

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Breast cancer is the most commonly diagnosed cancer in women worldwide. The advancements in early detection and systemic treatment have resulted in improved mortality and survival rates among patients diagnosed with breast cancer (12). Mammography is a simple and effective imaging modality and a standard test for breast cancer detection. The overall sensitivity of this procedure was commonly reported at 85%; however, in women with dense breast tissue, the technique has limited efficacy and has a reduced overall sensitivity of 68% (3).
Breast-specific gamma imaging (BSGI) is a new functional imaging modality that has been introduced in the diagnostic imaging of breast cancer. It was developed from the imaging modality of breast scintigraphy and offers superior intrinsic, spatial resolution compared with that of a conventional, gamma camera. BSGI has a detection sensitivity and specificity rate of 92%–96% and 71%–80%, respectively, for tumors, based on visual assessment (45). Additionally, in a comparison of BSGI and mammography, BSGI showed higher sensitivity and specificity rates during the screening of patients with dense or scarred breast tissue or in those with implants (678).
99mTc-sestaMIBI (MIBI) uptake of tumor in BSGI is affected by angiogenesis, regional blood perfusion, and mitochondrial membrane potential. In particular, mitochondrial density is a reflection of the proliferative activity of cells; thus, the accumulation of MIBI is higher in tumor cells than in normal breast tissue. Similarly, the uptake of MIBI differs according to the tumor biology and histopathologic characteristics of breast cancer. Previous studies have reported that the tumor-to-background ratio (TBR) of BSGI was correlated with some prognostic factors such as tumor size, histologic grade, axillary lymph node metastasis, and expression of estrogen receptor (ER)/progesterone receptor (PR) (910111213). However, very few studies have investigated the correlation of TBR with breast cancer subtype (913). Moreover, the method of TBR measurement, histologic type of breast cancer, and size of the tumor were different among previous studies, resulting in discordant results (91113).
Therefore, the purpose of this study was to determine whether correlation exists between TBR on BSGI and prognostic factors and subtypes of breast cancer, especially in invasive ductal carcinoma.
MATERIALS AND METHODS
Patients and study design
Sixty-seven patients with a recent diagnosis of invasive ductal carcinoma and who underwent preoperative BSGI were retrospectively enrolled between January 2014 and October 2015. They did not receive any treatment prior to BSGI, and surgical treatment was performed after BSGI. The exclusion criteria were as follows: 1) received neoadjuvant chemotherapy or radiation therapy before preoperative BSGI; and 2) diagnosed with distant metastasis in initial staging. The patients underwent mammography, ultrasonography, and MRI for the initial staging.
BSGI protocol
Patients underwent BSGI (Dilon 6800; Dilon Technologies, Newport News, VA, USA) at high-resolution and a small field-of-view. Imaging was performed 10 minutes after the intravenous injection of 99mTc-sestaMIBI (555 MBq; European Medicines Agency, London, UK) into a vein of the arm contralateral to the breast with the suspected lesion. The patients were in a seated position during the study. Craniocaudal (CC) and mediolateral oblique (MLO) images of both breasts were obtained. A low-energy, general purpose collimator was used, and the energy window was centered on 140 keV ± 10%. Planar images were acquired for 90,000 counts each, and the acquisition time for each image ranged from 5 to 8 minutes.
Imaging analysis and TBR measurement
The images were reviewed through a picture archiving and communication system (PACS). Two experienced nuclear medicine physicians analyzed the images and were blinded to the results of the other images and the tumor location, as determined by clinical examination.
Imaging sequences were divided into 5 categories according to the 2010 guidelines of the Breast Imaging Reporting and Data System (BIRADS) of the Society of Nuclear Medicine and Molecular Imaging (14). A score of 1 was assigned if there was evidence of diffuse uptake or an absence of focal uptake; a score of 2 was assigned if there was a benign finding with minimal, patchy uptake; a score of 3 was assigned if the finding was classified as probably benign with evidence of minimal, patchy uptake; a score of 4 was assigned if the finding was probably abnormal with minimal patchy and some focal uptake; and an abnormal finding with marked, focal uptake was assigned a score of 5. The incidence of abnormal, focally, increased uptake was determined by consensus between the 2 readers. Scores of 1, 2, and 3 were classified as a negative scan, and scores of 4 and 5 were classified as a positive scan.
