

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Alcoholic liver disease (ALD) is a leading cause of cirrhosis and one of the most common indications for liver transplantation (LT) in Western countries, accounting for about 20%–40% of all primary transplants (123). Despite a high rate of recidivism, outcomes for patients who undergo LT for ALD have been reported to be similar to those of patients who undergo LT for most other diagnoses (345). Because deceased donor organs are public resources, the finding that post-LT outcomes are comparable for patients with ALD and other etiologies is especially important for deceased donor liver transplantation (DDLT) into patients with ALD.
Hepatitis B virus (HBV) is endemic in Korea, with an estimated 5%–6% of the general population being carriers (6). HBV, however, has been controlled by a national vaccination program for neonates and by antiviral treatment under a national surveillance program (7). Thus, the proportion of patients undergoing DDLT for ALD has risen sharply, from 6.8% in 2010 to 27.5% in 2014, while the proportion of patients undergoing living donor liver transplantation (LDLT) has increased gradually, from 8.3% in 2010 to 8.9% in 2014 (8). ALD has become the second most frequent indication for LT in Korea, following HBV.
The shortage of deceased donor organs in East Asian countries, including Korea, indicates a need for a fair therapeutic strategy and strict application of narrow selection criteria for DDLT in these countries. However, most transplantation centers in Korea, as well as Korean Network for Organ Sharing (KONOS) guidelines, do not require a minimum abstinence period of 3–6 months prior to LT. This likely results from the previously low proportion of patients with ALD undergoing DDLT (8). Moreover, more than 50% of DDLT recipients in Korea were 2A status, making them too sick to apply pre-transplantation abstinence.
Few studies to date have compared post-LT outcomes in patients undergoing DDLT for ALD and HBV in Asian countries in which LDLT is dominant, HBV is endemic and a minimum abstinence period before LT is not mandatory. This study therefore retrospectively compared post-LT outcomes of Korean patients who underwent DDLT for cirrhosis due to HBV and ALD, the latter without a pre-transplant minimum abstinence period.
MATERIALS AND METHODS
From January 2010 to December 2014, 220 adult patients underwent primary DDLT at Seoul National University Hospital. Patients transplanted for other than HBV and ALD were excluded, as were patients transplanted for combined HBV and hepatitis C virus (HCV) infection, and combined ALD and viral hepatitis. ALD was diagnosed by the hepatologist or transplant surgeon based on guidelines of the American Association for the Study of Liver Diseases and the Korean Association for the Study of the Liver (910). The medical records of all included patients were retrospectively reviewed and overall survival compared in patients who underwent DDLT for ALD and HBV. Subgroup analysis was also performed excluding patients with hepatocellular carcinoma (HCC), as determined by explant liver pathology, to rule out any effect of malignancy.
Pre-LT evaluation
Indications for LT were based on each patient's history and clinical and laboratory findings according to a multidisciplinary approach. Although our center did not mandate a specified period of alcohol abstinence, all patients and their families were interviewed by a psychiatrist. ALD patients were asked to strictly abstain from alcohol, indicating an intention of lifetime abstinence.
Post-LT management and follow-up
After LT, maintenance immunosuppression was based on a triple regimen, including tacrolimus, mycophenolate mofetil (MMF), and a corticosteroid. HBV patients received a combination prophylactic regimen of anti-hepatitis B immunoglobulin and an antiviral agent. Routine biochemical examinations were performed every day during the patient's hospital stay. Outpatient follow-up visits were usually conducted once a week during the first month after discharge, twice a month during the second and third months, monthly during the first year, and every 3 or 4 months thereafter, or when required. One-year protocol biopsy was recommended for patients without a high risk of bleeding. Routine biochemical examinations, including liver function tests, were performed at every follow-up visit. Patients showing significant changes in liver function tests were asked to return for additional follow-up shortly thereafter or to be admitted to hospital for observation, depending on the severity of abnormalities. Liver function was rechecked and evaluated by blood tests, imaging, and/or liver biopsy, if needed.
Statistical analysis
Statistical analyses were performed using SPSS software (version 22; SPSS Inc., Chicago, IL, USA). Results are expressed as means and ranges or as the number and percentage of patients. Continuous variables were compared using Student's t-tests and categorical variables using the χ2 test or Fisher's exact test, as appropriate. Overall survival rates were estimated by the Kaplan-Meier method. The log-rank test and Cox proportional hazards regression analysis were used to evaluate the association between patient characteristics and overall survival in univariate and multivariate analyses. A P value ≤ 0.05 was considered statistically significant.
