

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The ATP-sensitive potassium channel (KATP channel) plays a crucial role in the regulation of pancreatic β-cell insulin secretion (1). Inactivating mutations in KCNJ11 or ABCC8 cause congenital hyperinsulinism presenting with persistent hypoglycemia in infancy (23). The most common causes of permanent neonatal diabetes mellitus (PNDM) are activating mutations in the KCNJ11 or ABCC8 genes that encode Kir6.2 or SUR1, respectively (45). Developmental delay, epilepsy, and neonatal diabetes (DEND) syndrome represents the most severe form of PNDM that is characterized by various neurologic features (6). Patients with intermediate DEND (iDEND) syndrome demonstrate less severe developmental delay without seizures (7).
A few cases of permanent neonatal diabetes have been reported in Korea (89). We describe the first case of DEND syndrome in a patient misdiagnosed with type 1 diabetes with long-term insulin treatment. The clinical course of the patient, molecular genetic analysis for confirmation of PNDM, and a successful switch to sulfonylurea therapy are reported.
CASE DESCRIPTION
A 50-day-old boy presented with fever and upper respiratory tract infection on May, 1996. The patient was born to non-consanguineous parents and was delivered by cesarean section with a birth weight of 2,750 g (−1.43 standard deviation score [SDS]). Hyperglycemia (306 mg/dL) was incidentally detected by laboratory tests. The infant was initially diagnosed with type 1 diabetes mellitus (DM) and treatment with subcutaneous insulin was initiated. Frequent partial seizures persisting 2 to 3 minutes were observed in the patient and had developed after birth. There were no loss of consciousness or postictal sleep. At 10 months of age, the patient was unable to hold his head up, make eye contact with others, or sit unassisted. Rehabilitation therapy was initiated due to a severe delay in motor development.
At 21 months of age, the Denver developmental test demonstrated a delayed developmental status in regard to visual contact, babbling response to name, almost absent facial expression, and a psychomotor developmental level of 3 months. Physical examination revealed generalized hypertonia with no dysmorphic features. Increased deep tendon reflex with pathologic reflexes such as Babinski reflex and ankle clonus were observed. Islet cell autoantibodies and serum insulin level were not determined. Serum C-peptide and 24-hour urine C-peptide levels were < 0.1 ng/mL and 0.2 μg/day, respectively. Abdominal ultrasound scan demonstrated a normal pancreas.
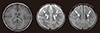
Electroencephalogram (EEG) showed spike discharges from the right centro-parietal area. At 21 months, magnetic resonance imaging of the brain demonstrated symmetric high signal intensity of the periventricular white matter on T2-weighted and fluid-attenuated inversion recovery (FLAIR) images, suggesting hypoxic encephalopathy or metabolic encephalopathy. No structural abnormalities were detected (Fig. 1). Treatment with antiepileptic drugs (oxcarbazepine, Trileptal®; Novartis Pharmaceuticals Corporation, Basel, Switzerland) was subsequently initiated.
Fig. 1
MRI of the brain at 21 months of age. The brain MRI demonstrates symmetric high signal intensity of periventricular white matter on T2-weighted and FLAIR images, suggesting hypoxic anoxic encephalopathy or metabolic encephalopathy. Myelination and migration of the underlying brain is normal. No other structural abnormalities including ventricle dilatation or encephalomalatic change are detected.
MRI = magnetic resonance imaging, FLAIR = fluid-attenuated inversion recovery.
The glycated hemoglobin (HbA1c) levels were up to 10% during the childhood and adolescent period, however, there were no complications such as diabetic retinopathy nor nephropathy. At 17.9 years of age, direct sequencing of the KCNJ11 gene identified a heterozygous mutation of c.602G>A (p.R201H) on February, 2014 (Fig. 2). Since then, treatment with sulfonylurea dose of 40 mg (gliclazide, Diamicron®; Servier Laboratories Ltd., Neuilly-sur-Seine, France) was initiated and well-tolerated. The insulin dose was gradually reduced. Following 3 months, insulin was discontinued with a gliclazide dose of 2.4 mg/kg/day (Fig. 3). The patient continued to have excellent glycemic control with a HbA1c level of 5.8% after 5 months. Antiepileptic therapy was discontinued following the absence of an abnormal spike or wave on EEG. However, the patient's psychomotor retardation was not observed to improve. Presently, the patient is 19.9 years of age and unable to communicate with others due to severe global developmental delay.
Fig. 2
Direct sequencing of the KCNJ11 gene. Partial sequences of KCNJ11 demonstrate a heterozygous mutation of c.602G>A (p.R201H).