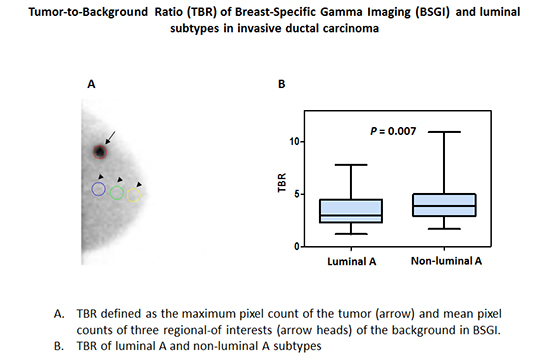
The TBR for each lesion was measured on BSGI. Focally increased uptake was selected as a target lesion. A circular region of interest (ROI) was drawn for each target lesion for the tumor uptake of MIBI. The maximum pixel value of ROI was measured as the tumor uptake of MIBI. The background uptake was measured as follows: 3 ROIs each measuring 2.0 cm in diameter were drawn so that the longitudinal axis was positioned in the breast parenchyma from right below nipple to the base of the breast parenchyma. The mean pixel value of each ROI was used to determine the background uptake of the breast lesion. TBR was calculated as the maximum pixel count of the tumor/mean pixel count of the background (Fig. 1). Images that showed higher tumor values between CC and MLO images were selected for the measurement of TBR.
Fig. 1
An example of measurement of a semi-quantitative index, TBR, in a 52-year-old woman with invasive ductal carcinoma. The left CC view shows the intense, focally increased uptake of the tumor measuring 2.2 cm in diameter. A ROI was marked on the tumor lesion, including the highest pixel value. The representation of 3 ROIs for the background was longitudinally drawn from the nipple to the base of the breast; the mean pixel counts were calculated.
TBR = tumor-to-background ratio, CC = craniocaudal, ROI = region of interest.

Pathologic diagnosis
The average interval between BSGI and surgical operation was 18 ± 8 days. We reviewed the histopathologic factors using an electric medical records system. The following parameters were retrieved from the pathologic report: tumor size, metastasis to an axillary lymph node; nuclear grade (NG); histologic grade (HG); Ki-67 index; and the expression profile of ER, PR, and human epidermal growth factor receptor 2 (HER2).
The patients enrolled in this study had unilateral breast cancer. Sixty-one patients had a single tumor, and 6 had multifocal tumors. For each of these multifocal cases, we only included one lesion with known tumor size and pathologic information. The pathologic tumor size was defined by the greatest diameter of the lesion. NG and HG were determined by the Bloom-Scarff-Richardson grading scheme. ER, PR, and HER2 expression was interpreted according to the guidelines of ER/PR/HER2 testing in breast cancer, as outlined by the American Society of Clinical Oncology/College of American Pathologists (15). ER and PR positivity were defined as the characterization of 1% or more of the tumor cells with an indication of nuclear positivity according to the Allred scoring system. Tumors were considered as HER2 positive if they received a score of 3+ based on immunohistochemistry (IHC). An IHC tumor score of 2+ warranted the fluorescent amplification of HER2 expression via in situ hybridization. The Ki-67 index was determined by IHC.
Tumors were categorized into 4 molecular subtypes (16): luminal A (ER positive and/or PR positive, HER2 negative, and Ki-67 < 14%), luminal B (ER positive and/or PR positive, HER2 negative, and Ki-67 ≥ 14%; or ER positive and/or PR positive and HER2 positive, irrespective of Ki-67 expression), HER2 positive (ER negative, PR negative, and HER2 positive), and triple negative (ER negative, PR negative, and HER2 negative).