RESULTS
Patient demographics
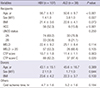
Of the 220 patients who underwent DDLT between January 2010 and December 2014 at our center, 145 were eligible for this study, including 107 patients who underwent DDLT for HBV alone and 38 who underwent DDLT for ALD alone. Patient characteristics are presented in Table 1. Patients in the ALD group were significantly younger (50.6 vs. 56.7 years; P < 0.001), were more likely to be men (3.8:1.0 vs. 1.4:1.0; P = 0.027), and less likely to have pathologically proven HCC (15.6% vs. 52.3%; P < 0.001) than patients in the HBV group. Mean Child-Pugh score was significantly higher in the ALD group (11.4 vs. 10.7; P = 0.003), whereas Model for End-stage Liver Disease (MELD) scores were similar (25.1 vs. 22.4; P = 0.114). Seventy-four patients (69.2%) in the HBV group and 30 (78.9%) in the ALD group had UNOS status 2A, but the difference was not statistically significant (P = 0.250). There were no between-group differences in donor age, sex, and body mass index (BMI), and no difference in cold ischemia time.
Table 1
Recipient and donor characteristics
Post-LT outcomes
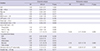
Complications were graded according to the classification system proposed by Clavien et al. (11). Grade I (25.2% vs. 47.4%; P = 0.011) and grade II (29.9% vs. 60.5%; P = 0.001) complications were more frequent in the ALD group, whereas grade IIIA to grade V complications were comparable in the 2 groups. The major complications in both the HBV and ALD groups were infection (16.8% vs. 47.4%; P < 0.001) and neurologic complications (14.0% vs. 28.9%; P = 0.039), with both being significantly more frequent in the ALD group. Other complications in the HBV and ALD groups included hemorrhage (3.7% vs. 18.4%; P = 0.007) and biliary complications (2.8% vs. 13.2%; P = 0.029), both of which were significantly more frequent in the ALD group. There were no significant differences in other complications.
After discharge, higher percentages of patients in the ALD than in the HBV group were admitted due to abnormal liver function tests (33.3% vs. 16.0%; P = 0.027) and visited a psychiatrist for psychiatric problems other than alcohol reuptake (38.9% vs. 7.0%; P < 0.001). Psychiatric problems included depressive disorder, anxiety disorder, and sleep disturbance. Hospital stay and number of admissions were comparable in the 2 groups (Table 2).
Table 2
Post-LT outcomes

One-year protocol liver biopsies were obtained from 51 of the 107 HBV patients (47.7%) and from 14 of the 38 ALD patients (36.8%). Pathologic findings of fibrosis (64.3% vs. 25.5%; P = 0.011), necrosis (35.7% vs. 11.8%; P = 0.049), and fatty changes (35.7% vs. 9.8%; P = 0.031) were more frequent in the ALD group, whereas pathologic findings of acute cellular rejection and inflammation were similar in the 2 groups.
Although serum gamma-glutamyl transferase (GGT) levels 7 days after LT were similar in the 2 groups, serum GGT levels after 1 year were significantly higher in the ALD than in the HBV group (90.5 vs. 39.9; P = 0.025).
Patient survival
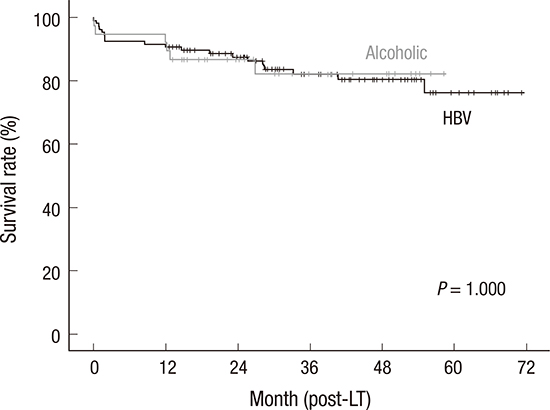
The 1-year and 3-year overall survival rates of patients were 90.7% and 82.1%, respectively, in the HBV group, and 92.1% and 82.3%, respectively, in the ALD group. There were no significant differences in overall survival rates between the 2 groups (P = 1.000; Fig. 1A).
