undergo LRP.
Because laparoscopic surgery is thought to be less invasive, the incidence of SSI in laparoscopic procedures could be lower than that in open procedures. Rassweiler et al. (14) reported that SSI occurred in 5 of 219 (2.3%) patients undergoing open RP, but in just 1 of 438 (0.3%) undergoing LRP. However, there was no comparison between pure LRP and RALRP. In this study, there was no difference in the incidence of infectious complications between pure LRP and RALRP. However, shorter duration of antibiotics, shorter duration of Foley catheterization, and longer placement of drains were associated with SSI.
In the present study, the duration of antibiotic administration affected the outcome of postoperative infectious complications. These data show that prostatectomy is associated with a high incidence of postoperative UTI and bacteriuria, as is TURP. Thus, it is logical to apply the antibiotic prophylaxis regimen of TURP to prostatectomy. In TURP, the prophylactic effect of multiple doses of cephalosporins for 24 to 72 hours is more effective than that of a single dose (1516). In the Japanese guidelines, RP is considered to be a clean-contaminated operation; therefore, antibiotic prophylaxis is recommended within 3 days (10). In Asia, the incidence of antibiotic resistance is higher than that in Western or European countries, which recommend single-dose or < 24-hour antibiotic prophylaxis. When we consider the results of this study and Japanese guidelines, antibiotic prophylaxis for 3 days (i.e., more than 2 days) might be appropriate for Asian populations.
No randomized controlled trials on antibiotic prophylaxis vs. placebo/no antibiotics in total prostatectomy have been performed. Thus, there is a lack of baseline data on the infectious profile of this frequently performed operation. A few retrospective and prospective cohort studies have evaluated SSI and catheter-associated bacteriuria following different antibiotic regimens. They concluded that the frequency of wound infection is low and that a single oral antibiotic dose is sufficient (45617). However, in this study, the duration of antibiotics was associated with SSI; a duration more than 2 days was associated with decreased infectious complications (OR, 0.61; 95% CI, 0.38–0.98; P = 0.042) and SSI (OR, 0.11; 95% CI, 0.11–1.04; P = 0.054).
In terms of antibiotic type, there is a lack of evidence to suggest the routine use of one class of antibiotics vs. another, with aminoglycosides, fluoroquinolones, cephalosporins, and TMP-SMX all demonstrating efficacy in large meta-analyses (15). In a Korean multicenter study, the prophylactic efficacy did not differ according to the antibiotic type, and a first or second-generation cephalosporin was a reasonable option to reduce antibiotic resistance when compared to a third generation cephalosporin (18).
Several studies have investigated risk factors for postoperative infectious complications after TURP (18). Well-documented risk factors include preoperative bacteriuria, duration of the operation, rupture of closed drainage systems, duration of postoperative catheterization, and DM. However, there are no well-defined risk factors for LRP. The incidence of postoperative infectious complications and SSI after LRP in this study was 55.6% and 2.9%, respectively. Older age, antibiotic administration for more than 2 days, and duration of Foley catheterization were independently associated with postoperative infectious complications. Shorter duration of antibiotics use, shorter duration of Foley catheterization, and longer duration of drain use were independently associated with SSI. In urologic surgical practice, the prevention of postoperative infectious complications is important, but few studies have evaluated the risk factors in such settings. Therefore, it is valuable to evaluate these risk factors as they relate to prostate surgery and the efficacy of prophylactic antibiotics in the era of antibiotic resistance.
The current study had limitations. Firstly, the antimicrobial regimens and durations are not standardized in Korea. Thus, we focused on second-generation cephalosporins. Our findings should be interpreted cautiously, because each center has different clinical practice guidelines for antimicrobial prophylaxis in surgery. Second, we did not consider locoregional antimicrobial resistance in our selection of antibiotics. Third, this study used a retrospective and non-randomized methodology. Lastly, heterogeneous operative methods can lead to the possibility of an unknown cofounder associated with infectious complications. However, to our knowledge, this is the first study in Korea to evaluate postoperative infectious complications after RP. No previous studies have investigated the risk factors for postoperative UTI after prostatectomy. With the paucity of data addressing this issue among the Korean population, the present study will serve as a basis for future prospective research. Evidence concerning perioperative infections in the urological field is limited. The presence of postoperative bacteriuria was not associated with SSI. Further studies on long-term complications in patients with postoperative UTI, such as urethral stricture, will be required. Further studies to gather additional evidence are necessary to establish guidelines, tailored to the Korean population.
In conclusion, the incidence of postoperative bacteriuria and SSI was higher in patients who received antibiotics for a short duration. Based on our results, older age, short duration of administration of antibiotics, and prolonged Foley catheterization affect postoperative infectious complications associated with LRP. Prolonged drain use is associated with SSI, whilst longer duration of antibiotic administration and prolonged Foley catheterization are associated with decreased SSI. Additional research with multi-center, prospective, well-designed randomized controlled trials is needed to further evaluate infectious complications after LRP.
 XML Download
XML Download