Statistical analysis
All data are expressed as mean ± standard deviation (SD). Independent t-test for bimodal variables and analysis of variance (ANOVA) test for trimodal variables were used to compare the TBR of BSGI according to histologic subtype. Multiple regression analysis was performed using histologic factors; significant, independent factors were determined by P values less than 0.05 in the univariate analysis. The receiver-operating characteristic curve analysis was used to determine the diagnostic accuracy of TBR. The correlations between TBR and histopathologic factors were analyzed by Pearson's correlation coefficient. A correlation value (r) of 0.4 to 0.59 suggested a moderate positive correlation, and that below 0.4 was assessed as a weak positive correlation. Statistical analyses were performed using commercial software packages (SPSS version 19, IBM, Chicago, IL, USA; MedCalc version 14, MedCalc Software bvba, Ostend, Belgium), and P values less than 0.05 were regarded as statistically significant.
RESULTS
Patients and sensitivity
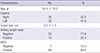
A total of 67 patients (age, 54.4 ± 10.0 years; ranging from 35 to 73 years) were included in this study. Patient characteristics are summarized in Table 1. The mean pathologic size of the tumor was 2.2 ± 1.5 cm, ranging from 0.5 to 10.2 cm. Of the 67 tumors, 60 (89.6%) were diagnosed as having a positive finding of BIRAD 4 or 5. There were 9 tumors less than 1 cm in diameter, of which 7 (77.8%, 7/9) were identified with a positive finding on BSGI, and their mean size was 0.7 cm, ranging from 0.5 to 0.9 cm. Among the 67 patients, metastatic axillary lymph nodes were detected in 15.
Comparison of TBR with prognostic factors
The image of BSGI was of satisfactory quality. In 60 tumors with BIRAD 4 or 5, the comparisons of TBR and prognostic factors are described in Table 2. A higher TBR value showed significant correlations with tumor size ≥ 2 cm, axillary lymph node metastasis, higher HG, negative PR status, and Ki-67 ≥ 14%. Among these variables, tumor size, axillary lymph node metastasis, and PR status were independently correlated with TBR in the multivariate analysis. Significant differences in TBR were not evident for NG, ER status, HER2 status, triple negative status, or subtype.
Table 2
The correlations between TBR and the histopathologic factors (n = 60)

TBR was not significantly correlated with the 4 subtypes of breast cancer (P = 0.102). However, it showed a significant difference between the luminal A subtype and non-luminal A subtypes (P = 0.007; Fig. 2). The mean TBR of luminal A subtype was 3.0 ± 1.2, while that of the non-luminal A subtype was 4.2 ± 1.9. For diagnosis of luminal A subtype, sensitivity and specificity of BSGI were 77.2% and 65.2%, respectively, at a TBR of 2.9
Fig. 2
The TBR of luminal A and non-luminal A subtypes of invasive ductal carcinoma. Bars represent the median value, and the whiskers represent the range of the 95% CI. The mean TBR of the luminal A subtype (3.0 ± 1.2) was lower than that of the non-luminal A subtype (4.2 ± 1.9), and significant correlation was evident between the 2 values (P = 0.007).
TBR = tumor-to-background ratio, CI = confidence interval.

Fig. 3 shows the correlations of TBR and histopathologic factors. The TBR had a weak correlation with tumor size (r = 0.374; P = 0.003), a weak negative correlation with the Allred score of PR status (r = −0.321; P = 0.013), and a moderately positive correlation with Ki-67 (r = 0.429; P = 0.001).
Fig. 3
Correlations between TBR and tumor size (A), Allred score of PR (B), and Ki-67 (C). TBR had a weak positive correlation with pathologic tumor size, a weak negative correlation with Allred score of PR, and a moderate positive correlation with Ki-67.
TBR = tumor-to-background ratio, PR = progesterone receptor.