Fig. 1
Kaplan-Meier analysis of overall survival in (A) all patients and (B) patients without HCC.
HCC = hepatocellular carcinoma, LT = liver transplantation, HBV = hepatitis B virus.

The most common causes of death were malignancy (42.1%) and infection (31.6%) in the HBV group and infection (50.0%) and liver dysfunction (33.3%) in the ALD group. Other causes of death were cerebrovascular disease, intra-abdominal hemorrhage, cardiopulmonary disease, and accidents.
Univariate analyses showed that factors significantly associated with patient survival were high serum GGT level 1 year after LT (< 70 vs. ≥ 70 IU/L), pathologic findings of necrosis on 1 year protocol liver biopsy, and admission due to abnormal liver function tests. HCC was not a significant factor. Multivariate analysis showed high serum GGT (≥ 70 IU/L) after 1 year was the only factor independently prognostic of overall survival (Table 3).
Table 3
Risk factors of mortality after LT in univariate and multivariate analysis
Subgroup analysis of patients without HCC
Because HCC is highly prevalent in patients with HBV, the effects of HCC were ruled out by subgroup analysis that excluded patients with HCC, based on explant pathology. Subgroup analysis identified 51 HBV patients and 32 ALD patients without HCC (Table 4).
Table 4
Post-LT outcomes of patients without HCC

Data are shown as mean ± standard deviation or number (%).
HCC = hepatocellular carcinoma, HBV = hepatitis B virus, ALD = alcoholic liver disease, BMI = body mass index, UNOS = United Network for Organ Sharing, MELD = Model for End-stage Liver Disease, CTP = Child-Turcotte-Pugh, LFT = liver function test, POD = postoperative day, ACR = acute cellular rejection, GGT = gamma-glutamyl transferase.
Patients in the ALD group were significantly younger (50.6 vs. 55.5 years; P = 0.003), had a higher proportion of men (3.6:1.0 vs. 1.0:1.0; P = 0.027), and had a significantly higher BMI (22.3 vs. 20.5 kg/m2; P = 0.039). Recipient's UNOS status, medical MELD score, and Child-Pugh score were similar in the 2 groups. There were no differences in donor age, sex, and BMI, or in cold ischemia time.
Grade I (46.9% vs. 21.6%; P = 0.016) and grade II (59.4% vs. 23.5%; P = 0.001) complications were significantly more frequent in the ALD than in the HBV group, whereas the rates of grade IIIA to grade V complications were comparable. Infection was the most common cause of death in both the HBV (50.0%) and ALD (50.0%) group. There were no statistically significant differences in cause of death between the 2 groups, and no significant differences in hospital stay, admission due to abnormal liver function tests, and number of admissions. Psychiatric problems after discharge (43.3% vs. 8.3%; P < 0.001) and 1-year biopsy findings of fatty change (36.4% vs. 6.9% vs. 36.4%; P = 0.039) were more frequent in the ALD group. Pathologic findings of acute cellular rejection, fibrosis, inflammation, and necrosis were similar. Serum GGT levels were similar in the 2 groups 7 days and 1 year after LT.
The 1-year and 3-year overall survival rates were 94.1% and 89.4%, respectively, in the HBV group, and 90.6% and 79.1%, respectively, in the ALD group. These rates did not differ significantly (P = 0.244; Fig. 1B).
DISCUSSION
Although the follow-up duration in this study was relatively short, the 1- and 3-year patient survival rates following DDLT for ALD of 92.1% and 82.3%, respectively, were similar to the overall survival rates previously reported in Europe and the USA (312). Moreover, the survival rates following DDLT for ALD were comparable with those of DDLT for HBV, with the latter group having 1- and 3-year survival rates of 90.7% and 82.1%, respectively. This finding was similar to that of other studies, which reported that outcomes of patients transplanted for ALD were at least as good as those for patients with most other diagnoses, and better than outcomes of patients transplanted for HCV (345).