Fig. 3
The clinical course of the patient with DEND syndrome. The insulin dose was tapered over 3 months and successfully switched to sulfonylurea (2.4 mg/kg/day). Serum C-peptide was undetectable (< 0.5 ng/mL) prior to sulfonylurea therapy. At 18.7 years of age, HbA1c was found to be 5.8%, indicating a well-controlled status following the switch to sulfonylurea.
DEND = developmental delay, epilepsy, and neonatal diabetes, HbA1c = glycated hemoglobin.

DISCUSSION
This study reports the first case of DEND syndrome in Korea with an activating mutation in KCNJ11 in a patient initially misdiagnosed with type 1 DM. Neonatal DM is a heterogeneous group of genetic disorders that results from a dysfunction of β-cell insulin secretion. The estimated incidence of neonatal DM has been reported to be 1 in 500,000 neonates (10). Neonatal DM is categorized into transient neonatal DM (TNDM) and PNDM. TNDM usually resolves within 3 to 6 months; however, long-term treatment is required in patients with PNDM (11). The majority of cases of TNDM result from abnormalities in the imprinted region of the chromosome 6q24 (1112). The most common causes of PNDM are activating mutations in KCNJ11 or ABCC8 genes (4). Each of these genes encode Kir6.2 and SUR1, which are subunits of the β-cell KATP channel (11011).
KATP channels are composed of hetero-octameric complexes with 4 SUR1 and Kir6.2 subunits. The KCNJ11 gene consists of a single exon and encodes a 390 amino acid protein. It is a crucial site for the ATP-binding mediating channel that plays an important role in the control of K+ channel selectivity through the pores (67). To date, more than 130 different mutations have been reported in the Human Gene Mutation Database (http://www.hgmd.org). Patients with diabetes due to KCNJ11 mutations affect the inhibitory effect of ATP, demonstrating decreased sensitivity of KATP channels (6). Consequently, the KATP channels remain open despite hyperglycemia, thereby reducing insulin secretion (713). Sulfonylurea inhibits the KATP channel and subsequently triggers insulin secretion by binding with its receptor to close the KATP channel (4). Functional studies have revealed that KATP channels that are heterozygous for the p.R201H mutation, which was found in our patient, exhibit a marked sensitivity to inhibition by tolbutamide (4).
KATP channels are involved in regulating insulin secretion from β-cells, glucagon secretion from α-cells, and glucagon-like peptide 1 (GLP1) secretion from intestinal L-cells (10). KATP channels are expressed in the brain, nerve, muscle, and pancreatic β-cells, implying an association with the neurological features observed in patients with PNDM (1011). In patients with DEND syndrome, the most severe form of PNDM, psychomotor developmental delay and epilepsy are manifested during the infantile period (611). The hallmark of DEND syndrome is neonatal DM, although it is not usually associated with diabetic ketoacidosis upon initial presentation. The DEND syndrome is characterized by the inability of patients to stand or talk in late childhood and generalized epilepsy within the first year of life (7). Most patients show developmental delay, symmetric muscle weakness usually affecting the lower extremities, and epilepsy with generalized EEG abnormalities (14). The patient reported here exhibited global developmental delay and DM at 50 days of age, suggesting DEND syndrome. On the contrary, iDEND syndrome is usually manifested with a less severe developmental delay and without epilepsy (714).
In conclusion, this study described the first patient with DEND syndrome in Korea that presented with PNDM, severe developmental delay, and seizures. Although neurologic symptoms cannot be corrected, sulfonylurea therapy may close the pancreatic KATP channel and not only improve glycemic control but also seizures, resulting in the discontinuation of antiepileptic drugs. Patients diagnosed with diabetes within the first 6 months of life should be screened for monogenic diabetes such as defects of the KCNJ11 or ABCC8 genes.
 XML Download
XML Download