Comparison of the positive and negative groups on BSGI
We compared the positive group with the negative group on BSGI. There was no difference between the 2 groups with regard to the following patient characteristics: age, histopathologic factors, and subtype. The mean size of the tumors with a positive finding on BSGI was 2.2 ± 1.6 cm, ranging from 0.5 to 10.2 cm; whereas tumors with a negative finding on BSGI had a mean size of 1.6 ± 0.8 cm, ranging from 0.7 to 3.1 cm. The mean background uptake (counts per pixel) in the positive and negative groups on BSGI was similar (86.9 ± 16.0 vs. 91.4 ± 37.7; P = 0.756). There were no significant differences between the 2 groups according to the histopathologic factors of the patients.
DISCUSSION
In this study, we compared a semi-quantitative parameter, TBR measured on BSGI, according to the prognostic factors of invasive ductal carcinoma. TBR showed a statistically significant difference in tumor size, axillary lymph node metastasis, expression profiles of PR, HG, and Ki-67 status. Furthermore, it showed a significant correlation with the luminal A and non-luminal A subtypes of breast cancer. Tumor size, axillary lymph node metastasis, and PR status were independent factors in the multivariate analysis.
The quantitative index of functional imaging in nuclear medicine has shown increasing favorability among clinicians for its use as a prognostic marker for lesion characterization and tumor response monitoring in cancer patients. For instance, the maximum standardized uptake value (SUVmax) is used as a prognostic factor in 18F-fluorodeoxyglucose (18F-FDG) positron emission tomography/computed tomography (PET/CT) and is measured using the voxel value with the maximum tumor uptake of FDG (1718). Likewise, the MIBI uptake of the tumor could also be used as a potential index as it has been an effective marker for the assessment of histologic type and grade and tumor proliferation (1920). However, despite the longevity of scintigraphy, it has not been well studied compared with 18F-FDG PET/CT. It is likely considered that the 2-dimensional imaging modality of scintigraphy provides less loco-regional information compared with anatomical imaging modalities such as breast ultrasonography or breast MRI. These are useful tools for more precise characterization of the tumor margins. However, they have certain limitations. Breast ultrasonography is a highly operator-dependent imaging modality, and breast MRI had a high false positive rate and the inability to identify calcifications or tiny calcium deposits. Consequently, these modalities could lead to unnecessary biopsies. The application of MRI, therefore, has been restricted for the diagnosis of breast cancer. Earlier studies have found that BSGI has higher specificity for discrimination of breast lesions compared to MRI (21). Therefore, BSGI can help reduce unnecessary breast biopsies.
In the present study, TBR was significantly correlated with the following poor prognostic factors: tumor size ≥ 2 cm, axillary lymph node metastasis, high HG, PR negative status, and high Ki-67 index (≥ 14%).
In concordance with our results, the correlation between TBR and only PR status, not ER status, was also reported in a previous study (12). The expression of PR is known to be dependent on estrogen and the end product of the estrogen-activated ER response. PR expression also represents a good response to endocrine therapy (22). Further studies are needed to elucidate the potential role of TBR on BSGI in response to endocrine therapy.
Related previous studies have reported that the TBR index has a predictive, prognostic value in breast cancer, whereas other studies have reported somewhat conflicting results. Cwikla et al. (12) concluded that the use of the TBR index in scintigraphy was correlated with tumor size, axillary lymph node metastasis, tumor grade, and PR status. A recent study using BSGI for patients with invasive breast cancer demonstrated that TBR showed differences in several prognostic factors including tumor size, NG, HG, and the expression profiles of ER/PR and HER2 (1011). In comparison with these studies, our study showed a discrepancy in that TBR did not show a difference according to NG or the expression profiles of ER and HER2. This discrepancy may have been attributable to the enrolled patient population. The previous study included 168 patients, larger than the sample in our study, and a tumor size below 1 cm was excluded to avoid a partial volume effect (11). In the present study, a tumor size below 1 cm was included to assess the diagnostic power of BSGI regardless of tumor size. Further study including a larger number of patients with wide distributions of tumor size is needed to resolve these discrepancies.