Most transplant centers in Western countries require that patients with ALD abstain from alcohol for 3–6 months (13141516). However, early LT without an abstinence period has been reported to improve survival in patients with a first episode of severe alcoholic hepatitis not responding to medical therapy (17). Both KONOS guidelines and those of our center do not specify duration of abstinence in patients undergoing LT for ALD. Furthermore, we found that 69.2% of patients in our HBV group and 78.0% in our ALD group had UNOS status 2A. As some patients with high status may not survive a prolonged abstinence period, we do not mandate a minimum abstinence period prior to LT. Rather, all patients and their families were interviewed by a psychiatrist. In the absence of a specific abstinence period before DDLT, patient survival after LT was comparable in the 2 groups. Although our study showed that several complications were significantly more frequent in the ALD than in the HBV group, including infection and neurologic, biliary, and hemorrhagic complications, the differences were no longer significant after subgroup analysis of patients without HCC. The comparable mortality rates observed in the HBV and ALD groups may be associated with the latter receiving continuous post-LT psychological and family support, in addition to younger age and lower proportion of patients with HCC (18). Racial homogeneity or genetic polymorphism may also be related to this result (1920). These findings indicate a need to reassess the value of abstinence periods prior to DDLT for patients with ALD, as well as the exclusion of these patients from DDLT because they have not completed a minimum abstinence period. However, when possible, abstinence periods may be recommended to reduce DDLT complications and improve post-LT outcomes in ALD patients.
We also found that serum GGT level 1 year after LT was significantly higher in the ALD than in the HBV group. Patients in the ALD group may return to a pattern of alcohol consumption, with many studies showing an association between alcohol consumption and GGT level (212223). GGT may in part be a marker of oxidative stress associated with ethanol metabolism. Moreover, the incidence of fatty changes was found to be higher in patients who returned to alcohol consumption than in those who remained abstinent (24). We found a higher rate of 1-year post-LT pathology diagnosed biopsy findings of fatty changes in the ALD group. Patients in this group may also have more genetic polymorphism, e.g., in the patatin-like phospholipase domain protein 3 gene, which has been associated with liver fat content (1920). However, this study did not evaluate alcohol reuptake or genetic polymorphisms. Further studies are required to validate these findings.
Our results show that ALD patients have more psychiatric morbidities, other than alcohol reuptake, after transplantation. A higher percentage of patients in this group visited a psychiatrist for depression, anxiety disorder, or sleep disturbance. In contrast, a previous study reported similar rates of psychiatric morbidities in ALD patients and controls at follow-up (18). However, other studies have shown an association between psychiatric comorbidity, defined as a psychiatric history before LT, and the risk of post-LT alcohol relapse (1525). These findings, taken together with ours, indicate the importance of careful psychiatric assessment before and after LT in patients with ALD.
No patient in either group died of de novo tumors. De novo tumors occurred in only 4 patients (3.7%) in the HBV group, but in none of the ALD group. In contrast, Western studies have reported higher rates of de novo malignancies among alcoholics (2627). These discrepancies may have been due to our relatively short follow-up time, differences in data sources, and differences in patient country of origin.
Subgroup analysis, after excluding patients with HCC, showed that mean BMI was significantly higher in the ALD than in the HBV group. This finding was in agreement with reports showing that ALD is related to overweight and obesity (282930). However, another study showed that body weight and BMI are significantly lower in heavy than in non-heavy drinkers (31). Body weight and BMI may depend on the severity of drinking. Although cold ischemia time was longer in the ALD group, this may have been due to the relatively small sample size. Cold ischemic time in Korea rarely exceeds 6 hours, with a 0.5 hours difference being unrelated to prognosis (32). After excluding patients with HCC, infection was the main cause of death of patients in both groups. Infectious complications after LT have been associated with the severity of underlying diseases (33). Patients with sustained alcohol toxicity often present with cardiovascular disease, pancreatitis, malnutrition, mental abnormalities, and damage to other organs, which may exacerbate the underlying disease (1). Thus, preoperative abstinence and a certain period of monitoring or management may reduce infectious complications and prolong survival.
This study had several limitations. First, it was retrospective in design, making us dependent on the completeness of patients' medical records. Second, the number of patients was relatively small and the follow-up period was relatively short. Thus, it was impossible to further classify patients according to their severity of drinking.
In conclusion, outcomes of DDLT were no worse for patients with ALD than for HBV in an HBV endemic area, even in the absence of a fixed abstinence period before LT. Careful psychiatric evaluation is required before and after transplant, with strict application of selection criteria reducing psychiatric complications and rates of readmission when compared with patients undergoing LT for HBV.
 XML Download
XML Download