Intriguingly, another more conflicting study demonstrated that TBR differed according to tumor size and presence of lymph node metastasis, whereas it was not significantly correlated with the status of ER/PR, HER2, or Ki-67 (13). This discrepancy may have been attributable to the included tumor histology types and the definition of TBR. The previous study included several histology types such as ductal carcinoma in situ, invasive lobular carcinoma, and micropapillary carcinoma, as well as invasive ductal carcinoma. Moreover, the measurement of TBR was different from the method used in our study. The ROI was drawn on the tumor lesion and then placed on the breast parenchyma. The TBR was obtained as the total radioactivity count of the tumor lesion area divided by the corresponding count of the breast parenchyma. In our study, TBR was calculated from the maximum pixel value of a tumor and the mean of the background count of 3 ROIs serially obtained from the longitudinal axis from right below the nipple to the base of the breast parenchyma. The measurement of background count in the present study could reflect the diverse density of normal breast tissue in the patients. The differences in TBR calculation seemed to result in some discrepancy. As of yet, no measurement of TBR has been standardized, and more related studies are needed.
In accordance with our results, a previous study has reported that the MIBI uptake of the tumor was a potential index to classify invasive ductal breast cancer into 2 subtypes (luminal A and non-luminal A subtypes) (9). The TBR was significantly lower in luminal A type than in non-luminal A type. The luminal A type is the most common subtype and represents 50%–60% of all breast cancers. It is defined as ER positive and/or PR positive tumor with HER2 negativity and a low Ki-67 index. Patients with luminal A breast cancer are mainly treated with an endocrine hormone. They have a good prognosis, and the relapse rate is significantly lower than those of the other subtypes (23).
Previous studies have demonstrated that BSGI had a high sensitivity rate of 92%–96% and a specificity rate of 71%–80% in patients with breast cancer. These results were comparable to those reported for MRI. Our study reported 60 positive findings and 7 negative findings, as classified by the BIRAD score. No significant histopathologic factors between the 2 groups were found. The possible causes of false negativity include eccentric positioning of the tumor beyond the gamma camera's field-of-view, detection of a small tumor nodule measuring less than 1 cm in diameter, and dense breast. In the present study, 3 of the 7 negative findings were located in an eccentric area adjacent to the chest wall. Of these, 2 instances of small nodules measuring less than 1 cm in diameter were detected, measuring 0.7 and 0.8 cm, respectively. There were also 2 cases (patient age: 30 and 31 years, respectively), one patient with extremely dense breast tissue. Younger patients are more likely to have dense breast tissue, and this made it difficult to distinguish a mass from uneven uptake of the radioactive tracer in the breast tissue parenchyma. (24). One patient underwent bilateral reduction mammoplasty prior to the evaluation. As such, the increased uptake of MIBI along the surface margins of the implant was interpreted as a post-operative change; therefore, the presence of mass was indistinguishable from the implant. Thus, a comparison of the histopathological factors of the positive and negative groups showed no significant differences.
There were some limitations in the present study. Firstly, this study was retrospectively designed and involved only a small number of patients from a single institution. Additionally, diagnostic biopsies before BSGI were performed in 49 patients (73%); this might have affected the properties of the images. In these cases, the interval time between BSGI imaging and diagnostic biopsy averaged 10.9 days. At our hospital, BSGI was performed after at least one week from the date of the biopsy to prevent the occurrence of biopsy-related artifacts. Further studies with a larger cohort sample and systemic study designs are warranted.
In conclusion, a high TBR value on BSGI was significantly correlated with poor prognostic factors of breast cancer. Luminal A subtype, a breast cancer subtype with more favorable prognosis, was associated with a low value of TBR on BSGI.
 XML Download
XML Download